
Abstract
Over the past few years, the correlation between periodontal disease (PD) and polycystic ovary syndrome (PCOS) has attracted widespread attention owing to the increased incidence of these diseases. Several studies have suggested a possible link between the two. In this narrative review, we examined the epidemiology, common risk factors, and pathological mechanisms of PCOS and PD to investigate the potential association between these diseases. Evidence from the literature indicates that PCOS and PD can interact with each other. Common risk factors, such as microbial homeostasis imbalance owing to dysbiosis, along with multiple hormone and inflammatory mediators, as well as inflammatory responses owing to oxidative stress and oxidative responses owing to ferroptosis, are all associated with the pathogenesis of both diseases. Further studies are needed to clarify the specific mechanisms of interaction between PCOS and PD, which could clarify future directions in disease management and combined multidisciplinary treatment.
Keywords
Introduction
Polycystic ovary syndrome (PCOS) is a common endocrine and reproductive disorder that manifests as hyperandrogenism, polycystic ovarian morphology, and ovulatory dysfunction, affecting approximately 6% to 10% of women. 1 This syndrome is frequently associated with a range of metabolic abnormalities, including atherosclerosis, insulin resistance, obesity, dyslipidemia, and an increased risk of cardiovascular disease. 2 Although the exact pathogenesis of PCOS remains unclear, emerging evidence suggests that genetic predisposition and adipokines (proteins secreted by adipose tissue) are involved in metabolic regulation and that various inflammatory and anti-inflammatory mediators may have important roles in the development and progression of PCOS.3,4 Periodontal disease (PD) is a chronic inflammatory disease caused by bacterial infection, characterized mainly by progressive loss of periodontal tissue. PD development is closely associated with systemic diseases. In recent years, many studies5,6 have focused on the latent association between PCOS and PD, which may have an interplay and mutually reinforcing relationship in the development of these diseases.
The aim of this narrative review was to inquire into the potential association between PCOS and PD, focusing on their shared risk factors and associated pathogeneses, with the aim of guiding research and treatment strategies for both diseases (Figure 1).
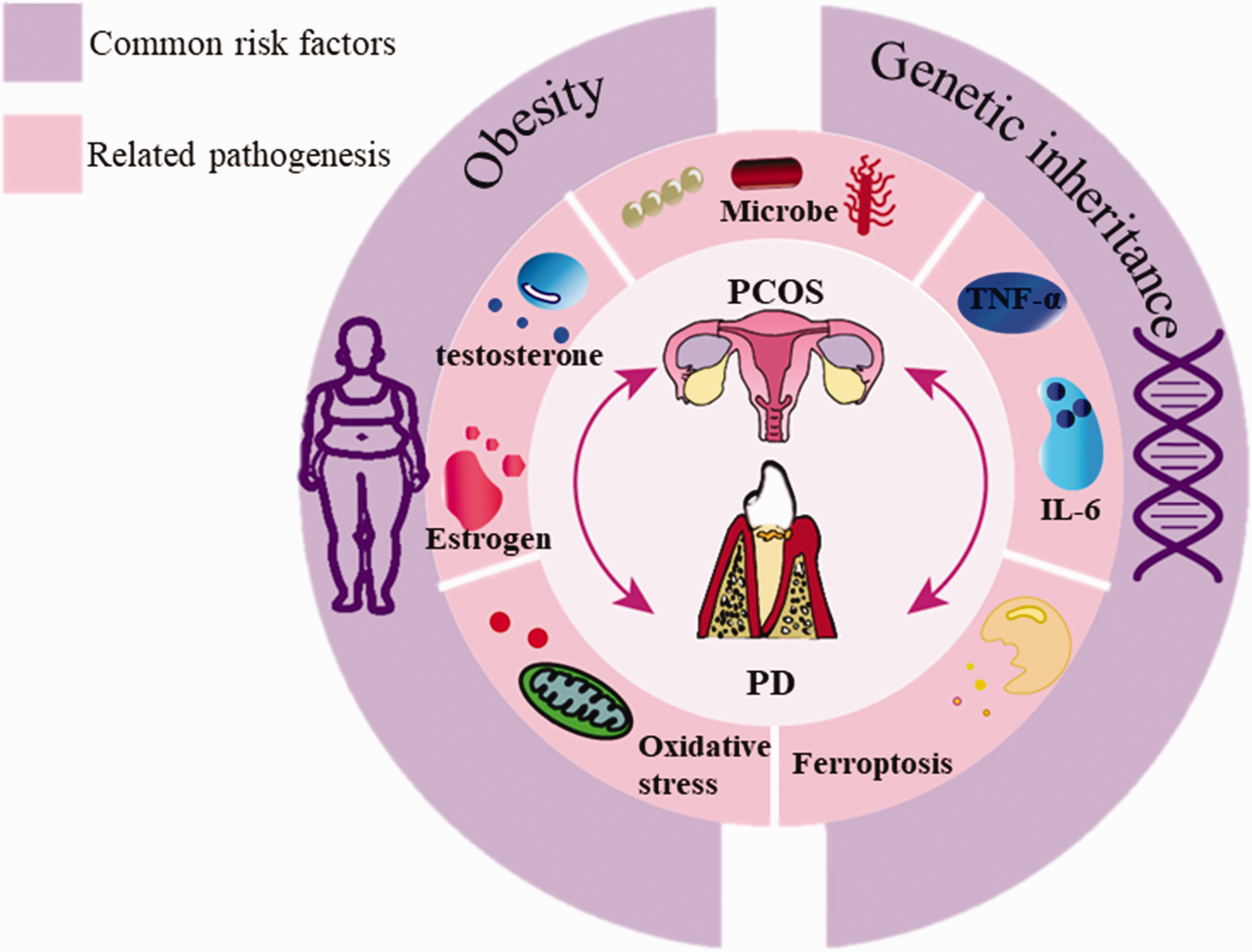
Correlation between periodontal disease (PD) and polycystic ovary syndrome (PCOS).
Literature review
In this narrative review, we conducted a literature search using PubMed, EMBASE, Google Scholar, and Up To Date for articles on PCOS and PD. The search was narrowed to articles published between 2010 and 2023. A total of 25 articles matched the inclusion criteria and were enrolled in this study. This review was guided by the Scale for the Assessment of Narrative Review Articles (SANRA). 7 Because this study was a review, ethics approval and informed consent were not required.
Epidemiological evidence
International studies have reported that the prevalence of PCOS among women of childbearing age ranges from 6% to 10%. 1 Approximately 10% of adults worldwide have PD, and severe periodontitis is recognized as the sixth most prevalent disease worldwide. 8 Several studies have demonstrated a close correlation between the development of PCOS and PD. In 2019, Tong et al. conducted a retrospective cohort study 9 among 24,410 women, with an equal number having and not having PD. In that study, 441 patients with PCOS were included in the PD group and 304 patients with PCOS were included in the control group. The prevalence of PCOS was significantly higher among patients with PD than that in the control group (p < 0.001). Furthermore, in a survey by Işık et al., 6 a total of 116 patients with PCOS between the ages of 18 and 24 years were included, along with 90 healthy controls. The results revealed that the periodontal probing depth was greater in the PCOS group for all subphenotypes. However, the remaining periodontal parameters (gingival index, plaque index, periodontal bleeding percentage on probing, and clinical attachment level) did not exhibit statistical significance when compared with the control group. Patients with PCOS had a higher likelihood of comorbid PD compared with healthy women. According to a 2020 meta-analysis by Machado et al., 10 women with PCOS had a 28% increased risk of developing PD compared with the healthy population, and women with PD had a 46% increased risk of developing PCOS compared with healthy controls. Additionally, women with PCOS exhibited a greater probability of gingival bleeding than women without PCOS. Furthermore, periodontal pocket depth and loss of clinical attachment were higher in women with PCOS than in those without PCOS. Additionally, that study found that women with PCOS were associated with clinical features and inflammatory deterioration in PD. The epidemiologic evidence indicates that the prevalence of PCOS is significantly higher in patients with PD and also that the prevalence of PD is higher in patients with PCOS than in healthy individuals; thus, these two conditions are closely linked and there may be an interaction between them.
Common risk factors
Obesity
With rapid socioeconomic development, obesity has emerged as a prevalent health concern. According to World Health Organization standards, individuals with a body mass index (BMI) of 25 kg/m2 or higher are classified as having abnormal body weight, and those with a BMI exceeding 30 kg/m2 are considered obese. 11 Obesity is a systemic low-grade inflammatory state that has adverse impacts on systemic bone metabolism and bone remodeling. 12 Several studies have revealed an association between obesity and decreased bone mass, potentially leading to alveolar bone resorption and the development of PD. 13 A meta-analysis conducted by Kim et al. 14 corroborated these findings, confirming that obesity heightens the risk of developing PD. Adipose tissue functions not only as an energy storage organ but also as an endocrine organ, secreting a variety of cytokines including leptin, adiponectin, resistin, lipocalin, interleukin (IL), and tumor necrosis factor alpha (TNF-α). 15 A heightened secretion of cytokines regulates the body's immune response and triggers inflammatory mediators in periodontal tissues, subsequently leading to periodontal tissue damage.
The pathogenesis of PCOS is closely related to endocrine imbalance. Therefore, some scholars believe that there is a close bidirectional relationship between PCOS and obesity, and that an increase in BMI will increase the risk of PCOS. 16 A genetics-based study by Venkatesh et al. 17 suggested that obesity contributes to increased susceptibility to reproductive diseases in women. Obesity disrupts the healthy homeostasis of the body, and the development of PCOS and PD becomes more likely in this situation. Therefore, in patients with PCOS or PD, improving lifestyle habits, adjusting dietary intake, and engaging in physical exercise are important.
Genetic correlation
Both PCOS and PD exhibit familial aggregation, suggesting a potential genetic correlation between the two diseases. Peroxisome proliferator-activated receptor γ (PPARγ), a subtype of PPAR that is abundantly expressed in adipose tissue, requires ligand activation for its function. PPARγ plays a crucial role in regulating adipocyte metabolism and insulin sensitivity by modulating glycolipid metabolism. 18 Polymorphisms in the PPAR-g gene are associated with both PCOS and PD, 19 suggesting a potential gene-level correlation between the two conditions. Furthermore, polymorphisms in PPAR-g, PPARGC1A, and CYP11A1, along with immune-related genes in adipose tissue, peripheral blood, and ovarian tissue, are closely linked to genetic susceptibility to PD. These genetic variations may also play a role in regulating PCOS and insulin sensitivity. 20 The genetic association between PCOS and PD could be emphasized in the prevention and diagnosis of these diseases in the future.
Interaction mechanisms between PCOS and PD
Dysbiosis
With periodontal pathogenic bacteria as the initiating factor of periodontitis, in the periodontal environment, the microbial community structure changes from parthenogenetic anaerobic to anaerobic, which disrupts the dynamic ecological balance of the periodontal biofilm, activates an exaggerated immune response in the body, and induces an inflammatory reaction in the periodontal tissue by releasing a large number of inflammatory mediators.
Fusobacterium nucleatum is a gram-negative anaerobic bacterium commonly found in both supragingival and subgingival biofilms. F. nucleatum plays a pivotal role in the pathogenesis of periodontitis by acting as a bridge, facilitating the colocalization of periodontally pathogenic bacteria and promoting plaque biofilm maturation. F. nucleatum expresses various bacterial virulence factors, including adhesion protein (Fad A), lipopolysaccharide, and fibroblast activation protein-2. Fardini et al. discovered that F. nucleatum binds directly to vascular endothelial calreticulin 415-534 via Fad A, thereby altering its intracellular distribution and inducing intracellular migration, ultimately enhancing vascular endothelial cell permeability. Enhanced permeability of vascular endothelial cells facilitates the passage of F. nucleatum through the vascular endothelium, enabling its dissemination to organs throughout the body via the bloodstream. Escherichia coli, a conditionally pathogenic bacterium found in the digestive tract, can breach the vascular barrier and enter the bloodstream when the body's immunity is compromised. In F. nucleatum infection, Fad A disrupts the integrity of the cellular barrier, leading to increased penetration of E. coli into the vascular endothelium. This suggests that F. nucleatum infection and colonization promote invasion and infection of the organism by other bacteria.21,22 F. nucleatum disrupts the epithelial barrier and engages in an assault on lymphocytes, resulting in an imbalance in host immunity and the subsequent destruction of periodontal tissues. In a study by Li N et al., 23 saliva and fecal samples from 10 patients with PCOS and 10 healthy controls were subjected to 16S rRNA gene amplicon sequencing. Saliva samples were collected at 6-hour intervals over a 24-hour period (Zeitgeber [ZT]0, ZT6, ZT12, and ZT18). The analysis revealed an increase in F. nucleatum counts and a decrease in Actinomycetes counts in the saliva microbiomes of patients with PCOS. This suggests a close association between F. nucleatum—a recognized major periodontal pathogen—and the development of PCOS.
Actinomycetes have a crucial role in maintaining microbial homeostasis in the oral cavity, and these organisms are typically more abundant in periodontal tissues during periods of health, as compared with inflammatory states. Watanabe et al. showed 24 that swallowing or oral administration of Porphyromonas gingivalis decreased the abundance of P. gingivalis in the mouse intestine. Additionally, butyric acid production affected P. gingivalis abundance and both the abundance of Turicibacter and insulin sensitivity while increasing the abundance of Deferribacterales; this in turn caused abnormalities in iron metabolism and influenced insulin function by significantly downregulating expression of the AKT gene and affecting the phosphoInositide-3 kinase/protein kinase B pathway, thereby promoting insulin resistance (IR). IR is also strongly associated with abnormal metabolic levels and ovarian function in patients with PCOS. Bao et al. 25 demonstrated that P. gingivalis and F. nucleatum were enriched in the gut microbiota of mice with severe periodontitis. Moreover, transplantation of periodontopathogenic bacteria into the colon induced the upregulation of pro-inflammatory cytokines and chemokines in mice, subsequently triggering colonic inflammation. Dong et al. 26 demonstrated that oral administration of P. gingivalis to mice induced alterations in both the composition and function of the intestinal microbiota, along with an increase in intestinal permeability. Mice given P. gingivalis exhibited alterations in serum metabolomic markers, including 5-hydroxyindoleacetic acid, indole-3-acetaldehyde, salicylic acid, and phosphatidylcholine, which were closely associated with changes in the gut microbiota. Owing to the existence of the oral–gut barrier, there are differences in the composition and distribution of the microbiota in the oral cavity and the intestinal tract. However, in the case of oral–gut barrier dysfunction, oral microorganisms and their products can be transmitted to the gastrointestinal tract through the swallowing of food and saliva, thereby affecting the microbiota that colonize the intestinal mucosa. At the same time, microorganisms from the intestinal tract can be transmitted through the oral cavity. Based on this interactive relationship, some scholars have put forward the notion of an “oral–gut axis.” 27
Endocrine disruption in PCOS may increase the risk of PD by altering the composition of the oral microbiota. Simultaneously, oral pathogens can migrate to the gut, rendering individuals more susceptible to PCOS by modifying the gut microbiota and augmenting intestinal permeability. However, further studies are needed to elucidate the mechanisms via which dysbiosis of the oral flora induced by PD interacts with PCOS.
Changes in hormone levels
Hyperandrogenemia (HA) is characterized by the excessive secretion or production of androgens and serves as the primary feature of PCOS. This alteration in androgen levels adversely impacts periodontitis by reducing the keratinization of gingival epithelial cells and enhancing the permeability of blood vessels in gingival tissue. 28 Alongside the production of elevated androgen levels, there is also a decrease in estrogen and IR. 29 Estrogen, a steroid hormone, has a pivotal role in regulating the proliferation and differentiation of osteoblasts and suppressing osteoclast production by enhancing osteoprotegerin (OPG) synthesis in osteoblasts. Furthermore, estrogen can exert an inhibitory effect on bone tissue cells, reducing the production of inflammatory mediators such as IL and TNF-α. 30 Estrogen deficiency leads to increased levels of inflammatory mediators. In vitro experiments 31 involving the observation of ovariectomized rats over a period of 90 days revealed a certain degree of alveolar bone loss. The absence of ovaries in these rats may bring about the loss of periodontal bone tissue. This suggests that abnormal hormone levels in patients with PCOS may induce alveolar bone destruction or infiltration of inflammatory mediators into periodontal tissues, thereby contributing to the development of PD. Further investigation is warranted to elucidate the specific mechanism by which PCOS and PD interact via hormone levels.
Inflammatory mediators
Both PCOS and PD share common inflammatory features characterized by a non-specific, persistent, mild inflammatory state. Inflammatory mediators are strongly associated with the development of both PCOS and PD. The pathogenesis of both PD and PCOS involves the release and activation of inflammatory mediators, including C-reactive protein, IL, TNF-α, and matrix metalloproteinase-9. 32 The release and activation of inflammatory mediators such as IL-6 and TNF-α contribute to exacerbation of the inflammatory response in periodontal tissues, leading to increased periodontal tissue destruction, and ultimately, tooth loosening and loss. 33
Inflammatory mediators can also induce IR through multiple pathways, consequently influencing the pathogenesis of both PCOS and PD. TNF-α activates serine/threonine protein kinase, promoting serine phosphorylation and competitively inhibiting tyrosine phosphorylation of insulin receptor substrates (IRS), resulting in insulin dysfunction and ultimately IR. Furthermore, TNF-α-induced activation of protein tyrosine phosphatase-1B results in dephosphorylation of the insulin receptor and IRS, inhibiting their binding and causing aberrant insulin signaling. Some studies 34 indicate that decreased TNF-α protein expression improves insulin-stimulated protein kinase B (AKT) phosphorylation in HepG2 cells and attenuates lipid-induced IR in diabetic hepatocytes. IL-6 can exacerbate inflammation and ultimately induce insulin suppression by activating the nuclear factor-κB (NF-κB) inflammatory cascade response in hepatic, muscular, and adipose tissues. 35 Previous studies 36 have demonstrated a correlation between periodontal infection and IR, an important pathophysiological feature and key pathogenic mechanism of PCOS. These studies collectively suggest that PCOS and PD may share similar underlying mechanisms.
Oxidative stress
Oxidative stress (OS) is an important factor in the body's inflammatory response, resulting from the failure to remove excess reactive oxygen species (ROS) in a timely manner and owing to an imbalance in the antioxidant mechanism. Excessive accumulation of ROS induces a state of OS, promoting oxidative damage and apoptosis, ultimately resulting in tissue damage. 37 Inflammation induced by OS plays a key role in the pathogenesis of chronic diseases, including diabetes. Several studies 38 have demonstrated a close association between OS and PCOS. The OS status in patients with PCOS can be evaluated by assessing markers such as malondialdehyde and total antioxidant capacity. Mitochondria are involved in metabolic processes via oxidative phosphorylation, which may become dysfunctional owing to genetic mutations. Some studies 36 have demonstrated significantly elevated levels of malondialdehyde and excess ROS in patients with PCOS compared with controls, alongside significantly reduced mitochondrial membrane potential, indicating a potential link between high malondialdehyde levels and IR in these patients. Therefore, it can be inferred that OS has an important role in the pathogenesis of PCOS.
NF-κB has a crucial role in mediating the responses to inflammation, stress, and immunomodulation as a key intracellular nuclear transcription factor. OS can lead to overactivation of the NF-κB pathway, thereby influencing inflammatory factors such as TNF-α and IL-1, ultimately resulting in systemic inflammation and inflammatory responses. 39 Tamaki et al. 40 found a positive correlation between the degree of periodontal tissue attachment loss in patients with periodontitis and serum levels of ROS metabolites, along with serum Porphyromonas antibody titers. That is, the degree of periodontal tissue attachment loss was positively correlated with serum ROS metabolite levels, with higher serum Porphyromonas antibody titers. P. gingivalis, the main causative agent of periodontitis, triggers an immune defense response that activates neutrophil chemotaxis and phagocytosis, resulting in local and systemic overproduction of ROS, as well as massive production of proinflammatory factors. This process also leads to elevated levels of the NF-κB receptor activator of the NF-κB ligand/OPG ratio, thereby increasing the number and activity of osteoclasts. Ultimately, these changes culminate in the destruction and loss of periodontal tissue. 41 OS damages vascular endothelial cells and elevates ROS levels, thereby stimulating the release of proinflammatory factors including TNF-α, IL-6, IL-8, and NF-κB. This inflammatory response leads to the development of systemic diseases and also acts locally on periodontal tissues, leading to their destruction. 37
Ferroptosis
Ferroptosis is a modifiable, non-natural apoptotic mode of cell death, the process of which is dependent on iron and ROS contributing to intracellular lipid peroxidation. 42 Ferroptosis is predicated on OS caused by abnormal iron metabolism, which is also an important factor in the body’s inflammatory response. Divalent iron ions in plasma can be oxidized to trivalent iron by ceruloplasmin. The resulting iron is bound to the transferrin receptor 1 complex for intracellular transport. Once inside the cell, it is reduced by the enzyme STEAP3 (six-transmembrane epithelial antigen of the prostate), and the reduced product is transported out of the cell by the membrane iron transport protein ferroportin. Ferroportin stores excess iron resulting from this process. Ferritin can undergo selective phagocytosis by lysosomes, where the bound iron is degraded into the cytoplasm, leading to the generation of large amounts of ROS through the Fenton reaction. This process, known as ferritin autophagy, is an important source of ROS in cells. 43
Autophagy-mediated ferroptosis serves as a crucial cell death mechanism implicated in various systemic diseases. Lipids present on cell membranes undergo peroxidation via both the Fenton pathway (non-enzymatic reaction) and the lipoxygenase pathway (enzymatic reaction). In these processes, polyunsaturated fatty acids (PUFA) are a key target of lipid peroxidation on cell membranes. This phenomenon primarily occurs owing to the influx of large quantities of iron ions and the direct or indirect inactivation of glutathione peroxidase 4 (GPX4). GPX4 uses glutathione as a substrate for its reduction reaction, a process that causes lipid peroxides to lose their peroxide activity, which may be interrupted when glutathione is depleted. GPX4 inhibitors and 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors, among others, can also lead to the inactivation of GPX4, thereby affecting the reduction reaction. 44 Intracellularly, ferroptosis primarily manifests as abnormal mitochondrial morphology, the accumulation of large amounts of ROS, and weakened antioxidant capacity. Mitochondrial dysfunction is considered a key factor leading to ROS generation, further contributing to the development of ferroptosis.
In a study by Li S et al., 45 32 women with PCOS and 34 healthy female controls were selected for a lipidomic study. The findings showed that levels of PUFA were abnormal in the PCOS group compared with healthy women. In particular, serum bioactive lipids downstream of arachidonic acid in the PCOS group were significantly lower than those in the healthy group. Phosphatidylethanolamine, a key phospholipid that leads to ferroptosis in cells, contains arachidonic acid, which could indicate that endocrine imbalance in patients with PCOS may contribute to ferroptosis. Zhang et al. 46 demonstrated that rats with PCOS, hyperandrogenism (HA), and IR exhibited abnormal metabolism and hormonal levels, leading to ferroptosis. Further investigation revealed lower expression of GPX4 and glutathione in the uterus and placenta of female rats compared with the normal group. Additionally, the expression of ferroptosis-related genes, including ACSL4, TFRC, SLC7A11, and GCLC, was significantly elevated. Ferroptosis-related abnormalities in mitochondrial morphology characteristics were also observed. In this way, the ferroptosis process was confirmed to occur in vivo among rats with PCOS, HA, and IR. Derangements in amino acid metabolism are characteristic of obese patients with PCOS, with notable changes observed in arginine, glutamine, and cysteine levels. Particularly, glutamine deficiency is closely associated with the development of ferroptosis. 47 Consequently, ferroptosis contributes to the development of PCOS.
Several research studies have demonstrated a close relationship between the development of PD and the ferroptosis process. Wang H et al. 48 found that ferroptosis can promote the development of PD by regulating genes. Guo et al. 49 confirmed that nuclear receptor coactivator 4-mediated ferritin autophagy plays a crucial role in the pathogenesis of periodontitis, with the degradation of ferritin promoting the generation of ROS in human periodontal fibroblasts. Ferroptosis induces OS and excessive production of ROS, resulting in cellular dysfunction, which subsequently promotes the development of PD. Therefore, inhibiting ferroptosis could potentially mitigate the inflammatory response in periodontal tissues. Moreover, abnormal iron metabolism has a key role in the remodeling and destruction of alveolar bone, contributing to alveolar bone resorption.
In conclusion, the ferroptosis process is important in the pathogenesis of both PCOS and PD, and there may be interactions between these two diseases mediated by this mechanism. However, the specific mechanisms underlying this interaction remain poorly understood, warranting further investigation (Figure 2).

Mechanism of ferroptosis. Fe, iron; CP, ceruloplasmin; TF, transferrin; TFR, transferrin receptor; STEAP, six-transmembrane epithelial antigen of the prostate; GPX, glutathione peroxidase; GSH, glutathione; HMG-CoA, 3-hydroxy-3-methyl glutaryl coenzyme A reductase; ROS, reactive oxygen species; OS, oxidative stress; TNF, tumor necrosis factor; PD, periodontal disease; PCOS, polycystic ovary syndrome.
Clinical treatment modalities
Periodontal treatment includes basic periodontal treatment, drug treatment, surgical treatment, and periodontal maintenance treatment. In the clinical treatment of periodontitis, the first step is to emphasize the importance of oral hygiene to patients, improve their oral health awareness, and carry out basic treatments such as supragingival cleaning, subgingival cleaning, and root planing. Local or systemic medication can be used for anti-inflammatory and anti-infection effects. When periodontitis progresses to the stage of abscess, periodontal surgery is needed to remove the infected lesion. 8
For the treatment of PCOS, the 2023 PCOS diagnosis and treatment guidelines suggest that combination oral contraceptives or metformin are the most effective medications. As for anti-androgen drugs in alternative regimens, the new 2023 guideline emphasizes that attention should be paid to adverse effects: spironolactone 25 to 100 mg/day has a low risk of adverse effects; cyproterone acetate at doses of ≥10 mg has an increased risk of meningiomas, among others; finasteride, flutamide, and bicalutamide have a risk of hepatotoxicity, among others. 50
In patients with PD as well as PCOS, periodontal treatment combined with use of drugs such as combined oral contraceptives or metformin has a positive effect on the condition of periodontal tissue and the systemic status of the patient.
Summary
A potential association exists between PCOS and PD, with evidence suggesting mutual influence and interaction between the two diseases. Addressing shared risk factors can have a beneficial effect on the prevention of both diseases in the future. The microbial homeostatic imbalance induced by dysbiosis, inflammatory mediators and hormones, OS-induced inflammatory responses, and the oxidative response triggered by the ferroptosis process, are all intricately linked to the development of both PCOS and PD.
Patients diagnosed with PD in conjunction with PCOS will benefit from a multidisciplinary treatment approach. Alongside standard periodontal treatments such as full-mouth supragingival cleaning, subgingival scraping, and other basic therapies, including periodontal surgery if necessary to manage the progression of periodontal inflammation, systemic therapy for PCOS should also be incorporated into the treatment regimen. Addressing metabolic abnormalities associated with PCOS can aid in controlling the progression of periodontal inflammation.
Currently, research on the specific pathophysiological interaction mechanism between PCOS and PD remains incomplete, necessitating a greater number of in-depth studies to enhance understanding and elucidate the specific association between the two diseases. Such studies are essential to provide effective guidance for the prevention and treatment of both PCOS and PD. Research evidence on the specific physiological and pathological interactions between PCOS and PD remains unclear. Existing studies involve issues such as small sample sizes and potential biases. Thus, researchers must expand sample sizes and conduct more in-depth studies to clarify these associations so as to provide effective guidance for the prevention and treatment of both PCOS and PD.
Footnotes
Acknowledgement
The authors greatly appreciate Dr. Xiaoping Lin, a respected professor at Shengjing Hospital of China Medical University, who contributed to the main idea of this manuscript.
Author contributions
Huishan Zhang: Investigation, Methodology, Validation, Visualization, Writing – Original Draft.
Xiaoping Lin: Conceptualization, Funding Acquisition, Project Administration, Supervision, Writing – Review and Editing.
Data availability statement
All data generated and analyzed during this study are included in the published article.
Declaration of conflicting interest
The authors declare that there is no conflict of interest
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.