
Abstract
Extrahepatic biliary atresia (EHBA) is a leading cause of neonatal cholestasis, often resulting in end-stage cirrhosis and portal hypertension without early diagnosis and treatment. This report highlights the importance of timely intervention, describing a 6-day-old male newborn diagnosed with EHBA who underwent successful Kasai portoenterostomy at 9 days of age. While the procedure is typically performed within the first 60 days of life, this exceptionally early intervention led to significantly improved outcomes. Postoperative recovery was marked by bilirubin normalization within 2 months and steady improvement in liver function tests, demonstrating the advantages of early surgery. The procedure involved creating a Roux-en-Y hepatic portojejunostomy to restore bile flow, preventing progression to biliary cirrhosis. Early intervention achieved effective bile drainage and substantial clinical improvement. At the 1-year follow-up, the infant displayed normal growth and liver function. This case supports the hypothesis that performing Kasai portoenterostomy earlier than current guidelines recommend may lead to better outcomes. It underscores the need for vigilant neonatal care to recognize early signs of cholestasis and enable prompt surgical intervention. Early diagnosis and intervention can preserve liver function, potentially delaying or preventing the need for liver transplantation.
Keywords
Introduction
Extrahepatic biliary atresia (EHBA), although rare, is the leading cause of neonatal and infantile cholestasis, accounting for up to 30% of cholestasis cases requiring surgical intervention in infants. It remains the primary indication for liver transplantation (LT) in children. EHBA is characterized by progressive scarring and obstruction of the intrahepatic and extrahepatic biliary ducts. 1
Without early surgical correction, secondary biliary cirrhosis, hepatocellular failure, portal hypertension, and death are inevitable before the age of 2 years. 2 Hepatic portoenterostomy (HPE), also known as Kasai portoenterostomy (KP), should ideally be performed before 8 weeks of age to achieve optimal outcomes. Although this procedure is not definitive, it delays LT and allows the patient to live with their native liver for a longer period. Native liver survival varies among patients and is significantly influenced by the timing of the operation, with earlier intervention yielding better outcomes. 2
Failure to achieve adequate bile flow after the Kasai procedure, or continued liver deterioration, growth retardation, or advanced cirrhosis, necessitates LT as the only solution. 3
We herein describe a very young newborn with EHBA who underwent successful Kasai HPE at 9 days of age, consistent with the cases reported by Makin et al. 4 in 2009 suggesting that liver injury might be present at birth.
Case presentation
A male newborn was delivered by Cesarean section to a non-consanguineous, healthy Egyptian couple. He was admitted to the neonatal intensive care unit (NICU) for respiratory distress, which was diagnosed as transient tachypnea of the newborn. At 4 days of age, jaundice was observed (Figure 1), along with deeply staining urine and clay-colored stools (Figure 2), raising suspicion of EHBA at an unusually early age. While EHBA typically manifests in early infancy, a diagnosis at just 4 days of age has not been previously reported.

Four-day-old neonate with jaundiced sclera.
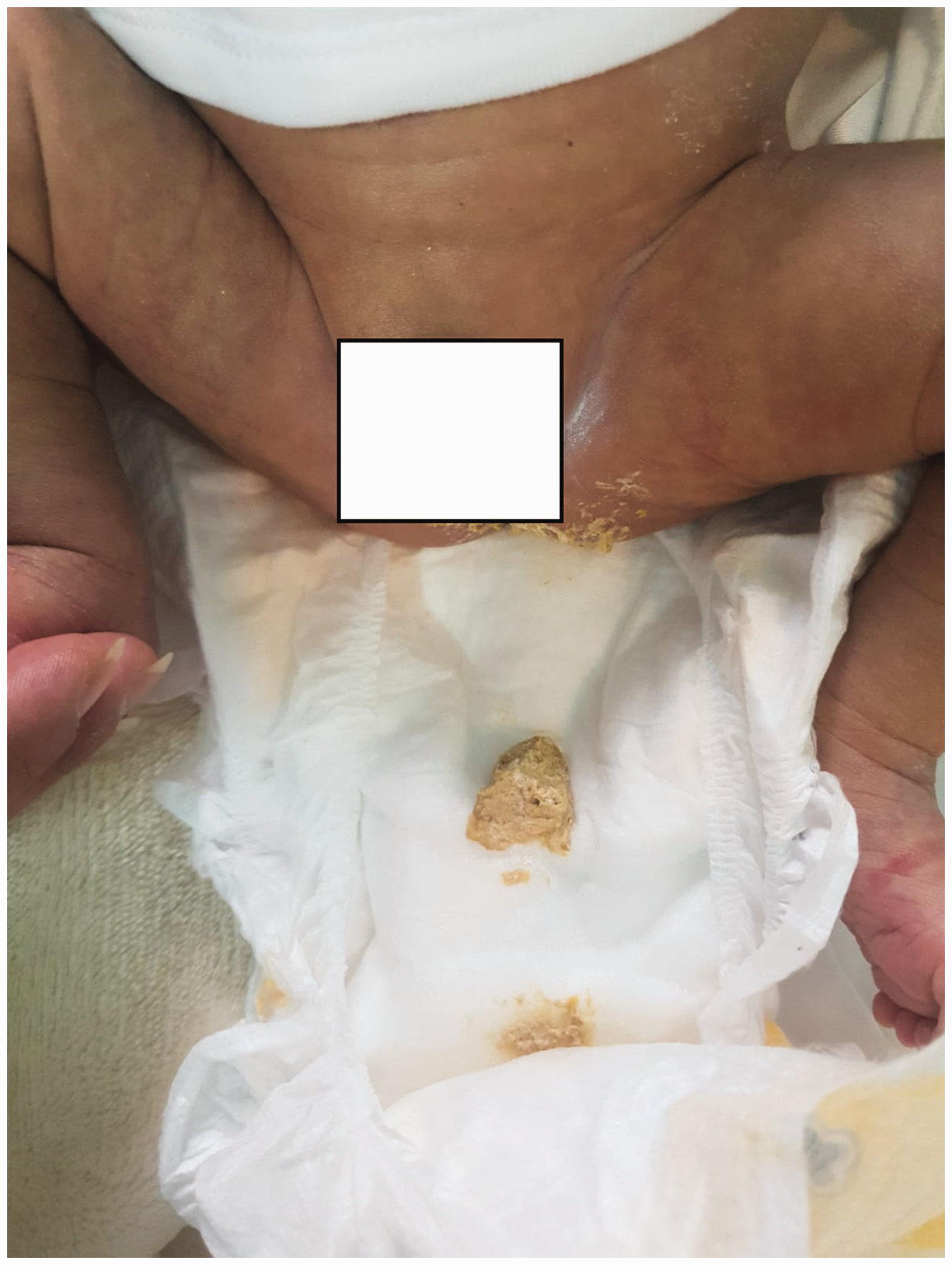
Clay-colored stool at 4 days of age.
The newborn’s birth weight, length, and head circumference were at the 50th percentile. Abdominal examination and systemic reviews were unremarkable, and ophthalmologic assessment was normal.
Laboratory investigations revealed elevated total serum bilirubin of 12.5 mg/dL (reference range, 0.5–1.2) and direct bilirubin of 7 mg/dL (reference range, 0.1–0.2). Gamma-glutamyl transpeptidase (GGT) was markedly elevated at 1842 U/L (reference range, 35–151), further supporting the diagnosis. The alanine aminotransferase and aspartate aminotransferase levels were 32 U/L (20–40) and 90 U/L (20–40), respectively. The coagulation profile was normal (prothrombin time: 12.2 seconds, partial thromboplastin time: 42.1 seconds, and international normalized ratio: 1). There was no clinical or laboratory evidence of infection, sepsis, hemolysis, or endocrine insufficiency. Metabolic screening was normal, and an echocardiogram showed a hemodynamically insignificant small patent foramen ovale and small patent ductus arteriosus.
Abdominal ultrasound revealed a normal-sized liver and spleen, but the gallbladder was small and contracted, with no detectable changes in size or contractility in pre- and post-prandial ultrasound films. This further supported the diagnosis of EHBA.
The pediatric surgeon recommended urgent laparotomy with intraoperative cholangiography to confirm EHBA, proceeding to KP if indicated. The urgency of the procedure and its potential benefits were thoroughly discussed with the parents, who provided written informed consent for the operation. At 9 days of age, the patient underwent surgery. Because of the severely atretic extrahepatic biliary tree and a small, atretic gallbladder, intraoperative cholangiography could not be performed, and a standard KP was completed. Figure 3(a) to (d) illustrates the surgical steps.
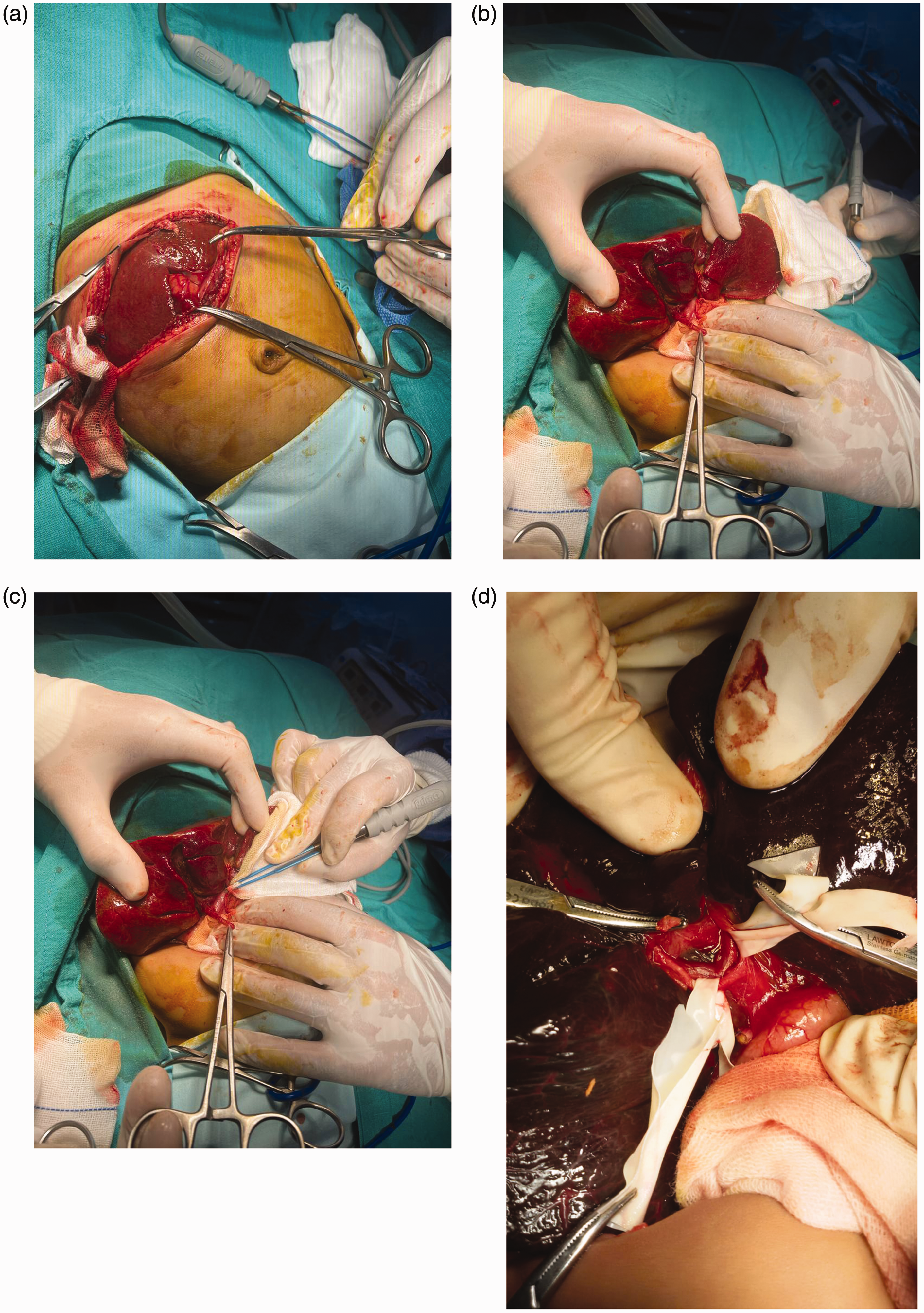
Surgical steps of Kasai portoenterostomy. (a) Right upper quadrant muscle-cutting incision with mobilization of the liver by division of the falciform ligament. (b, c) The liver was elevated outside the abdominal cavity, showing mobilization of the gallbladder and exposure of the porta hepatis. The liver appeared healthy due to early recognition and intervention and (d) Exposure and dissection of the porta hepatis.
The immediate postoperative course was complicated by cardiorespiratory instability, requiring a 5-day NICU stay for stabilization. Within 48 hours of surgery, the stools changed to yellow (Figure 4(a)), becoming a deeper yellow-green color 1 week later (Figure 4(b)). After discharge from the NICU, his jaundice gradually resolved, and serum total and direct bilirubin levels normalized by 2 months of age.
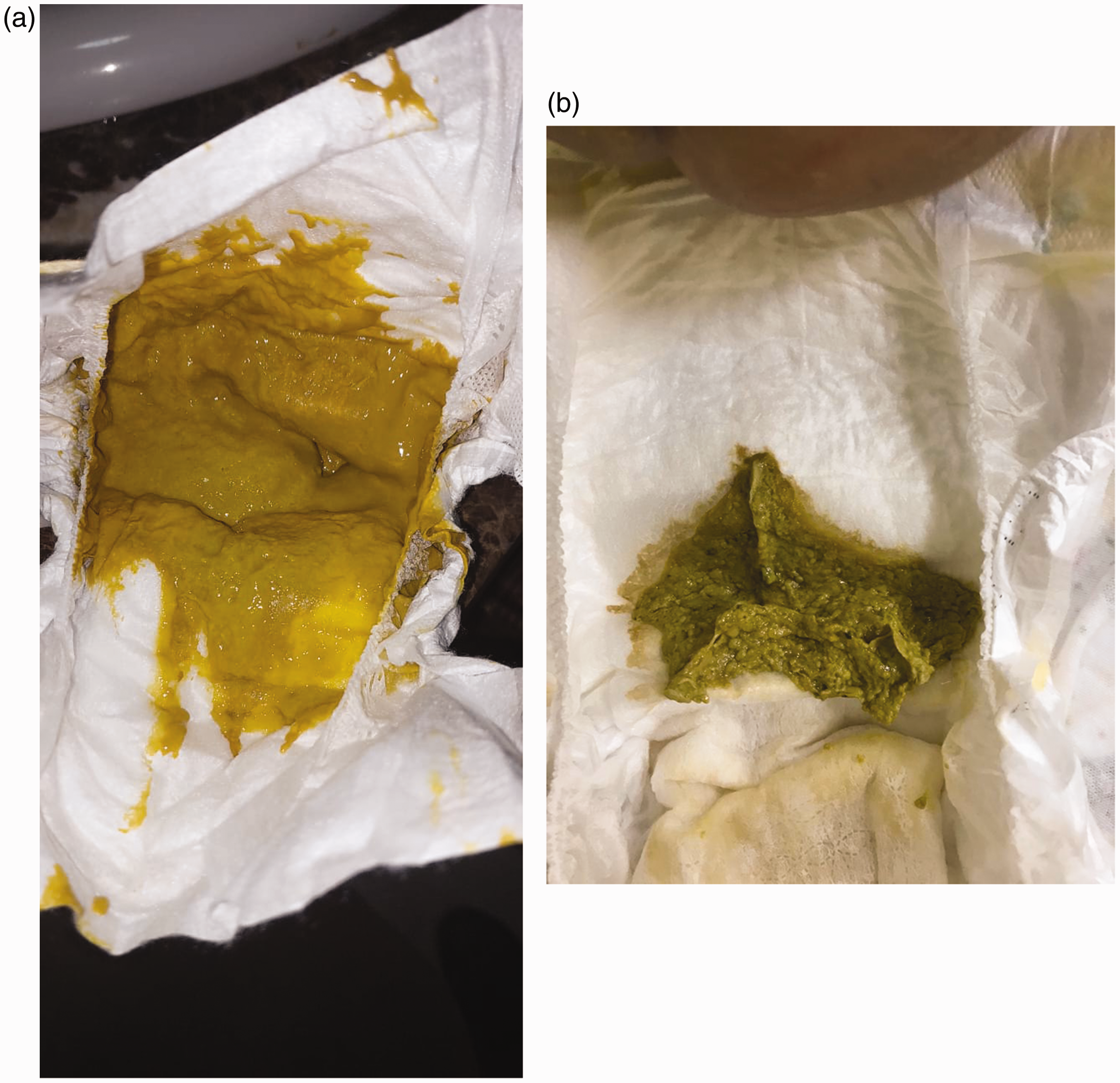
Stool color changes post-Kasai portoenterostomy indicating successful bile drainage. (a) Colored stool 48 hours postoperatively and (b) More deeply colored stool 7 days postoperatively.
At 15 months, the patient remained jaundice-free, with a mildly enlarged liver but no splenomegaly. Laboratory tests showed normal bilirubin levels, liver transaminases, and coagulation profiles. He was growing well with no reported episodes of cholangitis.
A strict follow-up plan was implemented to monitor the long-term effects of this exceptionally early Kasai intervention on the patient’s native liver function and to assess the potential for avoiding later LT.
Discussion
To the best of our knowledge, this is the youngest reported newborn clinically diagnosed and operated on for EHBA in the English literature. Makin et al. 4 reported a newborn among their cohort of three patients, who underwent surgery for intestinal obstruction as early as 24 hours after birth. That newborn presented with dysmorphic facies, including mandibular hypoplasia, cleft lip and palate, high rectal atresia, rectovaginal fistula, bilateral hydronephrosis, and only four digits on one hand. The newborn underwent surgery for jejunal and colonic atresia and malrotation. 4 During the procedure, the jejunal content was noted to be acholic, and further dissection revealed an absent gallbladder consistent with type III biliary atresia. A primary jejunal anastomosis, colostomy, and KP were performed. 4 Although bile flow was initially observed, recurrent sepsis episodes led to end-stage liver disease and death at 48 months of age. 4
By contrast, our patient was diagnosed and operated on based solely on clinical findings and a workup strongly suggestive of EHBA. He was an otherwise normal newborn, with no dysmorphic features or congenital anomalies. Postoperative bile flow was successfully established, and at 15 months of age, the patient remained jaundice-free with normal liver function and growth parameters confirmed by clinical examination and laboratory evaluations. This case underscores the potential for successful outcomes with extremely early diagnosis and surgical intervention, even in the absence of associated anomalies. It highlights the importance of vigilant clinical observation and prompt management to optimize prognosis in EHBA.
EHBA is a significant cause of cholestatic liver disease in infants. Without early identification and intervention, it progresses to secondary biliary cirrhosis, end-stage liver disease, and portal hypertension. 5 A hallmark feature of EHBA is pale or clay-colored stool, which serves as a critical marker for early diagnosis. 6 Effective management of EHBA relies on prompt detection and timely surgical intervention, emphasizing the need for caregivers and physicians to be vigilant in recognizing early symptoms. 6 At our center, the use of stool color cards, along with measurements of serum conjugated bilirubin and GGT levels in newborns with persistent jaundice beyond 14 days, has significantly enhanced early EHBA detection. These diagnostic tools underscore the importance of systematic screening in improving outcomes. 7 However, this case is exceptional because the newborn was admitted to the NICU and promptly investigated and treated immediately after birth, allowing for surgical intervention at an unusually early age.
KP aims to re-establish bile flow from the liver to the intestine, preventing rapid progression to secondary biliary cirrhosis. The procedure involves creating an enterostomy approximately 10 cm beyond the Treitz ligament, forming a Roux-en-Y hepatic portojejunostomy. The distal segment of the jejunum is brought to the porta hepatis and connected to the cut surface of the fibrous mass at the porta hepatis through an anastomosis. The proximal section is then attached to the side of the jejunum approximately 45 cm beyond the Treitz ligament. 8 This case highlights the critical impact of early detection and intervention in achieving favorable outcomes for EHBA, demonstrating the effectiveness of systematic diagnostic approaches and prompt surgical management. 8
Since its development in the late 1950s, KP has undergone significant advancements in surgical techniques and postoperative care, all aimed at optimizing patient outcomes. 8 Among the key factors influencing the success of KP, the age at which the procedure is performed has been a central focus of research. 9 Early observations by Morio Kasai indicated that performing KP before 60 days of age improves bile drainage, a finding supported by numerous subsequent studies. Nevertheless, the question of optimal timing remains, as researchers continue to explore how surgical timing impacts recovery. 8
In the Middle East, the reported average age at which KP is performed is approximately 56 days. 8 Similarly, a recent survey by the Quality-of-Care Task Force of ESPGHAN, published in February 2024, revealed that despite efforts to reduce the age at KP to less than 30 days, the median age in Europe has remained around 60 days for decades. 9 Alarmingly, approximately 6% of cases in the survey were ineligible for surgery because of advanced cirrhosis and late referrals. 9 Although stool color cards have demonstrated potential in reducing the age at KP, adherence to screening protocols across Europe remains inconsistent, highlighting the need for increased awareness and adherence to guidelines. 9
The rapid bile drainage observed in our patient within 2 days and normalization of bilirubin levels in less than 2 months suggests that much earlier intervention may be beneficial than previously thought.
We also emphasize the role of artificial intelligence models in the early and precise diagnosis of EHBA, which can optimize patient outcomes. 10 In 2020, Liu et al. 11 demonstrated the potential of an artificial neural network (ANN) model as a non-invasive, efficient diagnostic tool for accurately diagnosing EHBA. The model analyzes 46 clinical parameters from patients with obstructive jaundice, including total bilirubin, direct bilirubin, and GGT levels. The ANN model achieved a high sensitivity of 97.2% and specificity of 91.0%, showcasing its effectiveness. 11
This advancement in diagnostic methodology aligns with our case’s central principle: the critical importance of early diagnosis for the successful management of EHBA. Liu et al. 11 advocate for integrating advanced diagnostic models such as ANN into clinical practice. These tools offer a non-invasive, efficient, and highly accurate approach to EHBA diagnosis, potentially reducing the diagnostic window and enabling timely interventions such as KP. This is particularly relevant to our case, which represents the youngest patient with EHBA to undergo surgery at just 9 days of age. 11
The incorporation of ANN-based diagnostic tools could revolutionize the early detection of EHBA by complementing traditional diagnostic methods and facilitating optimal timing for interventions. Our case, along with the findings reported by Liu et al., 11 highlights the evolving landscape of EHBA diagnosis and management, emphasizing the transformative potential of artificial intelligence in pediatric surgery and the paramount importance of early intervention.
Conclusions
To the best of our knowledge, this case represents the youngest reported newborn to undergo surgery for EHBA in the English-language literature. The prompt diagnosis and successful KP, leading to normalization of stool color, underscore the critical importance of early detection and timely intervention in EHBA to prevent irreversible liver damage and improve long-term outcomes. Early KP is strongly associated with improved jaundice clearance and enhanced long-term survival.
The timing of diagnosis and referral is heavily influenced by healthcare systems, highlighting the need for structured guidelines and targeted awareness campaigns. Prospective studies are crucial to identify barriers to early detection of biliary atresia and to promote adherence to early intervention protocols. Future research should focus on determining how surgical intervention can be performed at even earlier stages to optimize prognosis for patients with EHBA. These findings would contribute to building a stronger foundation for future treatment protocols and improving overall patient outcomes.
Declarations
The reporting of this study conforms to the CARE guidelines.
12
All patient’s details were de-identified. The patient’s parents provided written informed consent for performance of the surgical intervention and publication of the report. Availability of data and materials: All data and materials related to the study are included in the current manuscript. Ethics approval: In accordance with our institution’s regulations, the requirement for ethics approval was waived because no new treatment or procedure was used in this case.
Footnotes
Acknowledgments
We thank our patient and his family.
Authors’ contributions
ME, GE: Conceptualization, supervision, validation, methodology
ME, GE, MQ: Data curation.
ME, GE, MQ, NK, MO, NA, SA: Formal analysis.
ME, NK: Writing — Original draft preparation.
ME, GE, NK, MQ, MO, NA, AA, SA: Writing — Review & editing.
Declaration of conflicting interests
All authors declare no conflict of interest related to the study.
Funding
No funds were received for the current work.