
Abstract
Objective
To investigate the prevalence of Sjögren’s syndrome (SS) and the associated factors in a sample of the Egyptian population.
Methods
This cross-sectional study obtained data by screening subjects from several hospitals in different governorates across Egypt. Demographic and health data were collected including symptoms and type of Sjögren’s syndrome, associated autoimmune diseases, the presence of specific autoantibodies and associated malignancies.
Results
The study analysed 7960 participants and 64 (0.80%) had SS. Of these, 22 (34.38%) had primary SS and 42 patients (65.63%) had secondary SS. For the total study cohort, the prevalence of primary and secondary SS was 0.28% and 0.53%, respectively. There was a higher prevalence of SS in females compared with males and SS was more common in the fifth and sixth decades. All patients with SS complained of oral and ocular dryness. The most common concomitant autoimmune disease was rheumatoid arthritis. Anti-SSA (Ro) and anti-SSB (La) antibodies were the most frequently associated autoantibodies. Only two patients had non-Hodgkin’s lymphoma.
Conclusion
This was the first study to describe the prevalence of SS in Egypt. SS is not a rare disease in Egypt, so raising awareness of SS in both patients and healthcare professionals is very important.
Introduction
Sjögren’s syndrome (SS) is a chronic slowly progressive systemic autoimmune disease that primarily affects the function of exocrine glands such as the salivary and lacrimal glands, leading to dry eye and dry mouth symptoms. Moreover, it can also cause several extraglandular symptoms such as musculoskeletal problems, fatigue, and skin lesions in addition to varying degrees of renal, neurological, hepatic and pulmonary involvement.1,2 SS is caused by lymphocyte accumulation producing autoantibodies targeting the salivary and lacrimal glands. 2 There are two subtypes of SS: primary SS (pSS), which affects previously healthy individuals; and secondary SS (sSS), which occurs in patients in combination with other autoimmune disorders such as rheumatoid arthritis, systemic lupus erythematosus and systemic sclerosis. 1
Previous epidemiological studies evaluating the prevalence of SS have yielded widely variable results, ranging between 0.01% and 3% of populations, which has created debate regarding the possible consideration of pSS as a rare disease. 3 These variations in the prevalence rates could reflect a real inconsistency between different populations or they could be due to different study designs and methods of diagnosis. Thus, an accurate assessment of the prevalence of pSS is particularly important to clarify the variable rates between populations with different genetic backgrounds and to determine the disease burden. 3 Although the overall mortality rate of patients with pSS is similar to that of the general population, it increases in older patients with parotid swelling, and it may also be associated with hypocomplementaemia, infections, cryoglobulinaemia, cardiovascular diseases and certain malignancies such as Hodgkin's lymphoma, which is the main malignancy associated with SS as a result of excess B cell activity. 4 Nonetheless, the global incidence of SS may have been underestimated because some patients are asymptomatic or have mild symptoms and they may never get diagnosed. SS has a significant impact on the perceived health and the quality of life of the patients; it also leads to a greater use of medical services by the patients. 3
Epidemiological information on SS is limited in African countries, which are very underrepresented in universal epidemiological research.3,5 Current studies from Europe and America have emphasized that both ethnic differences and geographic location influence the phenotypic expression of SS; for example, earlier onset of the disease together with a higher risk of developing lymphoma is more frequently encountered in Africans in comparison with White people.6–8
There is a considerable need to undertake studies in African countries to obtain more accurate prevalence data for this important disease that affects the quality of life of many patients. Accordingly, the present study was performed to investigate the epidemiology of Sjögren’s syndrome and the associated factors in a sample of the Egyptian population.
Patients and methods
Study design
This cross-sectional study analysed data obtained by screening subjects from several hospitals and dental convoys in various locations withing Egypt between August 2023 and April 2024. All individuals in the population-based sample were invited to take part in the present study in a consecutive way to avoid selection bias. They were informed about the study's nature and those who agreed to participate gave their consent as the first question of the survey questionnaire. The inclusion criteria were as follows: (i) Egyptian males and females > 18 years old; (ii) residents of any Egyptian governorate; (iii) only patients diagnosed with SS according to the American–European Consensus Group (AECG) classification criteria. 9 The exclusion criteria were as follows: (i) non-Egyptians; (ii) patients who refused to participate in the study; (iii) patients with a history of head and neck radiotherapy: (iv) patients receiving drugs that reduced salivary flow such as antihistaminic medications or diuretics.
This study was approved by the institutional research ethics committee of the British University in Egypt (approval no. 23-054; September 2023) and was performed according to the Declaration of Helsinki of 1975 as revised in 2013 and reported according to the relevant EQUATOR network guidelines. All patient details were de-identified. Patients providing data for the study were required to provide verbal informed consent. The reporting of this study conforms to STROBE guidelines. 10
Data collection
Demographic and health data were collected during a structured interview to identify patients with sicca symptoms, those who were diagnosed with SS and those who were not. Sicca symptoms were explored by evaluation of ocular symptoms and evaluation of oral symptoms. Each one consisted of three questions and if any of these three questions were answered as ‘yes’, the participant was determined as having ocular or oral symptoms. These questions are those used in the European criteria proposed by the AECG in 2002 to detect sicca symptoms because it is the most widely used classification criteria. 9 The individuals with a diagnosis of SS were classified according to the type of SS as either pSS or sSS. Patients with sSS were further categorized according to the associated autoimmune disease as rheumatoid arthritis, systemic lupus erythematosus, mixed connective tissue disease, systemic sclerosis or any other autoimmune diseases.
The presence of any comorbidities such as hypertension, cardiovascular disease, renal disease, serious infections or any other condition was recorded. The presence of specific autoantibodies such as anti-SSA (Ro), anti-SSB (La), antinuclear antibodies (ANA), rheumatoid factor (RF) and anti-salivary gland protein (SP1) was also recorded. The occurrence of lymphoma or any other malignancy in association with SS was acknowledged and recorded. Regarding quantitative variables as age and duration of SS, SS patients were distributed into three age categories: 40–49 years, 50–59 years and 60–70 years. The duration of SS was expressed either a duration of ≤1 year or >1 year.
Statistical analyses
A sample size calculation was based on research published regarding the incidence of SS in Spain. 11 By fixing alpha at 0.05 and beta at 0.2, the odd ratio was 5.4. The minimal sample size was 7580 subjects to be included.
All statistical analyses were performed using the R statistical package (R version 4.4.1; R Foundation for Statistical Computing, Vienna, Austria). The data are presented as frequency and percentage values. Univariate associations between SS type (primary versus secondary) and different predictors were analysed using χ2-test. A decision tree analysis using the Chi-square Automatic Interaction Detection algorithm was made to detect any significant subgroups within the dataset. Additionally, univariate and multivariate binary logistic regression models were constructed to examine the effect of adjusted and unadjusted predictor variables on the type of SS. The unadjusted model estimated the impact of each variable on the outcome without controlling for other factors, while the multivariate model adjusted for potential confounders to isolate the independent effect of each predictor. A P-value <0.05 was considered statistically significant.
Results
This cross-sectional study enrolled 7960 participants; of which 3124 (39.25%) were male and 4836 (60.75%) were female. Regarding age distribution, 1518 participants (19.07%) were aged 20–40 years, 3680 participants (46.23%) were aged 41–59 years and 2762 participants (34.70%) were aged 60–70 years. The majority of study participants (7896 of 7960; 99.20%) did not have SS; while 64 participants (0.80%) were reported as having SS.
The demographic and clinical data for the SS patients (n = 64) are presented in Table 1. Regarding sex distribution, 11 participants (17.19%) were males and 53 (82.81%) were females. The age distribution was as follows: 12 participants (18.75%) were between 40–49 years, 33 (51.56%) were between 50–59 years and 19 (29.69%) were between 60–70 years. Clinical features showed that 45 participants (70.31%) experienced a burning sensation, while 19 (29.69%) did not. In terms of SS types, 22 participants (34.38%) had pSS and 42 (65.63%) had sSS. The prevalence of pSS and sSS was estimated at 0.28% and 0.53%, respectively.
Demographic and clinical characteristics of the patients (n = 64) diagnosed with Sjogren’s syndrome (SS) in a cross-sectional study that investigated the epidemiology of SS and the associated factors in a sample of the Egyptian population.
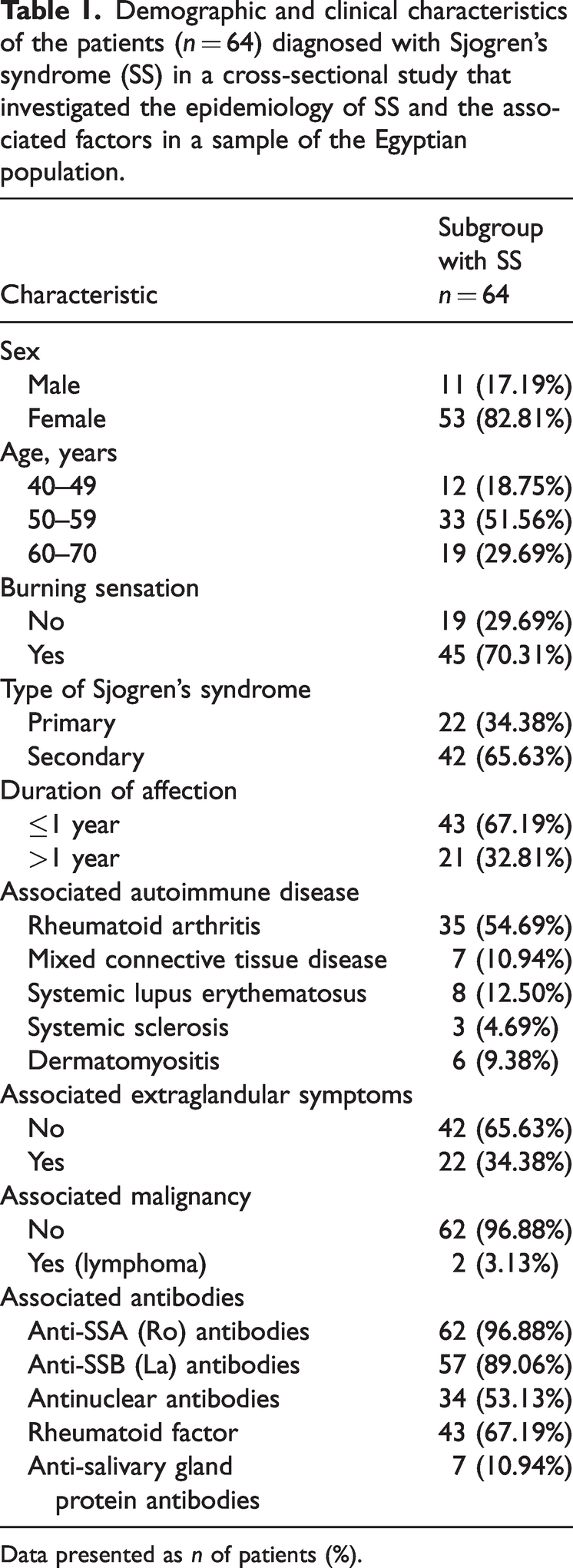
Data presented as n of patients (%).
Duration of affection demonstrated that 43 participants (67.19%) had been affected for ≤1 year , whereas 21 (32.81%) had a longer duration of affection. Associated autoimmune diseases were reported as follows: rheumatoid arthritis in 35 participants (54.69%), mixed connective tissue disease in seven (10.94%), systemic lupus erythematosus in eight (12.50%), systemic sclerosis in three (4.69%) and dermatomyositis in six (9.38%).
Regarding extraglandular symptoms, 42 participants (65.63%) did not report any, while 22 (34.38%) did. Associated malignancies were rare, with only two participants (3.13%) reporting lymphoma. Antibody presence was high, with 62 participants (96.88%) testing positive for anti-SSA (Ro) antibodies, 57 (89.06%) for anti-SSB (La) antibodies, 34 (53.13%) for ANA, 43 (67.19%) for RF and seven (10.94%) for SP1 antibodies.
The patients were stratified into pSS and sSS based on the type of SS (Table 2). A significantly larger proportion of patients with sSS had joint and muscle pain compared with the pSS group (P = 0.025). A significantly higher proportion of patients with sSS had ANA antibodies compared with the pSS group (P < 0.001). There were no other significant between-group differences.
Demographic and clinical characteristics of the patients (n = 64) diagnosed with Sjogren’s syndrome (SS) stratified according to the type of SS in a cross-sectional study that investigated the epidemiology of SS.

Data presented as n of patients (%).
Univariate associations between SS type (primary versus secondary) and different predictors were analysed using χ2-test; NS, no significant between-group difference (P ≥ 0.05).
There was no association between the presence of autoimmune disease and specific autoantibodies in patients (n = 64) diagnosed with SS (Table 3). A multivariate model with all the tested predictors included was conducted to analyse their effect on the type of SS (Table 4). The model was statistically significant (χ2 (11) = 58.847; P < 0.001) and explained 83.1% of the variability in the outcome (Nagelkerke's R2). The results showed that the odds of the presence of RF in the cases of sSS was higher than that of anti-SSA (Ro) antibodies. Additionally, the odds of the presence of anti-SSA (Ro) antibodies in the cases of sSS was higher than that of the SP1 antibodies. The results of the unadjusted models generally agreed with their adjusted counterparts, except for extraglandular affection. This might have been due to a significant association between this predictor and RF (P < 0.001).
Association between the presence of autoimmune disease and autoantibodies in patients (n = 64) diagnosed with Sjogren’s syndrome (SS) in a cross-sectional study that investigated the epidemiology of SS.

Data presented as n of patients (%).
A multivariate model with all of the tested predictors of the type of Sjogren’s syndrome (SS) in patients (n = 64) included in a cross-sectional study that investigated the epidemiology of SS.

*P < 0.05.
CI, confidence interval.
Discussion
Sjögren’s syndrome is the second most common autoimmune disorder after rheumatoid arthritis, with a variable global prevalence ranging from 0.01% and 3%. 3 The results of prevalence studies of SS are heterogeneous because of the different diagnostic criteria used in each study and the diverse geographical areas and ethnic populations in which they were performed.12,13 The epidemiology of SS is poorly characterized in Africa with limited available data suggesting the need for more focused high-quality research in different countries. 14 Epidemiological studies are essential to identify the actual prevalence rates of this disease in different populations to recognize its burden on society and clarify any associated factors or conditions. Nevertheless, data originating from African countries are scarce, thus, the present investigation aimed to investigate the prevalence of SS in a sample of the Egyptian population for the first time.
The present cross-sectional study screened a total of 7960 subjects from several hospitals and dental convoys in different locations across Egypt, which were scattered throughout seven governorates: Cairo, Alexandria, Behera, Dakahlia, Gharbia, Menoufia and Qalyubia. This sampling pattern was to avoid information bias and increase the variability and validity of the study sample. Diagnosis of SS was undertaken according to the AECG classification criteria as it is the most widely used classification criteria. 11 The authors have focused on previous research articles that have used the same criteria when discussing the present results. The current study demonstrated that 64 of 7960 study participants were diagnosed with SS, which was a prevalence of 0.80%. This prevalence rate falls within the range of the worldwide prevalence of SS that is estimated to range from 0.01%–3%.3,15–17 The current prevalence rate for SS of 0.80% is also close to those reported in Turkey (0.72%) and Denmark (1%).18,19 It is a little higher than the estimated prevalence of 0.4% in the UK and that reported in Spain (0.33%).10,20
The prevalence of pSS had never been evaluated in Egypt. In the present cross-sectional population study, the prevalence of pSS was 0.28%, which agrees well with the 0.25% prevalence of pSS reported in Spain; 10 and it is also similar to that reported in Greece (0.15–0.23%) and Turkey (0.21%).15,21,22 These data suggest that the prevalence of pSS in the Mediterranean countries including Egypt ranges between 0.15% and 0.28%. On the other hand, some studies have reported lower pSS prevalence rates of 0.06%, 0.02% and 0.03%.7,23,24
Based on the above-mentioned data, pSS should not be considered a rare disease anymore in most European and Mediterranean countries and the current results suggest that this also applies to Egypt. This indicates the need to raise awareness regarding SS symptoms, diagnosis and management, in addition to focusing on the development of effective therapeutic strategies by researchers and healthcare providers to reduce the disease burden.
All SS patients in the present investigation complained of oral and ocular dryness, which was consistent with the documented evidence that ocular and oral dryness are the hallmark symptoms of SS. 25 Regarding age range in the current study, only 12 patients (18.75%) were between 40–49 years, while 33 (51.56%) were between 50–59 years and 19 (29.69%) were between 60–70 years, reflecting a higher prevalence of SS in the fifth and sixth decades of life, which is in line with several previous studies.10,13,14,26
Among SS patients, 82.81% were females and 17.19% were males; an approximate female-to-male ratio of 5:1. These results agree well with recent research showing that women accounted for 86% of patients with SS; 24 and with a recent study in Spain where women represented 85% of SS patients. 10 Also, the current results are in line with previous studies reporting more frequent disease occurrence in women but with slightly lower female-to-male ratios.4,14 Similarly, SS was reported to affect middle-aged females, with a mean age of onset in the fourth or fifth decade. 13
Among the affected 64 patients with SS in the current study, 22 (34.38%) had pSS and 42 patients (65.63%) had sSS. The most common associated autoimmune disease was rheumatoid arthritis, which affected 54.69% of SS patients in the current study; followed by systemic lupus erythematosus (12.50%), then dermatomyositis (9.38%) and the least common was systemic sclerosis (4.69%). The proportions of patients with autoantibodies were similar for the associated autoimmune diseases, with the highest proportions occurring in patients with rheumatoid arthritis. These results agree with a few studies reporting the common association of SS with several autoimmune diseases, especially rheumatoid arthritis and systemic lupus erythematosus.12,13,27,28
Anti-SSA (Ro) antibodies were most frequently associated with SS as they were encountered in 96.88% of patients followed by anti-SSB (La) antibodies, which were present in 89.06% of patients. The least frequently encountered antibodies were SP1 antibodies, which were only seen in 10.94% of patients. In addition, a significantly higher proportion of sSS patients had ANA antibodies compared with the pSS group (P < 0.001). These current results agree with recent research demonstrating that ANA antibodies are the most frequent autoantibodies detected in SS, with anti-Ro/SS-A antibodies being the most specific antibodies.13,14,29,30
Two patients in the present study had the associated malignancy non-Hodgkin’s lymphoma: one pSS patient and one sSS patient having associated rheumatoid arthritis. The increased risk of lymphoma in SS patients is well documented; pSS has been linked with an increased risk of non-Hodgkin’s lymphoma with a 5% lifetime risk. 31 While a lower lymphoma prevalence in pSS of 2.6% was reported in a recent cross-sectional study on pSS patients. 32 Moreover, other studies have shown that having both SS and rheumatoid arthritis increased the risk of non-Hodgkin's lymphoma and increased the mortality rate compared with those patients with rheumatoid arthritis alone.10,33 Since the prevalence of non-Hodgkin’s lymphoma (2.7– 9.8%) is becoming more common in SS patients, constant monitoring of patients over time is extremely important.34,35
Previous studies indicated that the coexistence of rheumatoid arthritis and SS could result in more severe arthritis with worse joint pain than that normally expected in rheumatoid arthritis alone.29,36 This could explain the significantly higher proportion of patients with sSS who reported joint and muscle pain compared with the pSS group in the current study. Extraglandular symptoms were much more common in the current study among sSS patients compared with the pSS group, which is in accordance with other related research reporting that extraglandular manifestations including myalgias and arthralgias are more frequently seen in sSS patients, leading to poor quality of life. 37
This current study had several limitations. First, focusing on hospitals and dental convoys for screening SS cases might be considered a limitation, but these are ideal places to encounter cases with minimal health mindfulness due to the general lack of awareness of this disease in the Egyptian population. There is an obvious deficiency in epidemiological studies in Africa and Egypt, 38 which might be attributed to the difficulties facing researchers in accessing accurate data from official registries, in addition to the potentially large number of unregistered patients presenting to private clinics because these are an important part of the healthcare system in addition to hospital-based systems in Egypt. These limiting factors are hindering disease prevalence studies including the prevalence of SS, which has never been previously evaluated in Egypt. In addition, the nonspecific symptoms associated with SS, especially in early stages of the disease, cause many cases of SS to go undiagnosed and overlooked for several years. Also, the lack of rheumatologists or specialists in general, especially in rural areas, makes it difficult to accurately estimate the incidence and prevalence of certain diseases, 38 thus the actual prevalence rate could be much higher. Another limitation is that data on the evaluated variables were not always available, so patients with incomplete records were excluded from the study. The current cross-sectional study estimated the prevalence of SS in Egypt for the first time by screening a large number of patients in different governorates scattered throughout Egypt, which is a point of strength of the current investigation.
In conclusion, the current cross-sectional study was performed to assess the prevalence of SS in Egypt, which was found to be 0.8%: and the prevalence of pSS and sSS was estimated as 0.28% and 0.53%, respectively. A higher prevalence of SS was encountered in females in the fifth and sixth decades. The most common autoimmune disease was rheumatoid arthritis. Anti-SSA (Ro) antibodies were the most frequent followed by anti-SSB (La) antibodies. Only two patients had non-Hodgkin’s lymphoma. These current findings suggest that SS is not a rare disease in Egypt, so raising awareness in both patients and healthcare professionals regarding symptoms, diagnosis and management of SS is important.
Footnotes
Author contribution
D.G.: conceptualization; supervision and editing; writing review, results, discussion & conclusion. A.Ab.: resources, data collection, and writing the original draft. A.Am.: clinical examination and data collection and writing the original draft. A.H.: clinical examination, data collection and writing the original draft. A.Eg.: clinical examination, data collection and writing the original draft. R.G.: data collection and writing the original draft. M.G.: writing a review and analysing the results.
Data availability statement
All data are available and included in the article.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.