
Abstract
Objective
We conducted a systematic review and meta-analysis to determine the prevalence of high-risk human papillomavirus (hrHPV) infection and its associated risk factors among Nigerian women.
Methods
Databases including PubMed, Web of Science, Scopus, and CINAHL were searched for studies published between 01 January 2001 and 31 December 2022, that had reported hrHPV infection and associated risk factors among women in Nigeria from ages of 25 to 65 years.
Results
Of the 136 records initially retrieved, 18 were eligible for analysis. The prevalence of hrHPV genotypes was 25%, and for hrHPV 16 and 18, were 9% and 10%, respectively. The prevalence of hrHPV among HIV+ve women was 71%. The most common risk factors for hrHPV were age at coitarche and multiple sex partners.
Conclusion
hrHPV prevalence is high in women in Nigeria and common among those HIV+ve. Rapid screening for hrHPV genotypes is recommended, and multivalent HPV vaccines should be considered for women.
Background
Human papillomavirus (HPV) is a relatively small virus linked to benign and malignant diseases of the cervix, penis, vulva, vagina, anus, and oropharynx.1,2 Globally, HPV infection has been identified as the most prevalent sexually transmitted disease. 3 A study estimated that in the general female population, 32% of 576,281 gynecologically healthy and unhealthy women were HPV carriers in 2011, and Asia and Africa were found to have the highest prevalence of 46% and 30%, respectively. 3
Cervical cancer is caused by a uterine cervix infection with the high-risk human papillomavirus (hrHPV) genotype.4,5 Epidemiological and genetic variables affect susceptibility to cervical hrHPV infection, persistence, and development into neoplasia. 5 Oral contraceptives, cigarette smoking, multiple sexual partners, and HIV co-infection are all well-established epidemiological risk factors for cervical hrHPV infection, but little is known about genetic risk factors. 4 While most HPV infections are eliminated spontaneously by the host's immune system in approximately two years, about 10% of infected individuals have persistent HPV infection with a high risk of developing epithelial cell abnormalities and consequential malignancies at the site of infection. 4 Cervical cancer is a significant public health concern, being the fourth most common cancer in women worldwide, with 604,127 new cases and 341,831 deaths estimated in 2020.6,7 In 2018, low and middle-income countries (LMICs) accounted for 84% of new cases and up to 90% fatalities worldwide.7,8
Since the discovery of the link between cervical cancer and HPV infection, much work has been done, especially in developed countries, to raise awareness about sexual behaviours and encourage early detection through widely accepted screening programs. 9 Furthermore, introducing a cytology-based screening program redefined the promptness in diagnosing cervical cancer and HPV infection. However, the significant decrease in cancer incidence occurred only when national call and recall systems enabled coverage of more than 70% prevalence. 10
In Nigeria, the narrative around cervical cancer is disheartening among women of reproductive age (15 to 45 years). Approximately 12,075 new cervical cancer cases are diagnosed annually (estimations for 2020) and cervical cancer is the second most common female cancer. 11 In addition, cervical HPV16 and HPV18 infection are predicted to be present in 3.5% of women in the general population at any given time, and both HPV16 and 18 are responsible for 66.9% of invasive cervical cancers. 11
Early detection and treatment of cancer and pre-cancerous lesions is the best way to avoid cervical cancer. However, the paucity of data on the burden and impact of hrHPV on cervical cancer in Nigeria has impeded the implementation of a screening program. 12 Therefore, we conducted a systematic review and meta-analysis according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) regulations 13 to determine the prevalence of hrHPV infection and its associated risk factors among women in Nigeria.
Methods
PubMed, Web of Science, Scopus, and CINAHL (Cumulative Index to Nursing and Allied Health Literature) databases were systematically searched for studies published between 01 January 2001 and 31 December 2022, that had reported hrHPV infection and associated risk factors among Nigerian women from 25 to 65 years of age. Only studies conducted in Nigeria were eligible for inclusion and the searches were done with no language restrictions. The review was registered with PROSPERO (CRD42022323327).
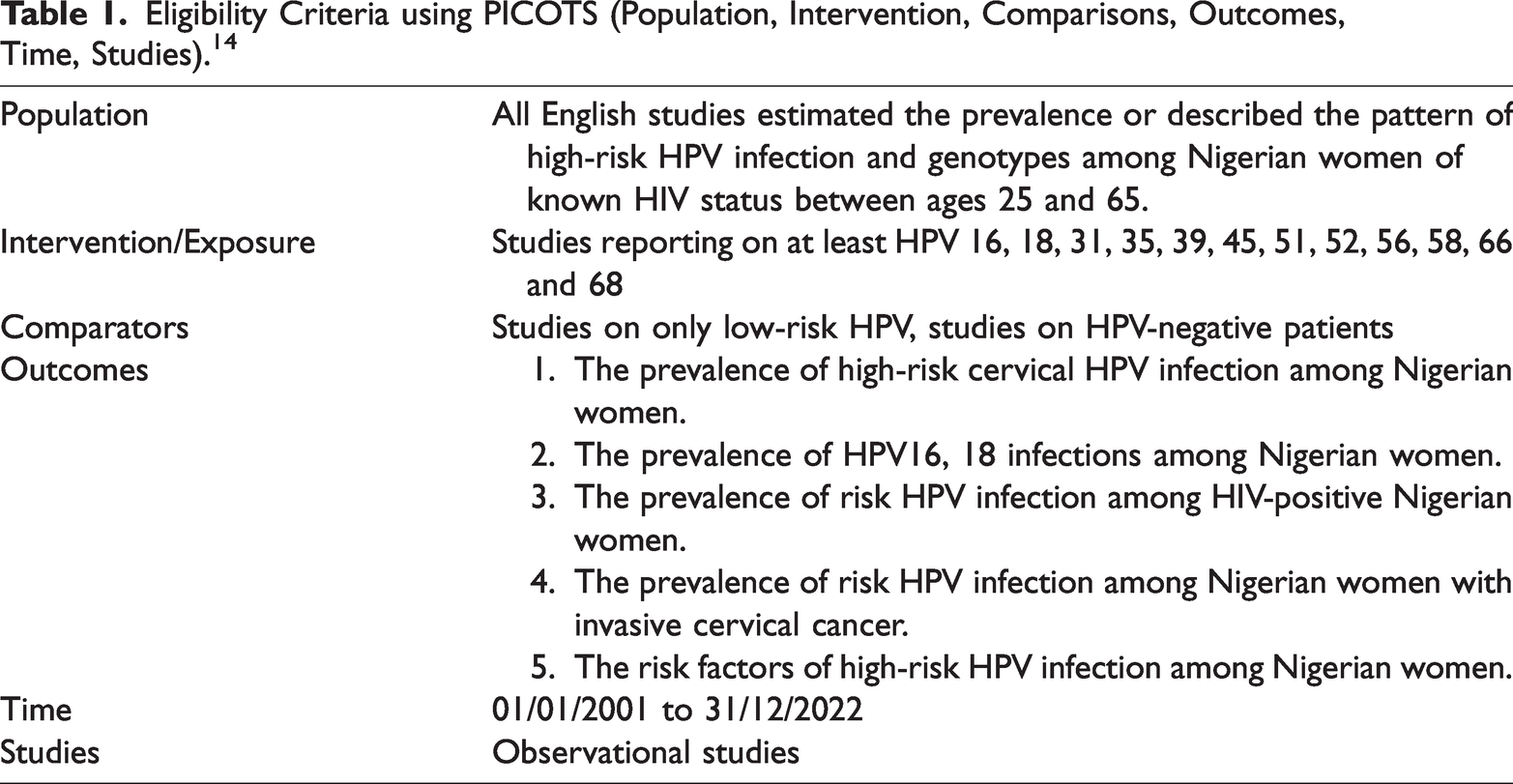
Key words/terms in both AND and OR combinations included: prevalence; seroprevalence; frequency; seroepidemiology; high-risk human papillomavirus; HPV; high-risk HPV; pap smear; co-testing; reflex HPV testing; cervical cancer; polymerase chain reaction; PCR; HPVs 16, 18, 31, 35, 39, 45, 51, 52, 56, 58, 66, 68; high-risk HPV genotypes; women; age 25 to 65 years; Nigeria. For a published report to be included in the meta-analysis, it had to fulfil the PICOTS framework (Population, Intervention, Comparators, Outcomes, Time, Studies). 14 The PICOTS search strategy for this study is shown in Table 1.
Eligibility Criteria using PICOTS (Population, Intervention, Comparisons, Outcomes, Time, Studies). 14
Studies selected were prospective, retrospective, cross-sectional, or case-control in design. In addition, the reference lists of all included studies were checked for any potential additional publications. Studies that met the eligibility criteria were included regardless of publication status (i.e., published, unpublished, or grey literature). Three reviewers [G.E., D.W., I.A.] independently screened the papers from their titles and abstracts removed duplicates and selected relevant studies. The reviewers then assessed the full text to determine if the study should be included. Two reviewers [O.A., I.A.] independently assessed the eligibility of the retrieved papers and resolved any disagreements by discussion or recourse to a third reviewer [G.E. or F.A.]. Two reviewers [I.A., O.A.] independently extracted data from the studies using a pre-tested data extraction form prepared in Microsoft Excel with any disagreement settled by a third reviewer [F.A.].
The following items were extracted: title; first author; publication date; region; study design; period of recruitment; sample size; inclusion criteria; number of abnormal cytology results; hrHPV genotype invasive cervical cancer; risk factors for hrHPV; age range. In addition, numbers of patients were recorded who were positive for: HPV; hrHPV; HIV; HPV16; HPV18; HPV31; HPV33; HPV35.
Primary outcomes of the meta-analysis were number of patients that were hrHPV+ve, followed by numbers hrHPV16+ve or hrHPV18+ve. The secondary outcomes were number of patients hrHPV31+ve, or hrHPV35+ve, and numbers testing +ve for other hrHPV types (i.e., 39, 45, 51, 52, 56, 58, 66, and 68) and risk factors for hrHPV infection. Other outcomes included the number of co-infections with HPV16 and 18 genotypes.
Two subgroup analyses were performed. The first assessed the prevalence of hrHPV positivity in different regions of Nigeria and the second assessed the prevalence of hrHPV positivity in women who were HIV+ve. Because this was a meta-analysis of previously published articles, ethical approval was not required.
Statistical analysis
The meta-analysis was performed using Review Manager (RevMan) [Computer program] Version 5.4.1. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration 2020. A P-value <0.05 was considered to indicate statistical significance.
Data were pooled from all eligible studies and hrHPV and associated risk factors (±95% confidence intervals [CIs]) were used as the effect size. The inverse variance method (Generic Inverse Variance) was used to calculate the pooled effect. For the assessment of risk factors, the Mantel–Haenszel method was used to calculate the odds ratio (OR) with 95% CIs.
Cochran's Q test and Higgins' I2 statistical test were used to assess the statistical heterogeneity of the pooled results. If I2 statistic ≥ 50% and P<0.01, a random effects model was applied to the data. If no heterogeneity was observed, a fixed effect model was to be used.
The methodological quality and risk of bias in the included studies was independently assessed by two authors [F.A., G.E.] using an adapted version of the NIH Quality Assessment Tool. Any discrepancies between reviewers were resolved by a third reviewer [M.O.] using an adapted version of the risk of bias tool for prevalence studies. 15 The tool consisted of nine domains, which were: description of the target population; sampling frame; sampling technique; response rate; non-proxy collection of data; case definition of study; validity of study instrument; reliability of study instrument; mode of data collection; an appropriate description of numerator and denominator for the parameter of interest. The total score for each study ranged from 0–9; bias was graded as follows: 0–3, high risk; 4–6, moderate risk; 7–9, low risk. A sensitivity analysis was to be performed omitting studies rated as ‘high risk’ of bias.
Results
Characteristics of included studies
Of the 136 records retrieved, 117 were from electronically published databases and 19 from grey literature, hand searches, and conference proceedings (Figure 1). After removing five duplicate records, 131 remained, from which 93 reports were excluded (74 from electronic databases and 19 grey reports) based on title and abstract. The full-text records for the remaining 38 studies were obtained for detailed evaluation. Of the 38 studies, 20 were excluded because one or more of the following applied: no information on hrHPV prevalence; the purpose of the study did not concern hrHPV prevalence among Nigerian women; no clear methodology. Therefore, 18 studies ultimately met the eligibility criteria.4,5,16–31
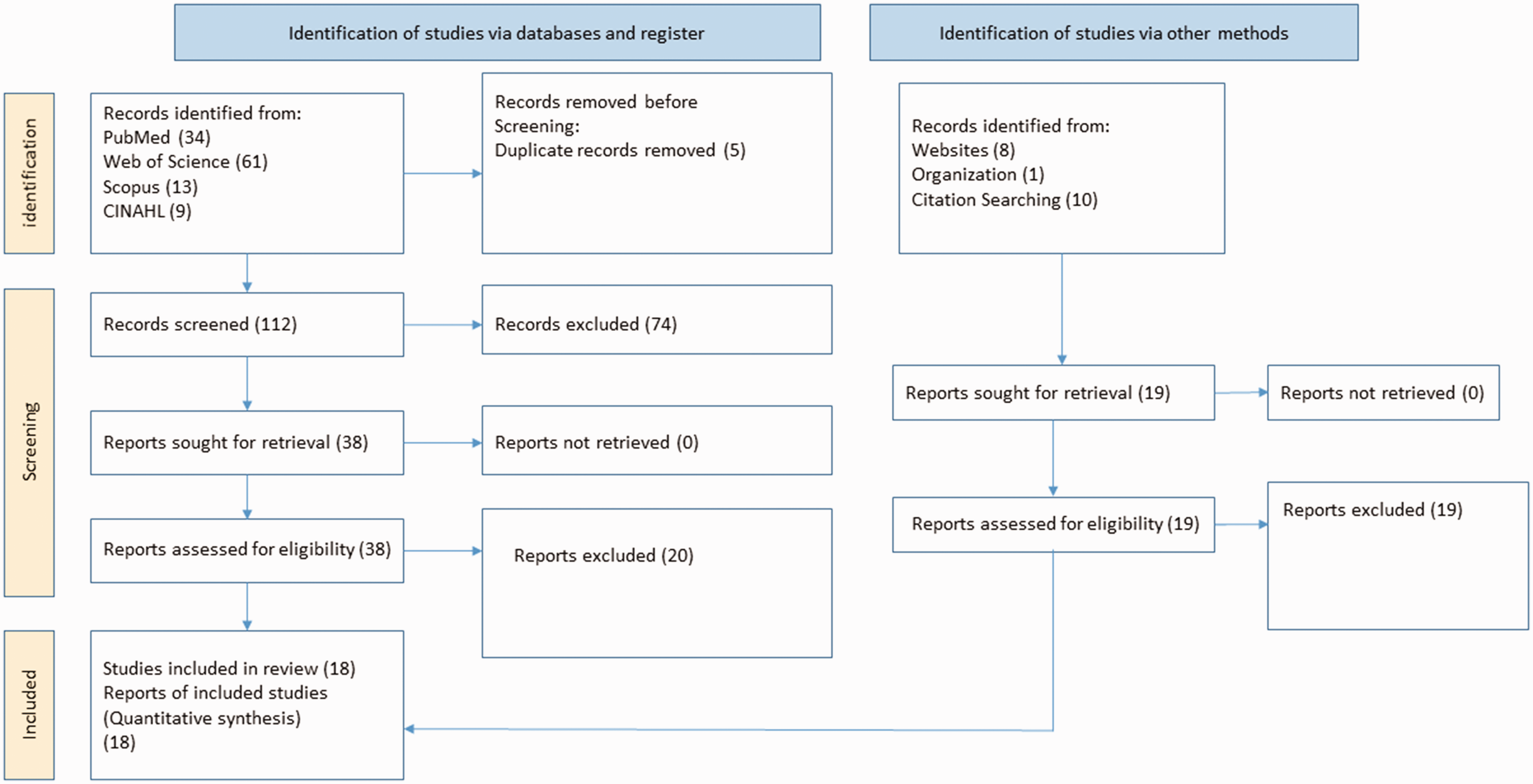
PRISMA flow diagram for the search results.
The main features of the 18 studies that involved 10,375 women are summarized in Table 2. Of the 18 studies, 12 (67%) were cross-sectional, four (22%) were cohort, and one was descriptive and another retrospective. The women originated from 11 States (i.e., Abuja, Borno, Gombe, Kaduna, Kogi, Lagos, Nasarawa, Ondo, Oyo, Plateau, and Rivers). Based on the classification of geopolitical zones in Nigeria, the South-West (i.e., Lagos, Ondo and Oyo) had the highest number of women included in this study (5627) while South-South (Rivers) had the least (80).
Summary of included studies.

– Not reported.
No study was deemed as having a high risk of bias and so a sensitivity test was not required. Twelve (67%) studies were graded as low risk of bias (score of ≥7 out of 9 on the quality scale) and six (33%) studies were graded as moderate risk of bias (score 4–6 on the quality scale). A visual inspection of a funnel plot showing the relationship between a study's effect size and its precision indicated a symmetrical distribution of studies and confirmed the absence of publication bias in the included studies (Figure 2).

Funnel plot showing symmetrical scatter of studies with no evidence of major publication bias.
HPV Analysis
Testing samples for HPV were obtained via vaginal swabs or cervical smear. The HPV genotyping of the Nigerian patients was conducted in laboratories in the North-Central, North-East, North-West, and South-West of the country. HPV detection and genotyping were performed either with commercially available DNA tests, such as Roche Linear Array HPV Genotyping test and Digene Hybrid Capture II DNA test, or through an assay of PCR using specific primers such as MY09/MY11 or GP5+/GP6+. A range of 16–68 hrHPV genotypes was identified.
In total, from the 18 studies, 4342 women were hrHPV+ve and the prevalence was 25% (95% CI; 0.19, 0.32] (Figure 3). From the 13 studies that assessed HPV16 status, 2071 women were hrHPV16+ve and the prevalence was 9% (95% CI; −0.07, 0.26] (Figure 4). From the 12 studies that assessed HPV18 status, 2012 women were hrHPV18+ve and the prevalence was 10% (95% CI; −0.08, 0.27] (Figure 5). From the two studies that assessed HPV16 and 18 co-infection status, 78 women were hrHPV16+ve and 18+ve and the prevalence was 6% (95% CI; −0.28, 0.40] (Figure 6). From the 11 studies that assessed HPV31 status, 2012 women were hrHPV31+ve and the prevalence was 4% (95% CI; −0.08, 0.16] (Figure 7). From the 11 studies that assessed HPV35 status, 2093 women were hrHPV35+ve and the prevalence was 7% (95% CI; −0.09, 0.23] (Figure 8).
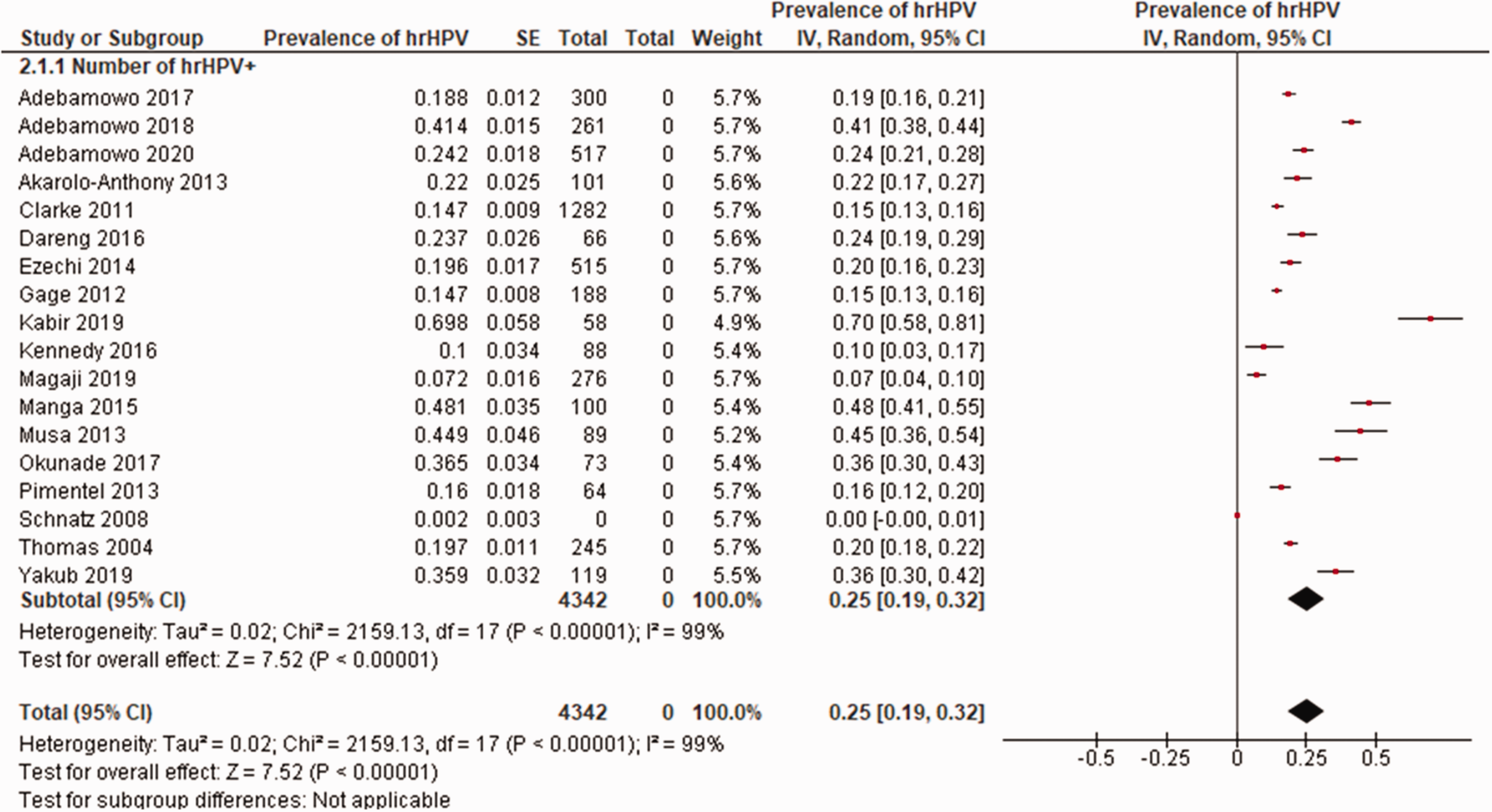
Prevalence of hrHPV.

Prevalence of hrHPV16.

Prevalence of hrHPV18.

Prevalence of HPV16 and 18 co-infections.

Prevalence of hrHPV31.

Prevalence of hrHPV35.
Analysis of data on HPV39, 45, 51, 52, 56, 58, 66, and 68, are shown in Figure 9. Of all these HPV types, hrHPV58+ve had the highest prevalence at 7% (95% CI; −0.23, 0.36) and the data were from three studies involving 389 women.

Prevalence of hrHPV39, 45, 51, 52, 56, 58, 66 and 68.
Sub-group Analysis
From the four studies included in a sub-group analysis that assessed hrHPV status among Nigerian women living with HIV, 1069 women were both hrHPV+ve and HIV+ve and the prevalence was 71% (95% CI; 0.69, 0.73] (Figure 10).

Prevalence of hrHPV among HIV-positive participants.
In a second sub-group analysis that explored prevalence of hrHPV+ve by region, data for the estimated prevalence in the Northern Nigeria were taken from 11 studies (Figure 11). This region had the highest prevalence (32% [95% CI; 0.19, 0.44) compared with southern and western regions. There were no data from the Eastern region.

Prevalence of hrHPV by region.
Risk factors
Multiple sexual partners (≥2) and age at coitarche (≤16 years) were the most frequently reported factors associated with hrHPV infection (Figures 12 and 13). Other significant risk factors included: hormonal contraceptive use; smoking exposure; age at menarche (≤16 years); age (≤30 years); age at first pregnancy (≤16 years).

Prevalence of hrHPV infection risk factors.
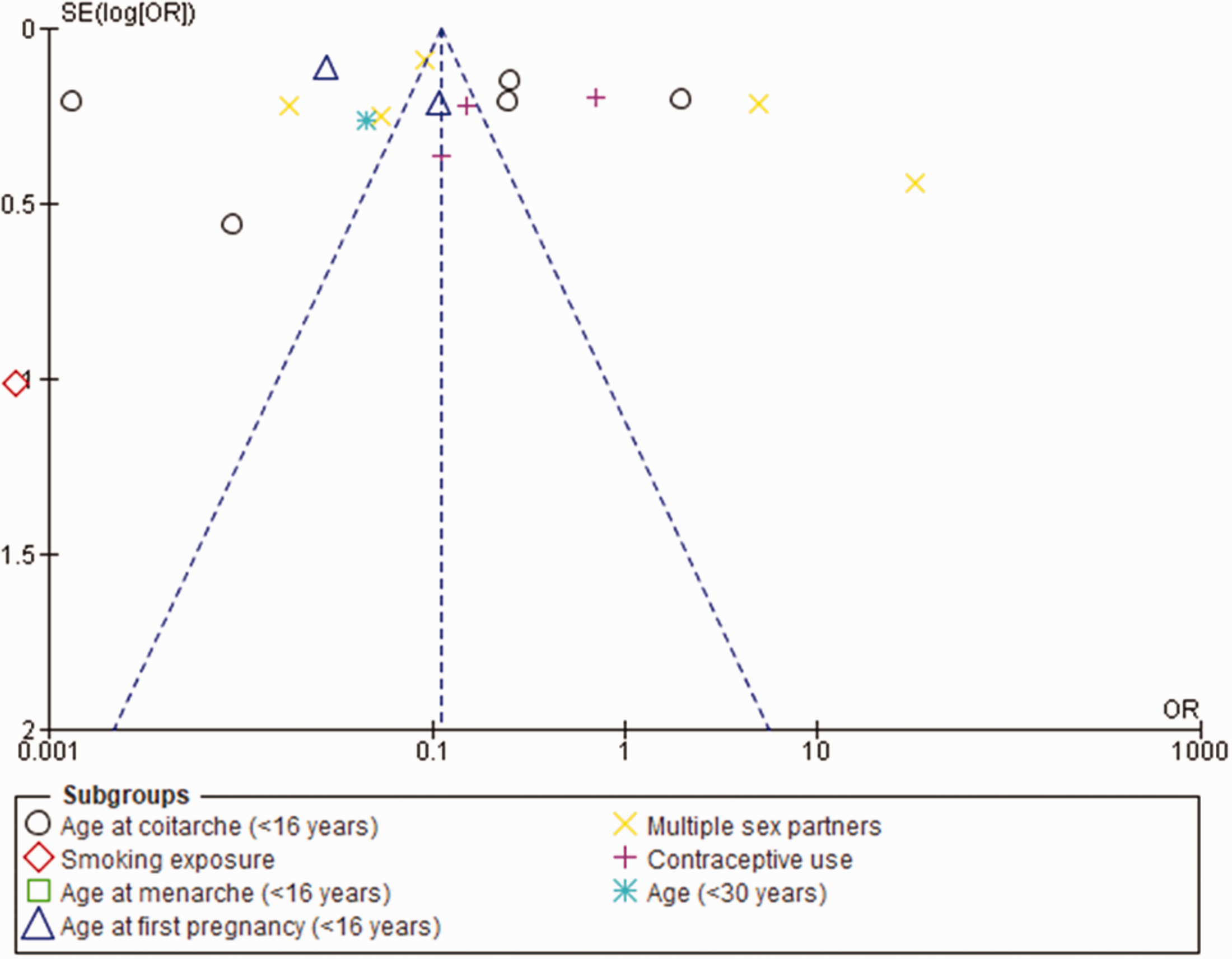
Funnel plot comparing risk factors for hrHPV infection.
Discussion
Despite proven interventions to control cervical cancer through primary, secondary, and tertiary prevention, a global disparity in the burden of cervical cancer persists. 32 From epidemiological, clinical, and molecular studies, infection with hrHPV has been shown to be the most important aetiologic agent in the pathogenesis of cervical cancer. 29 Therefore, the aim of our systematic review and meta-analysis was to determine the prevalence of hrHPV infection and its associated risk factors among women in Nigeria from the ages of 25 to 65 years.
We identified 18 studies that met our eligibility criteria. Twelve (67%) studies were graded as low risk of bias (score of ≥7 out of 9 on the quality scale) and six (33%) studies were graded as moderate risk of bias (score 4–6 on the quality scale). From the studies, we found that the estimated pooled prevalence of hrHPV genotypes among Nigerian women (25%) was lower compared with previous reports from primary studies conducted in the South-West (45%), 33 North-East (70%), 31 and North-West (76%) 34 regions of Nigeria. However, the prevalence was higher compared with a study conducted in the North-Central region (16%). 20 The variability in the burden of hrHPV across the country might reflect differences in cultural practices. For example, the early marriage age of females in northern Nigeria, associated with early sexual debut.24,34 Other plausible reasons for the disparity in the prevalence of hrHPV may be related to influences of geographical dissimilarities, differences in methods of DNA extraction, and diagnostic performance of HPV detection protocols. 31 Interestingly, our findings are higher than hrHPV genotypes recorded in Uganda (21%) and Zimbabwean (17%) women.35,36 Although the results were pooled from only two studies, our findings for the overall prevalence of hrHPV16 and 18 co-infection (6%) were consistent with estimates from a large population-based study conducted in China (2%). 37
We found the prevalence of hrHPV infection HIV+ve women was 71%. This result is consistent with findings from a meta-analysis of data from 19 studies in LMICs that reported a 51% overall pooled prevalence. 38 but higher than the 27% recorded from a previous single centre study conducted in Kenya. 39 The pooled prevalence of several high-risk HPV genotypes was also estimated in this study (i.e., HPV genotypes 16, 18, 31, 35, 39, 45, 51, 52, 56, 58, 66, and 68). The highest prevalence was observed for HPV18 (10%), 16 (7%), 35 (7%) and 58 (7%). These results align with findings from a review of data from Ethiopian women which found HPV16, 18, 58, and 45 were the top four genotypes, with prevalence of 45%, 8%, 7%, and 5%, respectively. 40 HPV16 is considered the most prominent HPV type in the development of cervical cancer and other HPV-associated malignancies. 41 HPV35 is also an oncogenic HPV type, and is closely related phylogenetically to HPV16. 41 However, data from our review showed that HPV18 was the most prevalent HPV type in our sample of 10,375 women.
We found that multiple sexual partners (≥2) and age at coitarche (≤16 years) were risk factors most frequently associated with hrHPV infection. Other risk factors that were significant included, age at first pregnancy (≤16 years), smoking exposure, contraceptive use, and age (≤30 years). Although slightly different risk factors, our findings are consistent with those from another review undertaken in Nigerian women. 41 These authors found duration (years) of sexual exposure, history of other malignancies, history of sexually transmitted infections, coital frequency/week, circumcision status of the sexual partner, and marital status, were significant risk factors of hrHPV infection. 40
Our study had several limitations. For example, most of our included studies were cross-sectional, making it challenging to establish a cause-effect relationship due to the nature of the study design. In addition, our studies were limited to five regions of Nigeria (i.e., North Central, North East, North West, South West and South South), which may have influenced the generalizability of our findings. Furthermore, although we confirmed absence of publication bias, six studies were graded as ‘moderate risk of bias’ on the quality scale. Therefore, caution should be exercised in interpreting our findings. Finally, we excluded several factors such as educational status, CD4 count, and co-infections as risk factors for hrHPV infection.
Despite the high burden of cervical cancer in Nigeria, there has been limited research on the prevalence and distribution of HPV genotypes among Nigerian women. This study contributes to the understanding hrHPV infection among Nigerian women and its impact on cervical cancer. The findings emphasize the need for early detection, treatment, and prevention of hrHPV infection and associated precancerous lesions. HIV positive women should be identified as a high-risk group. Specific risk factors were identified, which will inform prevention programs. In addition, the study identified the most prevalent hrHPV genotypes in the Nigerian population, which could inform future screening and vaccination strategies. The findings of this review provide evidence to support improvements in policies and practices aimed at reducing the prevalence of hrHPV among Nigerian women. To enhance the well-being of Nigerian women and prevent cervical cancer, it is necessary to strengthen programs for diagnosis and treatment and provide HPV vaccination based on common hrHPV genotypes.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231182884 - Supplemental material for High-risk human papillomavirus infection among Nigerian women: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-imr-10.1177_03000605231182884 for High-risk human papillomavirus infection among Nigerian women: A systematic review and meta-analysis by Oliver Ezechi, Folahanmi Akinsolu, Abideen Salako, Olunike Abodunrin, Ifeoluwa Adewole, Mobolaji Olagunju, Hilary Okunbor, Rukayat Sanni-Adeniyi, Emmanuella Zamba, Diana Wangeshi Njuguna and George Eleje in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605231182884 - Supplemental material for High-risk human papillomavirus infection among Nigerian women: A systematic review and meta-analysis
Supplemental material, sj-pdf-2-imr-10.1177_03000605231182884 for High-risk human papillomavirus infection among Nigerian women: A systematic review and meta-analysis by Oliver Ezechi, Folahanmi Akinsolu, Abideen Salako, Olunike Abodunrin, Ifeoluwa Adewole, Mobolaji Olagunju, Hilary Okunbor, Rukayat Sanni-Adeniyi, Emmanuella Zamba, Diana Wangeshi Njuguna and George Eleje in Journal of International Medical Research
Supplemental Material
sj-pdf-3-imr-10.1177_03000605231182884 - Supplemental material for High-risk human papillomavirus infection among Nigerian women: A systematic review and meta-analysis
Supplemental material, sj-pdf-3-imr-10.1177_03000605231182884 for High-risk human papillomavirus infection among Nigerian women: A systematic review and meta-analysis by Oliver Ezechi, Folahanmi Akinsolu, Abideen Salako, Olunike Abodunrin, Ifeoluwa Adewole, Mobolaji Olagunju, Hilary Okunbor, Rukayat Sanni-Adeniyi, Emmanuella Zamba, Diana Wangeshi Njuguna and George Eleje in Journal of International Medical Research
Footnotes
Acknowledgment
We would like to express our sincere gratitude to the Clinical Science Department, Nigerian Institute of Medical Research, Yaba, Lagos, and the Department of Public Health, Faculty of Basic Medical and Health Sciences, Lead City University, Ibadan, for their invaluable support and guidance throughout this systematic review. Their expertise and resources were essential in the successful completion of this study. We also appreciate all the authors whose studies were included in this review.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.