
Abstract
Objective
To evaluate the effect of preoperative intravenous mannitol on the capsulorhexis process and intraoperative complications in patients with primary angle-closure glaucoma (PACG).
Methods
In this prospective randomized controlled trial, 65 PACG eyes were randomized into the mannitol and control groups. The capsulorhexis duration, number of forceps grasps, need for viscoelastic re-injection, and intraoperative complications were recorded.
Results
The mannitol group had a significantly shorter capsulorhexis duration and fewer forceps grasps of the capsule. All intraoperative complications (18.2%) occurred in the control group. The patients with intraoperative complications had significantly higher intraocular pressure and lower best-corrected visual acuity than those without complications after surgery. Multivariate analysis found that intravenous mannitol (odds ratio [OR] = −14.263; 95% confidence interval [CI] =−26.713 to −1.813) reduced the capsulorhexis duration, whereas zonulopathy (OR = 14.477, 95% CI = 2.622–26.331) prolonged the duration.
Conclusion
Preoperative intravenous mannitol can reduce the risk of intraoperative complications and improve postoperative outcomes in patients with PACG. Factors including anterior chamber depth, incision location and method, and the zonule status significantly influence the capsulorhexis process.
Keywords
Introduction
Primary angle-closure disease (PACD) comprises a spectrum of conditions characterized by the closure of the anterior chamber angle, potentially leading to elevated intraocular pressure (IOP) and/or optic neuropathy, resulting in irreversible vision impairment and blindness globally. 1 It encompasses primary angle-closure suspect (PACS), primary angle closure (PAC), and primary angle-closure glaucoma (PACG). The prevalence of PACG is highest in Asia, especially in China, with 87% of all global cases occurring in Asia. 2
The management of PACD incorporates a variety of interventions, including medical, laser, and surgical treatments. The primary objectives of these treatments are to widen the anterior chamber angle and effectively reduce IOP. The surgical procedures include trabeculectomy, lens extraction with or without goniosynechialysis, and a combined approach involving cataract and filtering surgery. 3 Lens extraction with goniosynechialysis can widen the angle and lower both IOP and the requirement for glaucoma medications. 4 However, it is crucial to note that pupil dilation prior to surgery can potentially trigger angle closure attacks.
Hypertonic mannitol, a hyperosmotic agent, can decrease both intracranial pressure and IOP by reducing the volume of the vitreous humor. 5 This is particularly relevant when performing capsulorhexis, in which anterior chamber shallowness and elevated IOP can increase the risk of intraoperative complications, such as capsulorhexis tears, zonular instability, and iris prolapse.6,7 Although mannitol has been used in phacoemulsification and intraocular lens (IOL) implantation procedures for patients with PACD, 8 its effects, particularly in relation to the capsulorhexis process and the risk of intraoperative complications, have not been thoroughly studied. The objective of this study was to evaluate the impact of preoperative use of intravenous mannitol on the process of capsulorhexis and intraoperative complications during phacoemulsification and IOL implantation combined with goniosynechialysis in patients with PACD.
Materials and methods
Subjects
This prospective, randomized, controlled study enrolled Chinese subjects diagnosed with PACD. The study was approved by the Ethics Committee of Peking University People’s Hospital (approval number: 2022PHB256-001) and followed the tenets of the Declaration of Helsinki. Additionally, we have adhered to the CONSORT reporting guidelines to ensure the clarity and completeness of our trial report. The protocol is prospectively registered at www.clinicaltrials.gov (registration number: NCT05563623). Written informed consent was obtained from every subject. Patients with PACD were recruited from the glaucoma clinic of Peking University People’s Hospital between September 2022 and June 2023. The participants were randomly allocated to the mannitol or control group using a computer-generated random number table. The sequence of randomization was carefully concealed in sealed, opaque envelopes that were prepared in advance and opened only by a nurse who was not involved in the study’s procedures or assessments. The labeling ensured that the nature of the infusion was indistinguishable to the study participants, surgeons, and outcome assessors. Throughout the study, the surgeons performing the procedures, the patients undergoing treatment, and the outcome assessors evaluating the results remained blinded to the group allocations to prevent bias. This blinding process was maintained rigorously from randomization through to the final assessment, ensuring the integrity of the study.
According to the International Society of Geography and Epidemiology of Ophthalmology (ISGEO) classification system, 9 all eyes included in this study were classified as having PACS, PAC, or PACG. An eye was defined as having PACS if there was a potential appositional contact between the peripheral iris and the posterior trabecular meshwork. An eye was classified as having PAC if it exhibited iridotrabecular contact, elevated IOP, or peripheral anterior synechia (PAS) without a secondary cause for the PAS and it lacked glaucomatous optic neuropathy. An eye was defined as having PACG if it displayed features of PAC in conjunction with glaucomatous optic neuropathy.
The exclusion criteria were as follows: history of ocular conditions that could potentially lead to secondary angle closure, such as ocular trauma, iris neovascularization, tumor, uveitis, and lens intumescence; prior intraocular surgery, including vitrectomy with silicone or inert gas, or prior laser peripheral iridotomy; medical conditions that could complicate intravenous mannitol administration, such as cardiac or renal diseases; preoperative IOP exceeding 24 mmHg with medication; preoperative slit lamp examination or ultrasound biomicroscopy (UBM) examination revealing lens subluxation; and difficulty in making an accurate diagnosis based on the patients’ medical history, symptoms, and clinical signs.
Ophthalmologic examinations
All participants underwent a comprehensive ocular examination including best-corrected visual acuity (BCVA), IOP measurement via Goldmann applanation tonometry (Haag-Streit, Koniz, Switzerland), detailed slit-lamp biomicroscopy, and stereoscopic evaluation of the optic disc using a 90-diopter lens (Volk Optical, Inc., Mentor, OH, USA). A glaucoma specialist (HJW) performed gonioscopy in a dimly lit room using a Goldmann-style four-mirror gonioscopy lens (Model G-4, Volk Optical, Inc.) at 16× magnification, both with and without indentation, to evaluate the presence of PAS. Five IOLMaster (ZEISS, Oberkochen, Germany) measurements were taken to determine axial length, the average of which was used for analysis. Optical coherence tomography (Spectralis HRA + OCT, Heidelberg Engineering GmbH, Heidelberg, Germany) was employed to detect retinal nerve fiber layer defects, and a visual field test (Humphrey Field Analyzer, ZEISS) was conducted to identify characteristic glaucomatous visual field defects. UBM measurements (Aviso, Quantel Medical, Inc., Bozeman, MT, USA) were performed using a 50-MHz transducer by a well-trained operator who was blinded to the clinical data. All patients underwent UBM in a supine position in a lit room. The findings from UBM were not analyzed or included in the results section because they were primarily used to confirm the diagnosis and eliminate secondary conditions.
BCVA and IOP were also recorded 1 day, 1 month, and 3 months after surgery.
Therapeutic methods
For all enrolled patients, oral acetazolamide was discontinued 3 days before surgery to eliminate any potential influence on the study outcomes. IOP was managed using only topical medications during this period to ensure consistency in preoperative IOP control. Patients in the mannitol group received a 250-mL infusion of 20% mannitol to decrease IOP 1 hour prior to surgery. This was followed by six instillations of 0.5% tropicamide eye drops (Santen Pharmaceutical Co., Ltd., Osaka, Japan) at 5-minute intervals for pupil dilation. In the control group, patients received a 250-mL infusion of normal saline, followed by six instillations of 0.5% tropicamide eye drops (one application every 5 minutes) starting 30 minutes before the procedure. All surgeries were performed by two experienced surgeons (HJW and XRH), with the same technician responsible for preoperative and postoperative measurements. Both groups underwent phacoemulsification and IOL implantation combined with visco-goniosynechialysis. Following topical anesthesia with oxybuprocaine, the main incision was made. Subsequently, around 0.2 mL of sodium hyaluronate (Iviz, Bausch & Lomb Incorporated, Laval, Canada) were injected as a viscoelastic agent into the anterior chamber to facilitate a continuous curvilinear capsulorhexis. Capsulorhexis was initiated through the main incision of the lens capsule with forceps (66 Vision Tech Co., Ltd., Glen Burnie, MD, USA) and extended counterclockwise. Physiological saline was used for hydrodissection, and a phacoemulsification device was employed to emulsify the lens nucleus. The irrigation/aspiration system was used to remove the residual cortex. The iris root was pushed back 360° along the angle with sodium hyaluronate, and angle adhesions were separated twice. A hydrophobic acrylic IOL (Abbott Medical Optics Inc., Santa Ana, CA, USA) of appropriate size and power was inserted into the capsule. After this, remnants such as the viscoelastic agent were removed, and the incision was hydrated and checked for aqueous humor leakage. Finally, the eye was covered with sterile gauze.
Surgical videos were recorded for all patients, and several items were documented according to the intraoperative situation and surgical video. First, for capsulorhexis, the duration of capsulorhexis, the number of times the forceps grabbed the capsule, and the need for re-injection of the viscoelastic agent were recorded. The duration of capsulorhexis was defined as the time from the initial insertion to the final withdrawal of the forceps through the incision. Regarding intraoperative complications, any complications that occurred during the operation, such as acute infusion fluid misdirection (malignant glaucoma), posterior capsular rupture, anterior capsular tear, iris prolapse, inadvertent propagation of a capsule tear, and zonulysis, were recorded. For zonulopathy, signs of zonulopathy, such as anterior capsule wrinkling, instability of the capsular bag, and deviation of the capsulorhexis after intraocular implantation, were recorded. All surgical information was determined intraoperatively by the surgeon (HJW and XRH) and confirmed post-operatively by the blinded investigators (ZQL).
Sample size calculation
The sample size for this randomized controlled trial was determined according to the primary outcome of the difference in the duration of capsulorhexis between the mannitol and control groups. A preliminary pilot study indicated that the standard deviation of capsulorhexis duration was approximately 30 s. To detect a clinically significant difference of 15 s between the two groups with an effect size of 0.5, alpha of 0.05, and power of 80%, a sample size calculation was performed using a two-sided two-sample t-test. Based on these values, the calculation yielded a sample size of approximately 30 patients per group. To account for potential dropouts and non-compliance, a 10% increase was included, leading to a final sample size of 32 or 33 patients per group. This sample size was deemed appropriate for achieving the study objectives while considering practical constraints and ensuring the study’s feasibility.
Statistical analysis
Data analysis was performed using IBM SPSS 22.0 software (IBM Corp., Armonk, NY, USA). All data were calculated to obtain the mean ± standard deviation. The distribution of the data was validated by the Shapiro–Wilk test, which demonstrated that certain quantitative parameters (age, anterior chamber depth, lens thickness, and white-to-white distance) followed a normal distribution. Therefore, a parametric test (Student’s t-test) was used for normally distributed data, whereas a non-parametric test (Mann–Whitney U test) as applied to non-normally distributed data because of its robustness in handling non-normally distributed datasets. Fisher’s exact test was used to assess sex and the necessity for re-injection of the viscoelastic agent. Furthermore, we performed univariate and multivariate regression to determine parameters associated with the duration of capsulorhexis, the number of times the forceps grabbed the capsule, and the need for re-injection of the viscoelastic agent. Missing data were minimal and handled using a complete-case analysis approach. P < 0.05 was considered statistically significant.
Results
Demographics, clinical characteristics, and preoperative data
In total, 65 eyes in 65 patients (16 with PACS, 27 with PAC, and 22 with PACG) treated between November 2021 and February 2023 were enrolled in the final analysis. The study randomly assigned 32 eyes to the mannitol group and 33 eyes to the control group. Figure 1 presents the CONSORT flow diagram, summarizing the enrollment, exclusions, and allocation of participants. Table 1 summarizes the demographic and clinical characteristics and capsulorhexis process of the patients. The mean patient age was 68.74 ± 7.33 years. The cohort included 23 men and 42 women. The mean preoperative BCVA was 0.36 ± 0.25. The mean preoperative IOP was 17.11 ± 5.83 mmHg on IOP-lowering medications. The duration of capsulorhexis was significantly shorter in the mannitol group than in the control group (P < 0.001). The number of times the forceps grabbed the capsule was significantly lower in the mannitol group than in the control group (P = 0.025). No statistical differences were identified between the two groups in terms of age, sex, diagnosis, BCVA, IOP, axial length, anterior chamber depth, lens thickness, the white-to-white distance, and the need for viscoelastic re-injection (all P > 0.05).

CONSORT flow diagram in this randomized controlled trial.
Comparison of demographic and clinical characteristics and the capsulorhexis process between the mannitol and control groups.

PACS, primary angle-closure suspect; PAC, primary angle-closure; PACG, primary angle-closure glaucoma; BCVA, best-corrected visual acuity; IOP, intraocular pressure; ACD, anterior chamber depth.
Intraoperative findings
Phacoemulsification and IOL implantation combined with visco-goniosynechialysis surgery were performed in 65 eyes with PACD. Zonulopathy was observed during the operation in 32 eyes (49.2%). Six eyes (18.2%) in the control group experienced intraoperative complications, including acute infusion fluid misdirection (malignant glaucoma), posterior capsule rupture, iris prolapse, inadvertent propagation of a capsule tear, and zonulysis during phacoemulsification in two, one, one, one, and one eye, respectively. No intraoperative complications were encountered in the mannitol Group.
Notably, there were no significant differences in the baseline BCVA and IOP between the groups with and without complications (P > 0.05). The analysis demonstrated significant differences in both BCVA and IOP at the first day postoperatively, IOP at 1 month post-operatively, and both BCVA and IOP at 3 months postoperatively between the two groups (all P < 0.05; Figure 2).
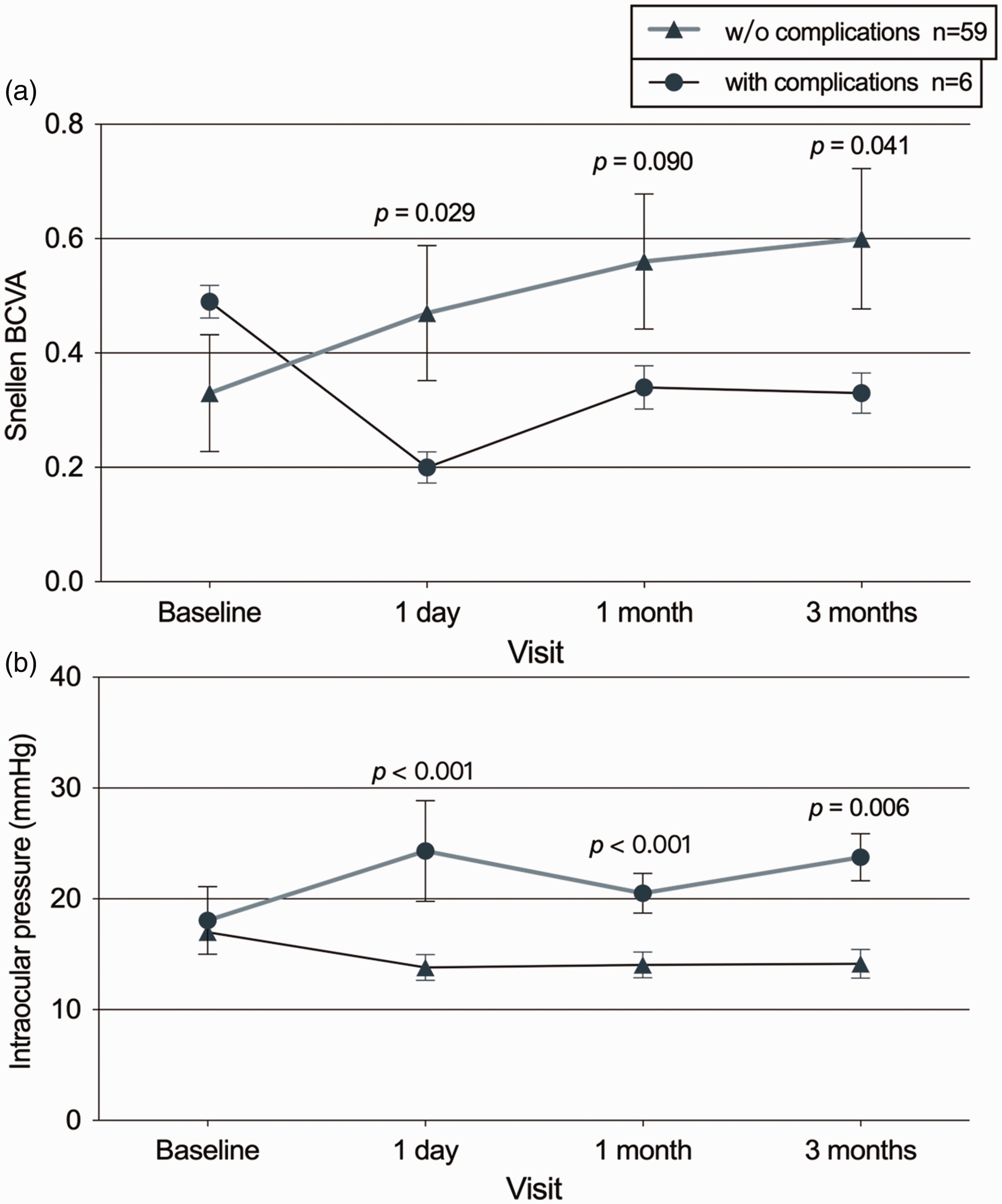
Serial changes of BCVA and IOP from baseline at each follow-up in patients with and without complications. (a) Serial BCVA from baseline at each follow-up in the between-group comparison and (b) Serial IOP from baseline at each follow-up in the between-group comparison. BCVA, best-corrected visual acuity; IOP, intraocular pressure.
Factors associated with the capsulorhexis process
Multivariate regressions analyses were performed to determine the factors associated with capsulorhexis. Intravenous mannitol significantly shortened the duration of capsulorhexis (odds ratio [OR] = −14.263; 95% confidence interval [CI] = −26.713 to −1.813; P = 0.026), whereas zonulopathy significantly increased the duration of capsulorhexis (OR = 14.477, 95% CI = 2.622–26.331; P = 0.018; Table 2). The number of times the forceps grabbed the capsule and the need for re-supplementation of the viscoelastic agent were not associated with the duration of capsulorhexis.
Regression analysis of determinants associated with the duration of capsulorhexis.

ACD, anterior chamber depth; OR, odds ratio; CI, confidence interval.
Subgroup analysis
We conducted a subgroup analysis based on the ISGEO classification and divided the eyes into two groups: PACS group (16 eyes) and PAC + PACG group (49 eyes). In the PACS group, seven eyes received intravenous mannitol. The duration of capsulorhexis was significantly shorter in the mannitol group than in the control group (P = 0.029). Posterior capsule rupture during surgery occurred in one eye (6.3%) in the control group (Table 3). In the PAC + PACG group, 25 eyes received intravenous mannitol. The mannitol group also exhibited a significantly shorter duration of capsulorhexis than the control group (P = 0.003). The control group displayed a higher likelihood of requiring re-injection of the viscoelastic agent than the mannitol group (P = 0.023). Intraoperative complications were observed in five eyes (10.2%) in the control group, including two cases of acute infusion fluid misdirection, one case of iris prolapse, one case of inadvertent propagation of a capsule tear, and one case of zonulysis during phacoemulsification (Table 3). For the cases of acute infusion fluid misdirection, irrigation was temporarily paused, and anterior chamber reformation was performed to resolve the issue. Iris prolapse was managed by carefully repositioning the iris with a viscoelastic agent and maintaining a stable anterior chamber throughout the procedure. Zonulysis, detected during phacoemulsification, was stabilized using a capsular tension ring to support the lens capsule and ensure safe IOL implantation. By contrast, no intraoperative complications were reported in the mannitol group.
Comparison of demographic, clinical characteristics, capsulorhexis process, and intraoperative complications between the mannitol and control groups of PACS and PAC + PACG eyes.

PACS, primary angle-closure suspect; PAC, primary angle-closure; BCVA, best-corrected visual acuity; IOP, intraocular pressure; ACD, anterior chamber depth.
Discussion
In the therapeutic landscape for patients with PACD and cataract, one of the most efficacious strategies is the combination of phacoemulsification and IOL implantation accompanied by goniosynechialysis.10,11 However, for patients with crowded anterior chamber structures, preoperative pupillary dilation carries a certain degree of risk. Intravenous mannitol is employed by many glaucoma surgeons as a preoperative agent to reduce IOP by causing vitreous dehydration.12,13 The findings of the current study revealed that the preoperative intravenous administration of mannitol could shorten the duration of capsulorhexis and effectively prevent intraoperative complications such as acute infusion fluid misdirection, posterior capsular rupture, anterior capsular tear, iris prolapse, and zonulysis. Furthermore, multivariate regression confirmed that the capsulorhexis process can be influenced by factors such as the preoperative administration of mannitol and status of the zonules.
Mannitol has been used to decrease IOP in both animals models and humans, thereby establishing its safety and efficacy for this application. The use of mannitol to reduce IOP was initially suggested by Weiss et al. 14 Mannitol can reduce the pressure within the vitreous cavity and posterior chamber by concentrating the volume of the vitreous. This action results in a relative expansion of the anterior chamber volume. This property is particularly beneficial in cataract surgery for patients with PACD, in whom challenges such as shallow anterior chambers and elevated IOP complicate the procedure.5,14 By expanding the anterior chamber, mannitol use prior to surgery can help mitigate these issues, potentially reducing the risk of intraoperative complications. Potential complications that can arise during the combined procedure of cataract extraction and goniosynechialysis in patients with PACD encompass acute infusion fluid misdirection, 15 iris prolapse, 16 and zonulysis. 17 The risk factors contributing to these intraoperative complications include a shallow anterior chamber, a short axial length, and a high prevalence of zonulopathy in eyes with PACD.15,16,18 In the current study, consistent with previous reports, six eyes (18.2%) in the control group experienced intraoperative complications. These complications included acute infusion fluid misdirection, posterior capsule rupture, iris prolapse, inadvertent propagation of a capsule tear, and zonulysis during the phacoemulsification process. According to our findings, the preoperative administration of intravenous mannitol can reduce the incidence of intraoperative complications, resulting in better BCVA and lower IOP postoperatively. The group that experienced intraoperative complications exhibited higher postoperative IOP and lower BCVA than the group without complications. Furthermore, in this study, the administration of mannitol intravenously prior to surgery effectively reduced the time required for the capsulorhexis process, suggesting that an increase in the anterior chamber space facilitates the procedure.
Acute infusion fluid misdirection, a rare yet serious complication of cataract surgery in patients with short axial length, 19 arises when the aqueous humor is propelled into the vitreous cavity because of an elevated posterior pressure gradient. This condition is characterized by a shallow anterior chamber, increased IOP, and diminished vision. 15 In this study, acute infusion fluid misdirection was observed in two eyes (6.1%) in the control group. This suggests that its occurrence was not incidental and that it might not be associated with the surgical technique. Conversely, no cases of acute infusion fluid misdirection were observed in the mannitol group, indicating that the preoperative administration of mannitol could potentially prevent this complication. Similarly, posterior capsular rupture and zonulysis, which are common complications of cataract surgery in patients with PACD and zonulopathy, occur when the zonules are weakened or damaged because of chronic angle closure or elevated IOP. This can lead to instability of the capsular bag, challenges in performing capsulorhexis, or lens subluxation.18,20 In the current study, one eye (3.0%) in the control group experienced posterior capsule rupture and another eye (3.0%) experienced zonulysis during phacoemulsification. However, no such complications were observed in the mannitol group. Chee et al. suggested that preoperative intravenous mannitol could contract the vitreous and deepen the anterior chamber, providing sufficient operative space to limit the occurrence of posterior capsular rupture and zonulysis intraoperatively. 21 This further substantiates the efficacy of preoperative mannitol administration in mitigating intraoperative complications during the combined procedure of cataract extraction and goniosynechialysis in eyes with PACD.
Performing capsulorhexis, a crucial step in cataract surgery for patients with PACD or a shallow anterior chamber,22,23 can be challenging because of the limited surgical space. This can lead to unintentional capsular rupture extension or insufficient capsulorhexis size. Hwang et al. reported a higher rate of wrinkling in patients with PACD (26.9%) undergoing cataract surgery than in patients without PACD (0%). This both extended the capsulorhexis duration and necessitated the implantation of a capsule tension ring. 22 In this study, patients with PACD were randomly assigned to the mannitol or control group. In the comparison of the capsulorhexis process between these groups, the duration of capsulorhexis was notably shorter in the mannitol group than in the control group (P < 0.001). Additionally, the number of times the forceps grabbed the capsule during the procedure was significantly lower in the mannitol group (P = 0.025). Multivariate analysis identified influencing factors such as the preoperative administration of mannitol and status of the zonules. Therefore, the findings of this study indicate that the preoperative administration of intravenous mannitol has the potential to induce vitreous condensation, theoretically increasing the anterior chamber space and reducing the duration of capsulorhexis.
This study identified zonulopathy as another factor influencing the capsulorhexis process. The observed zonulopathy rate (49.2%) was significantly higher than previously reported, potentially because of racial differences or varying disease severity at the time of surgery. A retrospective study by Salimi et al. demonstrated a high prevalence of zonulopathy in patients with PACD (7.3%), far exceeding the occurrence rate in the general population (0.46%–2.6%).18,24,25 Performing capsulorhexis in eyes with zonulopathy necessitates additional caution to prevent unintended capsule tear propagation, as zonular laxity fails to provide adequate counteraction, thereby extending the capsulorhexis duration.
In the therapeutic strategy for patients with PAC or PACG and a history of elevated IOP or significant PAS, there is a general consensus (albeit not standard care) in clinical practice regarding intravenous mannitol administration prior to pupillary dilation and cataract surgery. 26 However, the necessity of preoperative mannitol administration in patients with PACS, who lack a history of elevated IOP or PAS, remains controversial. This study conducted a subgroup analysis based on disease type and found that preoperative intravenous mannitol administration shortened the duration of capsulorhexis and reduced intraoperative complications in both the PACS and PAC + PACG groups. Although these trends align with the broader cohort, the small sample size in the PACS subgroup limits the strength of the conclusions and highlights the need for larger studies to validate these findings. This provides evidence supporting the clinical proposition that patients with PACS should receive intravenous mannitol prior to surgery. By deepening the anterior chamber and improving surgical conditions, mannitol both shortens the surgical duration and mitigates risks associated with complex intraoperative maneuvers. This insight serves as a valuable guide for clinical decision-making processes, emphasizing that preoperative mannitol should be considered in surgical protocols for patients with PACS, particularly in cases in which shallow anterior chambers and elevated IOP present challenges.
The limitations of this study include the lack of evaluation of long-term outcomes, particularly regarding post-surgical IOP control and visual acuity, as well as postoperative complications. Although the short-term benefits of preoperative intravenous mannitol were evident, its long-term impact on maintaining stable IOP and preserving visual function requires further investigation. Moreover, this study did not compare the effects of preoperative intravenous mannitol with other antiglaucoma drugs, such as acetazolamide, or alternative methods for reducing IOP before surgery. Additionally, although patients who received oral acetazolamide and those with conditions complicating mannitol use were excluded, the potential effects of other medications, including oral drugs and eye drops, on anterior chamber dynamics were not controlled, potentially affecting outcomes. This could have introduced variability in the outcomes, and this should be addressed in future studies.
In conclusion, this study indicated that preoperative intravenous mannitol can decrease the risk of intraoperative complications in patients with PACD undergoing cataract extraction combined with goniosynechialysis. It can also reduce the risk of suboptimal postoperative visual acuity recovery and poor IOP control to some extent, potentially reducing the duration of capsulorhexis. Factors such as preoperative mannitol administration and the status of the zonules play pivotal roles in influencing the capsulorhexis process. Therefore, these factors should be carefully considered when planning cataract surgery for patients with PACD, as they can significantly impact surgical processes and outcomes. Future studies should include longer follow-up periods and a comparison of different preoperative interventions to fully assess their relative efficacy in managing PACD.
Footnotes
Acknowledgements
We thank Qian Zhang and Yafei Fu for performing UBM in all subjects.
Author contributions
Huijuan Wu was responsible for the conceptualization of the study. Zhiqiao Liang and Xianru Hou curated the data. Zhiqiao Liang conducted the formal analysis. The methodology was developed by Zhiqiao Liang, Kangyi Yang, Kun Lv, Yao Ma, Ye Lu, and Kuankuan Wu. The original draft of the manuscript was written by Zhiqiao Liang and Hongyan Li. Huijuan Wu reviewed and edited the manuscript. All authors have read and agreed to the published version of the manuscript.
Data availability statement
Data presented in this study are available from the corresponding author upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
This work was supported by Capital’s Funds for Health Improvement and Research (2024-2-4087) and Central guidance for local scientific and technological development funding projects (2022ZY0026). The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.