
Abstract
Objective
The cardiac return assist blanket (CRAB) has been designed to increase central venous pressure (CVP) to manage severe hypotension associated with anaphylaxis. This interventional study aimed to identify the relationship between CRAB pressure and CVP. CRAB pressure was also compared with the change in CVP associated with a straight leg raise (SLR), the Trendelenburg position, and 1 L of compound sodium lactate.
Methods
Sixteen healthy, fasted volunteers were exposed to CRAB pressure at 10, 20, 30, and 40 cmH2O, the SLR, and 15 degrees of the Trendelenburg position. The volunteers were then fed and hydrated with 1 L of CSL over 30 minutes and the protocol was repeated.
Results
The initial 10 cmH2O of CRAB pressure increased CVP by 3.7 mmHg (95% confidence interval 2.7, 4.7). Each subsequent 10-cmH2O rise in CRAB pressure increased CVP by 0.9 mmHg (95% confidence interval 0.55, 1.25). The SLR, Trendelenburg position, and 1 L of CSL increased CVP by 0.97 , 0.75 , and 0.69 mmHg, respectively.
Conclusions
The CRAB controllably increases CVP, and 40 cmH2O of CRAB pressure increases CVP by 6.41 mmHg. The effect of the CRAB is greater than that with the SLR, Trendelenburg position, or 1 L of CSL.
This trial was registered with the ANZCTR (ACTRN12621000840886: https://www.anzctr.org.au).
Keywords
Introduction
The cardiac return assist blanket (CRAB) was designed to increase central venous pressure (CVP) to manage hypotension associated with anaphylaxis. Anaesthetic anaphylaxis is an uncommon emergency, occurring in 1:6000 to 1:20,000 anaesthetic procedures. 1 A total of 51% of patients require cardiopulmonary resuscitation and approximately 4% of cases are fatal. 2 In Australia, <1% of patients die, but anaesthetic anaphylaxis is still the most common cause of death due to anaesthesia. 3 Mortality from anaphylaxis is mostly a result of the sequalae of hypotension. Anaphylactic hypotension is partly due to a reduction in systemic vascular resistance, but there is also a reduction in venous return associated with reduced CVP, and thus a reduction in cardiac output. 4
Anaphylactic hypotension has been well investigated in many animal models. A study on anaphylaxis in dogs showed that dogs commonly survived 30 minutes of severe hypotension but then died overnight. 5 Autopsies showed a hyperaemic bowel and areas of bowel that were haemorrhagic, which suggested that severe splanchnic congestion occurred during the anaphylaxis. Other anaphylaxis studies on dogs, 6 rabbits, 7 guinea pigs, 8 rats, 9 calves,10,11 and mice 11 examined multiple parameters, such as CVP, portal pressure, and hepatic venous tone. These studies showed similar results, which suggested that in all animals, anaphylaxis causes hepatic venoconstriction and portal hypertension, which then causes congestion of the upstream splanchnic organs and, consequently, a decrease in venous return and effective circulating blood volume, and, finally, augmentation of anaphylactic hypotension. 11 The same mechanisms are likely to occur in humans. The splanchnic circulation normally contains 25% of the circulation 12 and hepatic venoconstriction causing portal hypertension with splanchnic vein venodilation could dramatically increase this volume. The combination of portal hypertension and leaky capillaries from anaphylaxis could cause rapid intestinal oedema. 13
Experience with other lower body compression devices suggests that the CRAB is safe. Fighter jet pilots have used aviator anti-G suits since World War II to help prevent the loss of consciousness during high G force manoeuvres. These suits automatically pressurise the lower body up to 750 cmH2O 14 for brief periods of time during the manoeuvres. The CRAB is intrinsically safer than these suits because it uses a lower maximum pressurise of 40 cmH2O. Positioning of the CRAB on patients is much easier than military anti-shock trousers (MAST suit) because it is inserted under the patient. The difficulties associated with applying the MAST suit leads to 4-minute delays at trauma scenes. 15 The MAST suit, aviator anti-G suits, and other novel lower body compression devices induce a large increase in CVP (5–8 mmHg).16–18 The MAST suit is also successful in managing hypotension from anaphylaxis.19–21 The largest case series reported 11 patients with anaphylaxis who had the MAST suit inflated with a mean rise in systolic blood pressure of 58 mmHg. 22
Increasing CVP with intravenous (IV) fluids and a straight leg raise (SLR) are recommended methods of treating anaphylactic hypotension. Unfortunately, infusing large volumes of IV fluids is difficult to achieve in an emergency. 2 No previous studies have examined the expected rise in CVP in healthy volunteers from 1 L of compound sodium lactate (CSL), the SLR, or the Trendelenburg position. Pre-trial investigations on multiple volunteers showed that increasing CRAB pressure increased the volume of the central neck veins when assessed by ultrasound. This suggested that CRAB increased CVP. One volunteer (Figure 1) also had a peripheral IV cannula inserted and a pressure transducer attached. A CRAB pressure of 40 cmH2O increased peripheral venous pressure by 6 mmHg. These pre-clinical trials guided the design of this study.

Image of use of the cardiac return assist blanket in a volunteer during a pre-clinical study.
This study primarily aimed to show the relationship between CRAB pressure and the rise in CVP in healthy volunteers. Secondary aims were to investigate the change in CVP from 1 L of CSL, the SLR, and 15 degrees of the Trendelenburg position compared with the CRAB. Their effects on heart rate (HR), blood pressure (BP), and oxygen saturation (SaO2) were examined. The safety of the CRAB was also investigated.
Materials and methods
Ethics approval
The protocol for this interventional trial was approved by the HREC and SCGHOPH Research Ethics Committee at Sir Charles Gairdner Hospital on 28 October 2021 (approval number: RGS00451). The trial was registered with the ANZCTR (ACTRN12621000840886; Universal Trial Number: U1111-1267-4979; and the Therapeutic Goods Administration: CT-2020-CTN-04786-1).
Participants
All participants had an American Society of Anaesthesiologists physical status grade I or 2 and were aged between 18 and 70 years old. Participants were excluded if they were pregnant, had abdominal surgery in last 6 months, had cardiac disease (ischaemic heart disease, valvular disease, arrythmias, or a history of recurrent vasovagal episodes), respiratory disease (symptoms of controlled mild asthma were accepted), any major medical conditions (American Society of Anaesthesiologists physical status III or IV), or were on prescription medication for the cardiovascular or respiratory system. All participants signed a consent form before commencing the study. Written approval for the use of photographs for publication was obtained from the participants.
Study protocol
The CRAB blanket, which was designed by one of the authors of this study, was 80 cm wide and 1 m long. This blanket was constructed from two sheets of airtight fabric, which were bonded around the edge to form a single air cell. The blanket was held onto the patient by four evenly spaced Velcro© loop straps (Velcro Australia Pty. Ltd., Pakenham, Australia), which were passed under the table/trolley and back onto Velcro hooks on the blanket. The upper edge was positioned under the patient’s xiphisternum, and the lower edge lay between the knees and ankles. When the pump was started, it inflated the blanket to 10 cmH2O, and then the pressure was adjusted up to 40 cmH2O. Two trained staff positioned and started applying the CRAB in less than 1 minute without any movement or manipulation of the patient.
All investigations were performed in the Interventional Radiology Department at Sir Charles Gairdner Hospital. Volunteers who had fasted without food or drink from midnight arrived in the morning. CVP monitoring was achieved with a 20-cm, single-lumen, 4 French Arrow midline catheter (Teleflex Medical Australia, Mascot, Australia), which was inserted under ultrasound guidance in the basilic or brachial vein, and the tip was advanced 20 cm into the central circulation. The insertion was completed by an experienced vascular access nurse. The midline catheter was connected to a pressure transducer, and the transducer was taped at the fourth intercostal space in the mid-axillary line. Continuous non-invasive BP monitoring was achieved with the Edwards Lifesciences ClearSight system (Edwards Lifesciences Australia Pty. Ltd., North Ryde, Australia) with a heart reference sensor taped to the fourth intercostal space in the mid-axillary line. The CVP transducer (ClearSight) and a pulse oximeter were connected to a GE Carescape B450 (GE HealthCare, Mascot, Australia). All data were transmitted in real time to a PC computer using VitalRecorder 1.9.9 software (VitalDB, Seoul, Korea). The participants lay supine on a hospital trolley with their heads on a pillow. The CRAB was placed on the participants with the superior border at the level of the xiphisternum, and the inferior border was between the knees and ankles.
The protocol comprised 12 stages. Six stages of 2 minutes of no intervention alternated with 2 minutes of intervention. The six interventions were as follows: inflation of the CRAB to 10, 20, 30, and 40 cmH2O, no CRAB inflation with an SLR, and no CRAB inflation in the Trendelenburg position. CVP, BP, HR, and SaO2 were recorded at the halfway point of each 2-minute stage. After completing the protocol, the participants were fed breakfast and hydrated with 1 L of CSL by the midline catheter over 30 minutes. The identical 12-stage protocol was then repeated immediately after completion of IV fluids.
On completion of the trial, the participants completed a questionnaire regarding their experience of being under the CRAB at the 10-cmH2O and 40-cmH2O pressures. They were asked to rate the experience on a linear scale of 0 to 10 for pain, tolerability, and difficulty breathing. They were also asked to write any comments about their experience.
The study was conducted in accordance with the Helsinki Declaration of 1975 as revised in 2013. The reporting of this study conforms to the CONSORT 2020 statement. 23
Statistical methods
The participants’ questionnaire data are shown as the non-parametric median, interquartile range, and range. Linear mixed effects models with random subject effects were used to obtain estimated mean CVP, BP, HR, and SaO2 outcome measures, such as nil pressure, CRAB increments (10, 20, 30, and 40 cmH2O), the SLR, and the Trendelenburg position, at every time point. Pairwise comparisons were performed between baseline and time points, and between hypotension and normal groups. The results are summarised using marginal means, mean differences, and 95% confidence intervals (CIs). Regression beta coefficients and 95% CIs of CVP between CRAB pressures were used to describe the gradient of the line of the best fit for CVP. Stata version 17.0 (StataCorp, College Station, TX, USA) was used for data analysis.
We calculated that we needed a sample of n = 16 with 12 repeats for 80% power (alpha = 0.05) in a linear mixed model to detect an effect size of f = 0.216 (equivalent to partial eta squared = 0.045 or 4.5% difference) (G*Power 3.1.9.7; https://www.psychologie.hhu.de/arbeitsgruppen/allgemeine-psychologie-und-arbeitspsychologie/gpower).
Results
Between 31 July and 3 September 2022, eight men and eight women aged between 18 and 69 years old with a mean (±standard deviation) age of 38 ± 17 years provided consent and completed the study.
The results of the changes in CVP with the different interventions are shown in Table 1. A CRAB pressure of 10 cmH2O led to a significant rise in CVP of 3.69 mmHg (p < 0.001). Further stepwise 10-cmH2O increases in CRAB pressure resulted in smaller increases in CVP. The gradient of the line of best fit from 10 cmH2O to 40 cmH2O showed a 0.9-mmHg (0.5–1.25) rise for each addition of 10 cmH2O of CRAB pressure. The change in CVP with 40 cmH2O of CRAB pressure was 6.41 mmHg.
Combined fasted and hydrated CVP measures with changes from baseline.
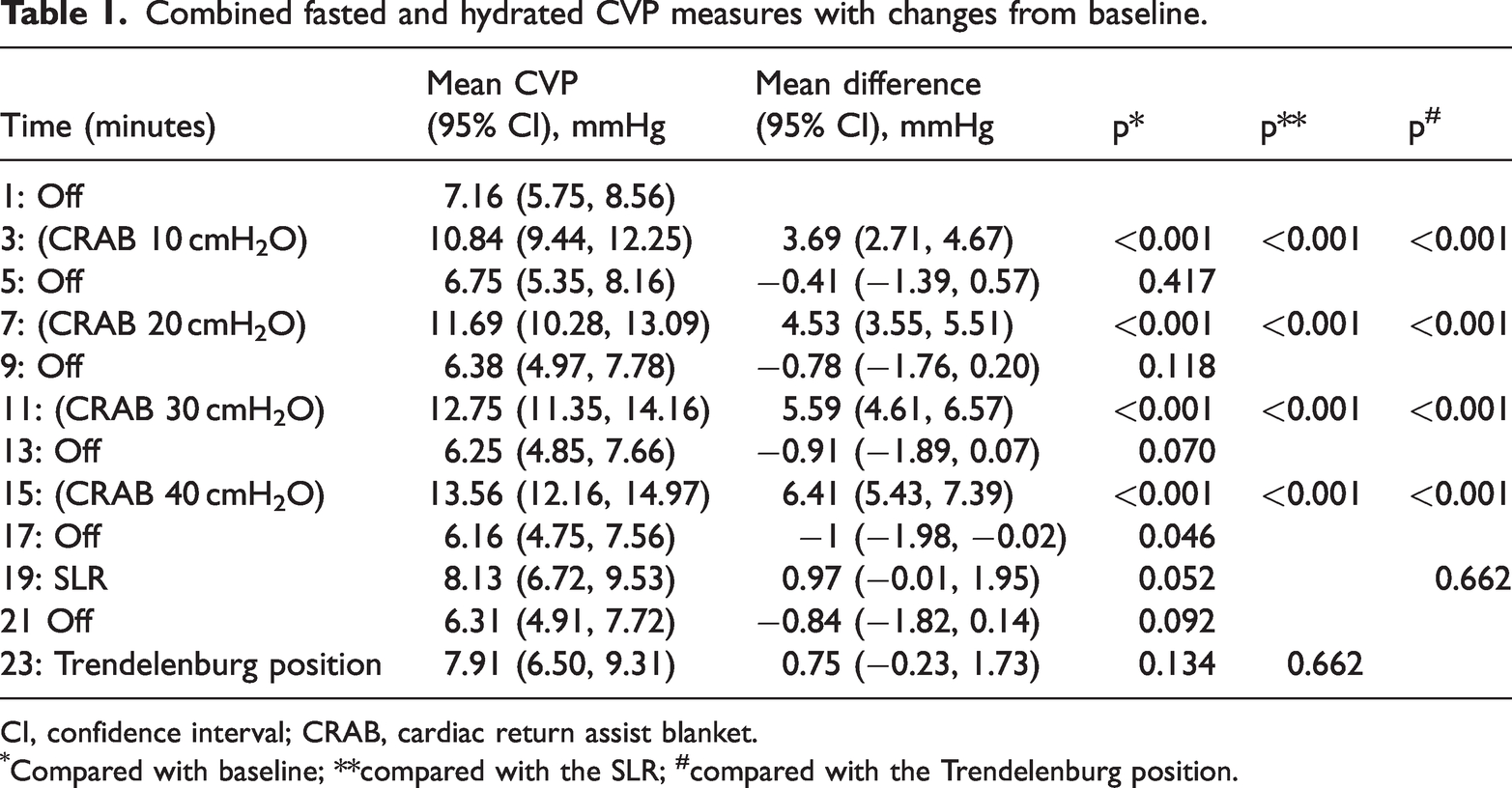
CI, confidence interval; CRAB, cardiac return assist blanket.
Compared with baseline; **compared with the SLR; #compared with the Trendelenburg position.
At 1 minute, the SLR resulted in an increase in CVP of 0.97 mmHg from baseline , but this was not a significant change. However, CVP during the no intervention stages showed a downward trend throughout the study from 7.16 to 6.16 mmHg. When the change in CVP with the SLR was measured from the no intervention stage 2 minutes earlier, the increase in CVP was 1.97 mmHg. The change in CVP with the first 10 cmH2O of CRAB pressure was 187% greater than the 1.97-mmHg change achieved by the SLR.
Applying 15 degrees of the Trendelenburg position only increased CVP by 0.75 mmHg from baseline and by 1.6 mmHg from the no intervention stage 2 minutes earlier. This change was smaller than that achieved with the SLR.
The results of CVP by the fasting status are shown in Figure 2. Hydration with breakfast and 1 L of CSL over 30 minutes only raised CVP by 0.69 mmHg (95% CI 2.06, −0.68), which was not a significant change. There was no significant difference in CVP between the fasted and hydrated phases of the study for any of the data points. The change in CVP achieved by the first 10 cmH2O of CRAB pressure was 534% greater than that achieved by hydration.
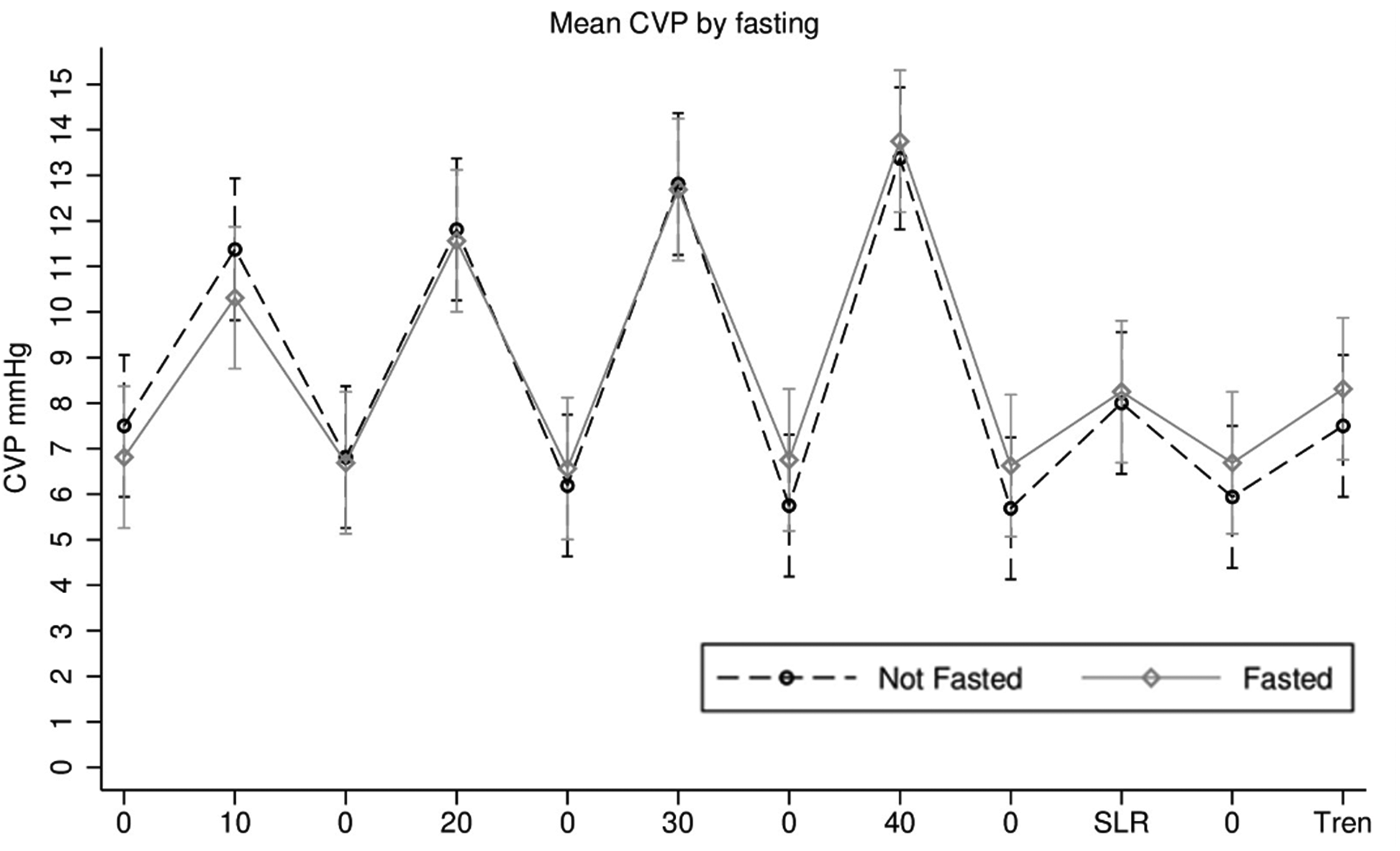
Mean CVP according to the fasting status for all interventions. There was no significant difference in CVP between the fasted and hydrated conditions. CVP, central venous pressure; SLR, straight leg raise; Tren, Trendelenburg position.
There was no clinically significant or statistically significant change in systolic BP, diastolic BP, HR, or SaO2 during any of the interventions.
The questionnaire (Table 2) showed that even at the highest pressure, the CRAB was well tolerated and caused minimal pain or difficulty in breathing. The comments from the participant who scored the highest pain score 6 was that 30 and 40 cmH2O of pressure caused headaches. This participant also had the greatest change in CVP when the CRAB was inflated to 40 cmH2O, with a rise in CVP from 8 to 20 mmHg.
Questionnaire results.

CRAB, cardiac return assist blanket; IQR, interquartile range; min, minimum; max, maximum.
Discussion
The main finding of this study is that inflation of the CRAB caused a significant rise in CVP. Importantly, the 3.69-mmHg rise at 10 cmH2O and 6.41-mmHg rise at 40 cmH2O were large enough to be clinically significant. These large changes are consistent with those in previous studies on lower body pressure devices.16,18
The SLR is considered a clinically important manoeuvre to increase CVP, and it is recommended in Australian and New Zealand Anaesthetic Allergy Group anaphylaxis management protocols for cardiac arrest. 24 In this study, the CRAB at 10 cmH2O was 187% more effective than SLR, and the CRAB at 40 cmH2O was 325% more effective than the SLR at raising CVP. These findings suggest that deploying the CRAB by operating theatre staff would be more effective than performing the SLR. Furthermore, after the CRAB is deployed, staff would be free to perform other tasks, whereas the SLR requires the constant attention of at least one staff member and might be difficult to maintain.
IV therapy is also an accepted method of increasing CVP. In this study, breakfast and 1 L of CSL over 30 minutes only increased CVP by 0.7 mmHg, which suggests that several litres may be required to achieve clinically significant rises. The first 10 cmH2O with the CRAB was 534% more effective than 1 L over 30 min. Administering a large volume of IV fluid for hydration takes a long time. In the NAP 6 report, an average of 1 L of fluid is provided in the first hour and may require the anaesthetist, who is performing the resuscitation, to place a new IV cannula. 2 Deployment of the CRAB may be a better use of initial resources.
The success of the CRAB compared with the SLR and IV administration is probably explained by the highly compliant splanchnic circulation. The splanchnic circulation contains 25% of the circulating blood volume. Therefore, compressing this area can lead to a large volume of blood being redistributed to the upper body. However, when 1 L of IV fluid is added to the circulation or the SLR redistributes venous blood away from the legs, most of the fluid likely remains in the compliant splanchnic circulation, and only a small volume is redistributed to the upper body. During anaphylaxis, when splanchnic vein congestion is causing hypotension, there is likely to be an even a greater volume of blood available for the CRAB to redistribute. This redistribution should enable the CRAB to partially reverse the drop in CVP and venous return, which has been well documented to occur with hypotension from anaphylaxis. In a 10-year case series on 226 patients with anaphylaxis, Fisher reported that 46 of the patients had CVP monitoring at some stage of the anaphylaxis. 4 The author of this review reported that “CVP was low in all patients without cardiac disease”. Recently, the use of transoesophageal echocardiography has shown a consistent lack of preload. A literature review reported 10 cases of transoesophageal echocardiography used in the early phase of anaphylaxis. Seven of these patients showed hypovolaemia and a hyperdynamic heart, which improved with IV fluids. Three patients had systolic anterior motion of the anterior mitral leaflet, and more fluid and less adrenaline were required to establish cardiac output.
The CRAB, may treat anaphylaxis hypotension by two mechanisms. One mechanism is that inflation of the CRAB immediately increases the venous pressure in the lower body veins to redistribute venous blood back to the central circulation. Another mechanism is that the CRAB also increase pressure in bowel tissue, changing the balance of Starling’s forces across the capillaries. Over the duration of the anaphylaxis, this should reduce bowel oedema and minimise intravascular fluid loss. Stopping the development of hypovolaemia and redistributing blood back to the central circulation is likely to increase CVP and restore venous return and cardiac output, and improve blood pressure.
Safety issues are unlikely to arise from lower body pressure with the CRAB. The aviator and MAST suits are much higher pressure devices than the CRAB and have been used for a long time without problems arising from the pressure effect. In this study, the awake participants found that the CRAB was tolerable. One participant experienced a bad headache during inflation of the CRAB to 30 and 40 cmH2O. This headache was likely due to the high CVP (20 mmHg). This is an unlikely problem when treating patients with a low initial CVP.
In this study, BP, HR, and SaO2 did not change in a clinically or significant manner during any of the interventions, even with a CRAB pressure of 40 cmH2O and a 6.41-mmHg rise in CVP. This lack of finding is probably because the healthy volunteers were able to autoregulate to maintain normal BP and HR. During anaphylaxis when a low CVP is causing inadequate cardiac filling, low cardiac output, tachycardia, and hypotension, a rise in CVP is expected to cause an improvement in these parameters. However, this possibility will need to be verified in future studies.
The ability to controllably raise CVP without administering IV fluids may lead to other uses for the CRAB. The rise in CVP is associated with neck vein dilation. Therefore, the CRAB could be used during central venous line insertion as an alternative to the Trendelenburg position, which has been proven to be helpful, 25 but is sometimes poorly tolerated by patients. During cardiopulmonary bypass, achievable pump flow can be limited by the venous reservoir volume, which can be augmented by techniques, such as vacuum-assisted venous drainage and transfusion of exogenous fluid or blood products. The CRAB device could be advantageous in this situation to reduce the patient’s venous capacitance and promote venous return to the reservoir.
In this study, the change in CVP was measured as the difference from the initial CVP. However, CVP during the no intervention stages showed a downward trend through the 24 minutes of the study from 7.16 to 6.16 mmHg. The physiological reason behind this downward trend in baseline CVP is not easily explained but probably reflects autoregulation. Future studies should be performed to measure the change in CVP from that just prior to each intervention. There are still many unknown physiological effects that might arise from CRAB pressure. In particular, there is likely to also be a rise in intrathoracic pressure, which could reduce the preload effects of the rise in CVP. The net effect could be further complicated by the difference between spontaneously ventilated and ventilated patients. This study showed a strong association between increasing CRAB pressure and CVP. However, further research is required to understand the other physiological effects of the CRAB and to determine if it helps resuscitation of anaphylaxis or central line insertion or if it has other uses.
Conclusion
Inflation of the CRAB caused a large and clinically significant change in CVP. A CRAB pressure of 10 cmH2O increased CVP by 3.69 mmHg. Each subsequent 10-cmH2O increase in CRAB pressure increased CVP by 0.9 mmHg to a maximal increase of 6.41 mmHg at 40 cmH2O. These increases were controllable and significantly larger than those produced by the SLR and IV fluids. These findings suggest that the CRAB is useful in the management of low CVP conditions such as anaphylaxis-induced hypotension.
Footnotes
Acknowledgements
We would like to thank the Sir Charles Gairdner Hospital Anaesthetic Allergy group (Peter Platt, Paul Sadlier, and Russell Clarke) for supplying the inspiration to develop the CRAB and for the constant feedback and enthusiasm through this long process.
Author contributions
C Mitchell – Study design, data collection, writing of the manuscript, and submission.
A Jacques – Study design, power analysis, statistical analysis, and review of the manuscript.
Data availability
Primary data are available by contacting the corresponding author:
Declaration of conflicting interest
C Mitchell is the inventor of the CRAB and the owner of Coco Industries Pty. Ltd. Coco Industries Pty. Ltd. holds the patent for the CRAB and paid for any expenses associated with this study. A Jacques declares that there is no conflict of interest.
Funding
All costs associated with this study were paid for by Coco Industries Pty Ltd. SCGH paid for the space to conduct the study and provided reuseable equipment. GE Healthcare loaned the Carescape B450 monitor. Edwards Lifesciences loaned the ClearSight system.