
Abstract
Objective
This study compared the clinical efficacy of off-pump coronary artery bypass grafting (OPCAB) with percutaneous coronary intervention (PCI) in the treatment of left main coronary artery and/or triple-vessel disease (LM and/or TVD).
Methods
We retrospectively enrolled 1484 consecutive patients with LM and/or TVD in Shanxi Cardiovascular Hospital from January 2015 to December 2022 and divided them into the OPCAB group (n = 583) and the PCI group (with second-generation drug-eluting stents) (n = 901). Propensity score matching was used for 316 equally matched pairs of patients in the groups. The outcomes were all-cause and cardiac mortality, angina recurrence, and major adverse cardiac and cerebrovascular events, which comprised non-lethal myocardial infarction, stroke, and repeat revascularization.
Results
The mean follow-up was 3.93 years in the OPCAB group and 4.19 years in the PCI group. There were no significant differences in all-cause mortality, cardiac mortality, major adverse cardiac and cerebrovascular events, or non-lethal myocardial infarction between the groups. The incidence of repeat revascularization and angina recurrence was higher in the PCI group than in the OPCAB group. However, the incidence of stroke was higher in the OPCAB group than in the PCI group.
Conclusions
OPCAB may be a favorable coronary revascularization strategy for LM and/or TVD.
Keywords
Introduction
Coronary artery disease (CAD) is currently one of the most common cardiovascular diseases worldwide, and approximately 7 million people die from CAD every year worldwide. 1 Coronary artery bypass grafting (CABG) is considered as the standard procedure for revascularization of left main coronary artery disease (LMCAD) and triple-vessel disease (TVD) because of its advantages of a high long-term patency rate and low repeat revascularization rate. 2 Conventional on-pump CABG is performed using cardiopulmonary bypass and induces cardiac arrest to facilitate anastomosis, which may increase the incidence of several complications. These complications include systemic inflammation, neurological and renal dysfunction, and ischemic myocardial injury. Off-pump coronary artery bypass grafting (OPCAB) avoids cardiopulmonary bypass and cardioplegic arrest, with less aortic manipulation, which could eliminate the complications caused by cardiopulmonary bypass and cardiac arrest. 3 Therefore, investigating the effect of OPCAB in patients with more complex coronary lesions is important.
With the development of drug-eluting stents (DESs) and endovascular imaging technology, the long-term patency rate after percutaneous coronary intervention (PCI) has also improved. PCI has become one of the options for treating CAD because of its advantages of minimal surgical trauma and rapid postoperative recovery. 4 At present, the second-generation of DESs plays a major role in PCI treatment of CAD.5,6 Several randomized, controlled trials showed that the gap between CABG and PCI in effectively treating LMCAD and TVD has gradually narrowed.7–9 However, these studies did not evaluate the effect of OPCAB on outcomes. Collecting and comparing a large amount of clinical research data is necessary to evaluate and compare the medium- and long-term effects of OPCAB and PCI in treating LMCAD and TVD.
Therefore, this study compared the clinical efficacy of OPCAB with PCI and second-generation DESs in the real-world treatment of patients with left main coronary artery and/or triple-vessel disease (LM and/or TVD).
Methods
Study design and setting
A retrospective study was conducted on consecutive patients with LM and/or TVD who underwent OPCAB or PCI at Shanxi Cardiovascular Hospital from January 2015 to December 2022.
This study was approved by the Ethics Review Board of Shanxi Cardiovascular Hospital (Institute) (approval number: 2019010, approval date: 30 July 2019). This study was conducted in accordance with the Declaration of Helsinki. Individual consent of the patients was waived owing to the retrospective nature of the study. We had de-identified all of the patients’ details. The reporting of this study conforms to the STROBE guidelines. 10
Participants
The inclusion criteria were as follows: age between 18 and 85 years old; an internal diameter of the lumen wall >1.5 mm on coronary angiography; stenosis of the left main artery >50% and/or stenosis of the three coronary arteries >70%; medication was taken when required; and a regular postoperative reexamination was performed. The exclusion criteria were as follows: patients with a previous history of revascularization; those who underwent other operations during follow-up; and those with severe liver, renal, or blood system diseases. The patients were divided into the OPCAB group and the PCI group according to the type of surgery that they underwent.
All enrolled patients were treated according to standard clinical diagnostic and treatment procedures.
Revascularization strategies
All OPCAB operations were performed by a single surgeon (Yongzhi Deng) according to basic surgery specifications. All patients in the OPCAB group underwent OPCAB through a median sternotomy. The arterial grafts of OPCAB included the left internal mammary artery and radial artery, and the long saphenous vein was mainly used for vein grafts. The left internal mammary artery was used as a conduit preferentially to the left anterior descending coronary artery. Radial artery use was restricted to the left anterior descending coronary artery when the left internal mammary artery was unsatisfactory and was uncommon. The obtuse marginal, posterior descending coronary artery or the distal right coronary artery was bypassed using the long saphenous vein. Proximal anastomosis was achieved by partially clamping the ascending aorta by lateral-side bite clamping to achieve partial occlusion of blood flow. All patients with OPCAB received aspirin (100 mg/day) and clopidogrel (75 mg/day) from the day of the operation, and this dual antiplatelet therapy was maintained for at least 9 months unless contraindicated because of the patient’s specific condition. Statins were routinely used after the operation during the study period.
All PCI operations were performed by cardiologists (Jin Dong and Shoudong Wei) according to standard interventional techniques. In the PCI group, second-generation DESs were used in all of the patients. The choice of stent type depended on the preference of the individual interventional cardiologist. Dual antiplatelet treatment with aspirin and clopidogrel was initiated before PCI. After PCI, aspirin (100 mg/day) and clopidogrel (75 mg/day) were provided for at least 12 months, and then aspirin was continued for at least 18 to 24 months, except for in patients with a gastric ulcer who continued with clopidogrel.
Data collection and definitions
Demographic, angiographic, and procedural data were collected from patients’ charts and hospital databases. Follow-up information was obtained by outpatient follow-up and/or telephone follow-up. If a patient died at the time of contact, the investigators attempted to obtain data from the family regarding death, including non-fatal events before the time of death.
Baseline clinical characteristics, such as myocardial infarction (MI), heart failure, diabetes, hypertension, smoking history, atrial fibrillation, chronic obstructive lung disease, and hyperlipemia, were regarded as present when these diagnoses were recorded in the hospital charts. The left ventricular ejection fraction was measured by echocardiography. A left ventricular ejection fraction <50% was defined as left ventricular dysfunction.
Outcomes
The outcomes assessed in this study were perioperative mortality and follow-up mortality, including all-cause mortality and cardiac mortality. Cardiac death included MI, death from heart failure, ventricular arrhythmias, and sudden death. Other outcomes were the recurrence of angina and any major adverse cardiac and cerebrovascular events (MACCE), which comprised non-lethal MI, stroke, and repeat revascularization, during the follow-up period.
Statistical analysis
Continuous variables are shown as the mean ± standard deviation or median (interquartile range), as appropriate. Baseline demographic characteristics were compared using the Mann–Whitney U-test for continuous variables and Pearson’s chi-square test or Fisher’s exact test for categorical variables.
Cumulative incidence functions of death from any cause, death from cardiac causes, non-lethal MI, stroke, repeat revascularization, recurrence of angina, and MACCE were estimated by the Kaplan–Meier method and compared using the log-rank test. Cox proportional hazard analyses were performed to evaluate the hazard ratio (HR) for events.
A propensity score-matching (PSM) analysis was performed to evaluate the efficacy of OPCAB with that of PCI using second-generation DESs. Propensity scores were estimated using a logistic regression model in which the outcomes were the log of the odds of undergoing surgical interventional procedures. Based on the collected data combined with years of clinical experience and referring to the relevant literature,11,12 the following 19 covariates were entered into the multivariable model: age, female sex, body mass index, smoking history, diabetes mellitus, hypertension, dyslipidemia, cerebrovascular disease, chronic obstructive pulmonary disease, poor mobility, EuroScore II, type of coronary artery disease, Canadian Cardiovascular Society angina class, congestive heart failure, atrial fibrillation, serum creatinine concentrations, renal insufficiency, type of coronary artery lesion, and the Synergy between Percutaneous Coronary Intervention with Taxus and Cardiac Surgery (SYNTAX) score. Using a 1:1 greedy nearest neighbor matching algorithm, OPCAB and second-generation DESs were matched according to a caliper width equal to 0.2 of the standard deviation of the logit of the propensity score. A total of 316 pairs of patients were successfully matched. After PSM, the Wilcoxon signed rank test was used for continuous outcomes, and McNemar or McNemar–Bowker test was used for categorical outcomes.
All tests were two-tailed and P < 0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS version 25 (IBM Corp., Armonk, NY, USA) and R Studio version 4.2.1 (www.r-project.org).
Results
Baseline characteristics
We included 1484 consecutive patients with LM and/or TVD who underwent OPCAB (n = 583) or PCI (n = 901) (Figure 1). The demographic characteristics of the patients were compared. The real-world data before PSM were compared and are shown in Table 1. Before PSM, patients in the OPCAB group had a significantly higher percentage of several comorbidities, such as hypertension, diabetes, hyperlipidemia, peripheral vascular disease, and cerebrovascular disease, than those in the PCI group (all P < 05). TVD was the dominant coronary disease in both groups, but the OPCAB group had significantly more patients with LM + TVD than those in the PCI group (P < 0.001).

Flow diagram of the study population. OPCAB, off-pump coronary artery bypass grafting; PCI, percutaneous coronary intervention; DES, drug-eluting stent.
Baseline characteristics of the patients.
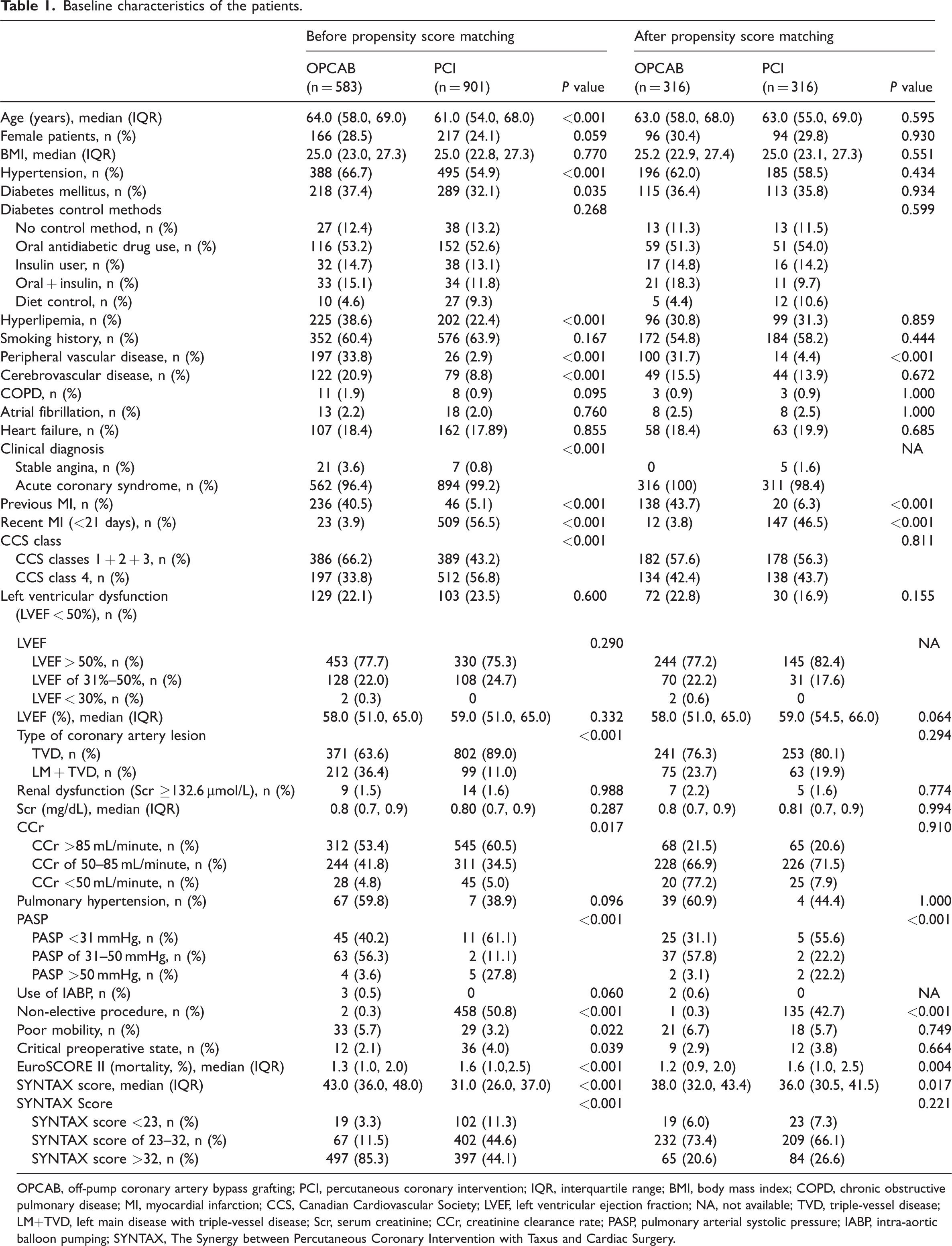
OPCAB, off-pump coronary artery bypass grafting; PCI, percutaneous coronary intervention; IQR, interquartile range; BMI, body mass index; COPD, chronic obstructive pulmonary disease; MI, myocardial infarction; CCS, Canadian Cardiovascular Society; LVEF, left ventricular ejection fraction; NA, not available; TVD, triple-vessel disease; LM+TVD, left main disease with triple-vessel disease; Scr, serum creatinine; CCr, creatinine clearance rate; PASP, pulmonary arterial systolic pressure; IABP, intra-aortic balloon pumping; SYNTAX, The Synergy between Percutaneous Coronary Intervention with Taxus and Cardiac Surgery.
After PSM, there were no significant differences in the baseline data between the two groups (Table 1).
Procedural data and in-hospital outcomes
The perioperative data of the two groups were analyzed, and the results of the total cohorts and the PSM cohorts are shown in Table 2. The incidence of perioperative mortality was 0.5% in the OPCAB group, and 0% in the PCI group. The mean number of bypass grafts per patient was 2.95 ± 0.65, and the mean number of stents was 2.25 ± 1.18. The study included only a few patients with isolated LMCAD, in whom only one or two grafts were used, resulting in an average of fewer than three grafts.
Perioperative characteristics of the OPCAB and PCI groups before and after propensity score matching.
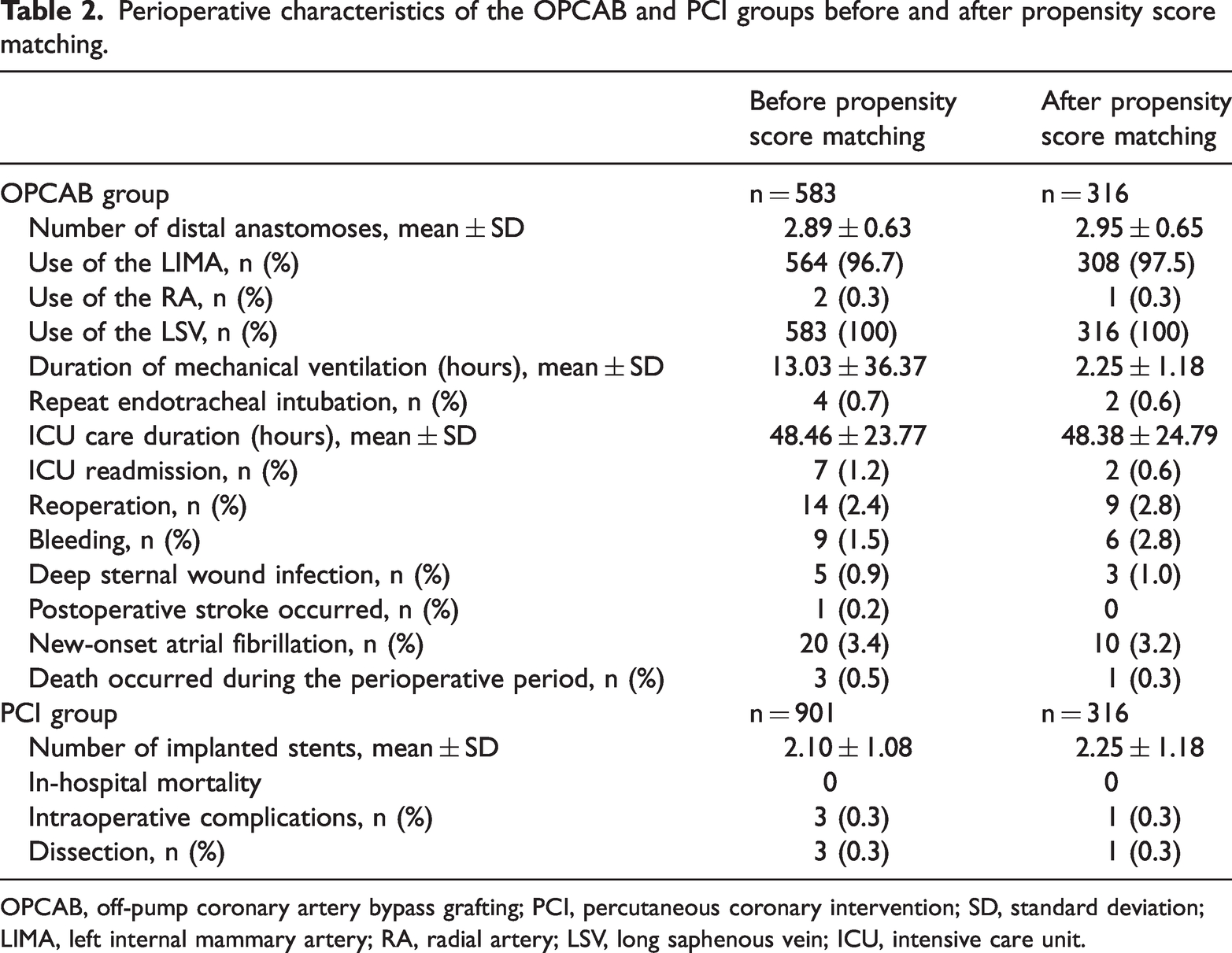
OPCAB, off-pump coronary artery bypass grafting; PCI, percutaneous coronary intervention; SD, standard deviation; LIMA, left internal mammary artery; RA, radial artery; LSV, long saphenous vein; ICU, intensive care unit.
Late outcomes
The perioperative characteristics of the two groups and the PSM cohorts are shown in Table 3. Before PSM, the median follow-up was significantly shorter in the OPCAB than in the PCI group (P < 0.001), with 7.38% and 8.99% of the patients lost to follow-up in each group, respectively. After PSM, the median follow-up was also significantly shorter in the OPCAB group than in the PCI group (P < 0.001).
Follow-up outcomes of OPCAB versus PCI before and after propensity score matching.

OPCAB, off-pump coronary artery bypass grafting; PCI, percutaneous coronary intervention; IQR, interquartile range; MACCE, major adverse cardiac and cerebrovascular events.
The Cox regression analysis showed that all-cause mortality at 4 years was lower in the PCI group than in the OPCAB group before PSM (3.11% vs 6.35%; hazard ratio [HR], 0.42; 95% confidence interval [CI]: −0.07–0.92, P < 0.001; Supplementary Figure S1A) and after PSM (3.16% vs 4.43%; HR, 0.63; 95% CI: −0.18–1.44, P = 0.260; Supplementary Figure S1B). Cancer accounted for 10 of the 37 deaths in the OPCAB group and for 3 of 28 deaths in the PCI group. Before and after PSM, there was no significant difference in the incidence of cardiac mortality between the PCI and the OPCAB groups (1.0% vs 1.37% and 1.27% vs 1.27%, respectively; Supplementary Figure S2A, Figure 2(a)).
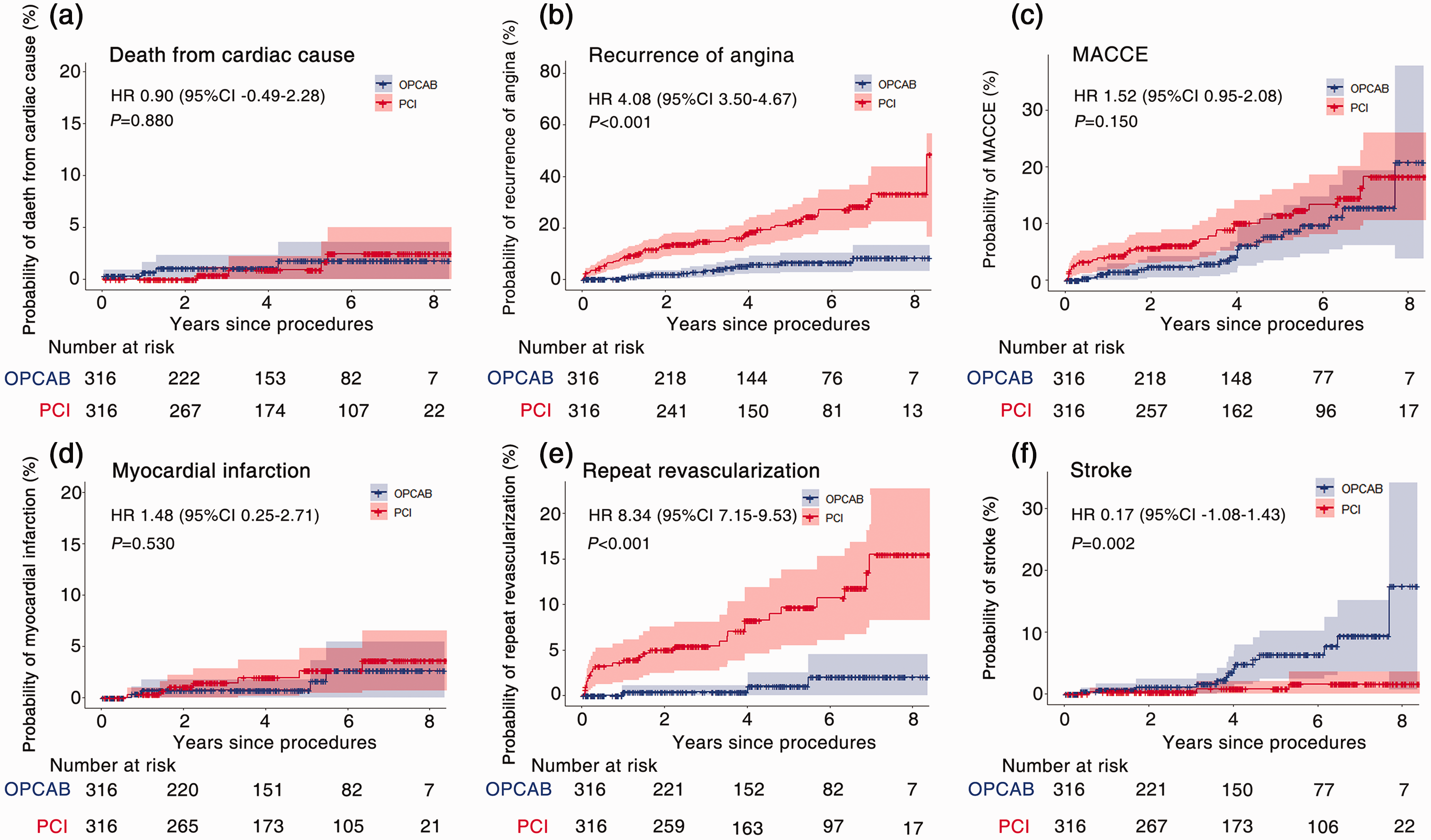
Kaplan–Meier curves of follow-up outcomes after propensity score matching. (a) Death from cardiac cause; (b) recurrence of angina; (c) MACCE; (d) myocardial infarction; (e) repeat revascularization; and (f) stroke. OPCAB, off-pump coronary artery bypass grafting; PCI, percutaneous coronary intervention; HR: hazard ratio; CI: confidence interval; MACCE: major adverse cardiac and cerebrovascular events.
After PSM, the recurrence of angina (HR, 4.08; 95% CI: 3.50–4.67, P < 0.001; Figure 2(b)) and repeat revascularization (HR, 8.34; 95% CI: 7.15–9.53, P < 0.001; Figure 2(e)) were significantly higher in the PCI group than in the OPCAB group. There was no significant difference in the incidence of MACCE (HR, 1.52; 95% CI: 0.95–2.08, P = 0.150; Figure 2(c)) or non-lethal MI (HR, 1.48; 95% CI: 0.25–2.71, P = 0.530; Figure 2(d)) between the groups. The incidence of stroke was significantly higher in the OPCAB group than in the PCI group (HR, 0.17; 95% CI: −1.08–1.43, P = 0.002; Figure 2(f)).
Subgroup analysis
All patients were divided into the TVD subgroup or LM+TVD subgroup according to the type of coronary artery lesions. All-cause mortality in the PCI group appeared to be lower than that in the OPCAB group in the TVD and LM+TVD subgroups (HR, 0.55; 95% CI: −0.41–1.52, P = 0.220 and HR, 1.44; 95% CI: −0.36–2.65, P = 0.860, respectively), but the difference was not significant (Figures 3(a) and 4(a) and Tables 4 and 5). Cardiac mortality was similar in the OPCAB and PCI groups in both subgroups (Figure 5 and Tables 4 and 5).

Kaplan–Meier curves of follow-up outcomes in the subgroup analysis of triple-vessel disease. (a) Death from any cause; (b) recurrence of angina; (c) MACCE; (d) myocardial infarction; (e) repeat revascularization; and (f) stroke. OPCAB, off-pump coronary artery bypass grafting; PCI, percutaneous coronary intervention; HR: hazard ratio; CI: confidence interval; MACCE: major adverse cardiac and cerebrovascular events.

Kaplan–Meier curves of follow-up outcomes in the subgroup analysis of left main disease with triple-vessel disease. (a) Death from any cause; (b) recurrence of angina; (c) MACCE; (d) myocardial infarction; (e) repeat revascularization; and (f) stroke. OPCAB, off-pump coronary artery bypass grafting; PCI, percutaneous coronary intervention; HR: hazard ratio; CI: confidence interval; MACCE: major adverse cardiac and cerebrovascular events.
Subgroup analysis of triple-vessel disease.

OPCAB, off-pump coronary artery bypass grafting; PCI, percutaneous coronary intervention; IQR, interquartile range; MACCE, major adverse cardiac and cerebrovascular events.
Subgroup analysis of left main disease with triple-vessel disease.

OPCAB, off-pump coronary artery bypass grafting; PCI, percutaneous coronary intervention; IQR, interquartile range; MACCE, major adverse cardiac and cerebrovascular events.

Kaplan–Meier curves of cardiac-cause mortality after subgroup analysis. (a) Kaplan–Meier curves of death from cardiac causes for subgroup analysis of triple-vessel disease; and (b) Kaplan–Meier curves of death from cardiac causes for subgroup analysis of left main disease with triple-vessel disease. OPCAB, off-pump coronary artery bypass grafting; PCI, percutaneous coronary intervention; HR: hazard ratio; CI: confidence interval.
In the TVD subgroup (Table 4 and Figure 3), the incidence of recurrence of angina (HR, 4.26; 95% CI: 3.61–4.91, P < 0.001) and repeat revascularization (HR, 10.19; 95% CI: 8.75–11.63, P < 0.001) was significantly lower in the OPCAB group than in the PCI group. The incidence of stroke was significantly lower in the PCI group than in the OPCAB group (HR, 0.12; 95% CI: −1.39–1.62, P = 0.001).
In the LM+TVD subgroup (Table 5 and Figure 4), the incidence of recurrence of angina (HR, 3.06; 95% CI: 1.70–4.42) and repeat revascularization (HR, 3.73; 95% CI: 1.46–6.01) appeared to be lower in the OPCAB group than in the PCI group, but this not significant. The incidence of stroke (HR, 0.61; 95% CI: −1.80–3.02) was also not significantly different between the two groups.
Discussion
This study compared the clinical efficiency of OPCAB and second-generation DESs with PCI in the treatment of LM and/or TVD. We found that the incidence of stroke at 4 years appeared to be lower in the PCI group than in the OPCAB, but there were no significant differences in all-cause mortality, cardiac mortality, or non-lethal MI between the two groups. The incidence of repeat revascularization and recurrence of angina was lower in the OPCAB group than in the PCI group. A further stratified analysis according to the distribution of coronary artery lesions of (TVD vs LM+TVD) showed that all-cause mortality and cardiac mortality were similar following OPCAB or PCI. However, in the TVD subgroup, the incidence of recurrence of angina and repeat revascularization was higher in the PCI group than in the OPCAB group. Although the incidence of MACCE and non-lethal MI was slightly higher in the PCI group than in the OPCAB group, these differences were not significant. Furthermore, there was no significant difference in any of the outcomes in the LM+TVD subgroup between the two different therapeutic modalities.
Our study showed a trend toward higher all-cause mortality after OPCAB. After the subgroup analysis, all-cause mortality still showed a higher trend in the OPCAB group than in the PCI group, but this difference was not significant. The SYNTAX trial was the first randomized trial to compare CABG and PCI in patients with complex coronary disease. 13 The 5-year results of the SYNTAX trial showed that all-cause death was not significantly different between the groups (11.4% in the CABG group vs 13.9% in the PCI group; P = 0.10). CABG was superior to PCI in patients with anatomically complex coronary artery disease. 13 In the SYNTAX trial, 10-year follow-up data showed no significant difference in all-cause mortality between PCI with first-generation eluting stents and CABG. However, CABG provided a survival benefit in patients with TVD. 14 The Nordic–Baltic–British Left Main Revascularization (NOBLE) trial and Evaluation of XIENCE versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization (EXCEL) trial are currently the most influential, randomized, controlled trials for patients with LMCAD.7,8 In the EXCEL trial, the mortality at 5 years was higher in the PCI group than in the CABG group, which likely reflects the enrolment of patients with complex bifurcation lesions in this trial. 7 Marui et al. 15 compared PCI with OPCAB in patients with multivessel disease in Japan and found that the OPCAB group had better long-term survival at a median of 3.5 years of follow-up when bare metal stents were used for PCI. The advantage of OPCAB was not apparent until after 5 years. Some studies have shown that the incidence of all-cause mortality and MACCE after OPCAB or PCI gradually increases with age.16,17 The mean age of the patients in Marui et al.’s 15 study was 67.9 years, which is older than the mean age in our study (64 years); therefore, the advantage of OPCAB was observed earlier in the same follow-up period. In another study with a follow-up of only 2 years, no difference in all-cause mortality was found between the two treatment modalities. 18 After further analysis, we found that the proportion of patients who died of cancer was higher in the OPCAB group than in the PCI group after PSM, which may have contributed to the higher rate of death from any cause in our OPCAB group.
MACCE are important adverse events of concern in the field of cardiac surgery. The 5-year follow-up results of the SYNTAX trial showed that the incidence of MACCE, non-lethal MI, and repeat revascularization in the CABG group was significantly lower than that in the PCI group (all P < 0.001). 13 In a Japanese study of patients with TVD, the rate of MACCE was higher with second-generation DESs than with CABG (P < 0.001) owing to higher rates of non-lethal MI and repeat revascularization. 11 The 3-year follow-up results of the FAME 3 trial showed that the incidence of non-lethal MI (P = 0.02) and repeat revascularization (P < 0.001) in the PCI group was higher than that in the OPCAB group. 9 In the current study, the incidence of repeat revascularization was higher in the PCI group than in the OPCAB group (Figure 2(e)), which is consistent with most previous findings. There was no significant difference in the incidence of MACCE or non-lethal MI between the two different therapeutic modalities, but there appeared to be higher trends of MACCE (Figure 2(c)) and non-lethal MI (Figure 2(d)) in the PCI group.
There was no difference in the incidence of stroke at any time in the first 2 years after OPCAB or PCI. Thereafter, the incidence of stroke was higher in the OPCAB group than in the PCI group. This finding likely reflects the higher peripheral vascular disease burden noted preoperatively in the OPCAB group. In this study, the ascending aorta was partially clamped by lateral-side bite clamping to achieve partial occlusion of blood flow. Previous studies have shown a direct relationship between the risk of stroke and the degree of aortic manipulation.19,20 Additionally, a higher stroke incidence may have occurred in the OPCAB group because of the shorter duration of aspirin and clopidogrel combination than that in the PCI group. The late difference in stroke incidence was unlikely to be due to the mode of revascularization, particularly because of the finding of the higher incidence of repeat revascularization and MACCE in the PCI group. The incidence of stroke may be reduced by using bilateral internal mammary arteries as in situ for OPCAB or using a proximal aortic anastomosis device (e.g., U-CLIP) to minimize manipulation of the proximal aorta. The absence of aortic manipulation (“anaortic” technique) may provide additional neurological protection. 19
Currently, OPCAB is associated with a lower incidence of adverse events and provides a considerable survival benefit in patients with multivessel disease. 21 The internal mammary artery is usually chosen as the arterial conduit for bypass grafting in OPCAB. This artery is usually anastomosed beyond the diseased segments, bypassing complex and diffuse atherosclerotic lesions, while PCI treats focal lesions only. The pedicled internal mammary artery can regulate blood flow according to physiological activities, 22 and it also secretes nitric oxide, which has vasodilatory and anti-platelet accumulation effects. 23 In addition, the internal mammary artery rarely develops atherosclerosis and has higher long-term patency.24,25
This study has some limitations. The number of patients was relatively small, and the follow-up time of some patients was short. This study was a single-center, retrospective study. PSM cannot account for all selection biases. Several types of second-generation DESs were used, which may also have affected the results in the PCI group. The anatomical characteristics and disease severity of the native coronary artery, such as the lesion length and degree of calcification, were analyzed. The heterogeneity of patients was addressed by using PSM, but this can account only for known and measured confounders.
Conclusions
In patients with LM and/or TVD, the survival rate is not significantly different between OPCAB and PCI with second-generation DESs. The incidence of MACCE appears to be lower in patients with OPCAB than in those with PCI and second-generation DESs, possibly caused by a lower incidence of non-lethal MI, recurrence of angina, and repeat revascularization. OPCAB and PCI provide different benefits in our Chinese population with LM and/or TVD, and these should be explained to patients during the decision-making processes. OPCAB may be a favorable coronary revascularization strategy for LM and/or TVD. Further randomized, controlled trials are required to confirm this hypothesis.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241304545 - Supplemental material for Off-pump coronary artery bypass grafting versus percutaneous coronary intervention with second-generation drug-eluting stents for coronary artery revascularization
Supplemental material, sj-pdf-1-imr-10.1177_03000605241304545 for Off-pump coronary artery bypass grafting versus percutaneous coronary intervention with second-generation drug-eluting stents for coronary artery revascularization by Nan Li, Xin Xiong, Kun Yang, Yijun Xu, Zhiqiang Chen, Peng Liu, Wen Wen, Xiaowei Li, Jin Dong, Shoudong Wei, Durong Chen, Xiaolong Zhang, Dajiang Yuan and Yongzhi Deng in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605241304545 - Supplemental material for Off-pump coronary artery bypass grafting versus percutaneous coronary intervention with second-generation drug-eluting stents for coronary artery revascularization
Supplemental material, sj-pdf-2-imr-10.1177_03000605241304545 for Off-pump coronary artery bypass grafting versus percutaneous coronary intervention with second-generation drug-eluting stents for coronary artery revascularization by Nan Li, Xin Xiong, Kun Yang, Yijun Xu, Zhiqiang Chen, Peng Liu, Wen Wen, Xiaowei Li, Jin Dong, Shoudong Wei, Durong Chen, Xiaolong Zhang, Dajiang Yuan and Yongzhi Deng in Journal of International Medical Research
Footnotes
Acknowledgements
We thank Dr. Hugh Peterson for helping to improve the grammar of the manuscript.
Author contributions
Nan Li contributed to collection and writing the manuscript; Xin Xiong and Kun Yang contributed to data collection; Yijun Xu, Zhiqiang Chen, Peng Liu, Wen Wen, and Xiaowei Li assisted in the OPCAB procedures; Jin Dong and Shoudong Wei are cardiologists who performed PCI; Durong Chen was responsible for the statistical analysis; Xiaolong Zhang is an anesthesiologist and was responsible for the patient’s anesthesia; Dajiang Yuan is an expert in critical care medicine and greatly contributed to the conception and design of the study; Yongzhi Deng performed the surgical procedures, obtained funding, and was involved in the conception and design of the study, analysis and interpretation of the results, and critical revision of the manuscript. All authors have approved the manuscript for submission.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This work is supported by the Key Research and Development Program of Shanxi Province (201903D321176).
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.