
Abstract
Objective
We herein propose a novel approach, laparoscopic segmental colectomy with extensive D3 lymph node dissection (ED3LND), for right-sided transverse colon cancer (TCC).
Methods
Forty-two patients with right-sided TCC were randomly assigned to two groups: Group 1 (segmental colectomy with D3LND) and Group 2 (segmental colectomy with ED3LND). Clinical characteristics, surgical and pathological outcomes, and oncological outcomes were retrospectively compared between the two groups.
Results
The number of lymph nodes retrieved, apical lymph nodes retrieved, and apical lymph node metastases were significantly lower in Group 1 than in Group 2. No significant differences were observed in the operation time, length of hospital stay, estimated blood loss, lymph node metastases, postoperative lymphoceles, or other Clavien–Dindo grade ≥III postoperative complications between the two groups. The 3-year disease-free survival rate was 82.6% in Group 1 and 84.2% in Group 2, with no significant difference.
Conclusions
Laparoscopic segmental colectomy with ED3LND for right-sided TCC may offer better oncological outcomes than D3LND. A large-scale prospective randomized controlled study is needed to further validate the oncological benefits of this novel procedure.
Keywords
Introduction
Transverse colon cancer (TCC) refers to tumors located between the hepatic and splenic flexures of the colon. The complexity of the anatomy and the lack of extensive randomized controlled trials make it challenging to standardize surgical procedures for TCC. The proximity of the transverse colon to critical upper abdominal structures adds further difficulty in performing radical surgery for TCC. Currently, there are no definitive guidelines for TCC surgeries, and surgical approaches often depend on the surgeon’s preference in clinical practice. The two primary surgical methods commonly used are segmental colectomy and right hemicolectomy with D3 lymph node dissection (D3LND). When comparing these two methods, right hemicolectomy typically yields a longer specimen and more harvested lymph nodes than does segmental colectomy. However, right hemicolectomy also involves greater trauma and potential functional damage. To combine the benefits of both approaches and consider both oncological and functional outcomes, we propose a novel approach for right-sided TCC: laparoscopic segmental colectomy with extensive D3LND (ED3LND). 1 Our preliminary study has confirmed the feasibility of this procedure, warranting further investigation through comparative studies.
Patients and methods
Data
We conducted a retrospective analysis of patients with right-sided TCC who underwent either laparoscopic segmental colectomy with D3LND or ED3LND by experienced surgeons at Hunan Provincial People’s Hospital between January 2017 and March 2021. Right-sided TCC was defined as a tumor located between the hepatic flexure and the midpoint of the transverse colon. The surgeons, each having performed a minimum of 100 laparoscopic colorectal resections annually, were highly skilled in laparoscopic colorectal surgery. We reviewed the medical records of 49 patients with right-sided TCC (Stage pT1-4aN0-2M0) during this period. The patients were randomly assigned to undergo D3LND or ED3LND in our department, and 42 patients met the inclusion criteria. Among these, 23 patients underwent D3LND and 19 underwent ED3LND.
The inclusion criteria were an age of ≥18 years, treatment by laparoscopic segmental colectomy with D3LND or ED3LND, and an American Society of Anesthesiologists score of ≤III. The exclusion criteria were incomplete data, synchronous colorectal carcinoma, emergency surgery, a primary tumor for which R0 resection was not achieved, and a history of colon or rectal segmental resections. This retrospective study was evaluated and approved by the ethics committee of Hunan Provincial People’s Hospital. The study received their exemption according to the regulations. Written informed consent was obtained from the patients for both treatment and publication. The study was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. We have de-identified all patient details. The reporting of this study conforms to the STROBE guidelines. 2
Group 1 comprised 23 patients who underwent D3LND, and Group 2 comprised 19 patients who underwent ED3LND. The following clinical characteristics were compared between the two groups: age at surgery, sex, body mass index (BMI), American Society of Anesthesiologists score, tumor size, and tumor stage (UICC). Additionally, the following surgical and pathological outcomes were compared: operation time, length of hospital stay, estimated blood loss, lymph node retrieval, apical lymph node retrieval, lymph node metastases, apical lymph node metastases, postoperative lymphoceles, and other Clavien–Dindo grade ≥III postoperative complications). Finally, the disease-free survival (DFS) curves of the two groups were drawn accordingly.
Surgical procedure
In recent years, we have focused on optimizing the surgical technique for patients with TCC. According to the Atlas of Human Anatomy, 3 the lymphatic vessels of the right colon flow to the root of the superior mesenteric blood vessels along the main intestinal blood vessels, and these lymphatic vessels are interconnected at the root of the main vessels (Figure 1(a)). Considering both oncological and functional outcomes compared with traditional D3LND (Figure 1(b), (d)), we propose laparoscopic segmental colectomy with ED3LND for right-sided TCC (Figure 1(c), (e), (f)). 1 The arterial patterns of the right and transverse colon exhibit significant variability, including the presence of supernumerary branches, common trunks, and certain branches.3–6 To address these variations, we compiled numerous vascular ligation locations and surgical resection ranges corresponding to normal arterial patterns (Figure 2). The vascular preservation and ligation followed the approach proposed by Efetov et al. 7 We present a surgical field after ED3LND in a case where the apical lymph nodes (Nos. 203, 213, and 223) were resected, while the accessory right colic artery, right colic vein, ileocolic artery, ileocolic vein, ileocecal junction, and part of the ascending colon were preserved (Figures 3 and 4).

(a) Lymphatic vessels flow to the root of the superior mesenteric blood vessels along the main intestinal vessels, with interconnections at the root of the main vessels (circle). (b) Segmental colectomy with D3 lymph node dissection. (c) Segmental colectomy with extensive D3 lymph node dissection (arrow). (d) D3 lymph node dissection in the specimen and (e, f) extensive D3 lymph node dissection in the specimen (arrow and circle). The green area indicates D3 lymph node dissection. The green and blue areas indicate extensive D3 lymph node dissection. Anatomical images are adapted from Atlas of Human Anatomy 3 .
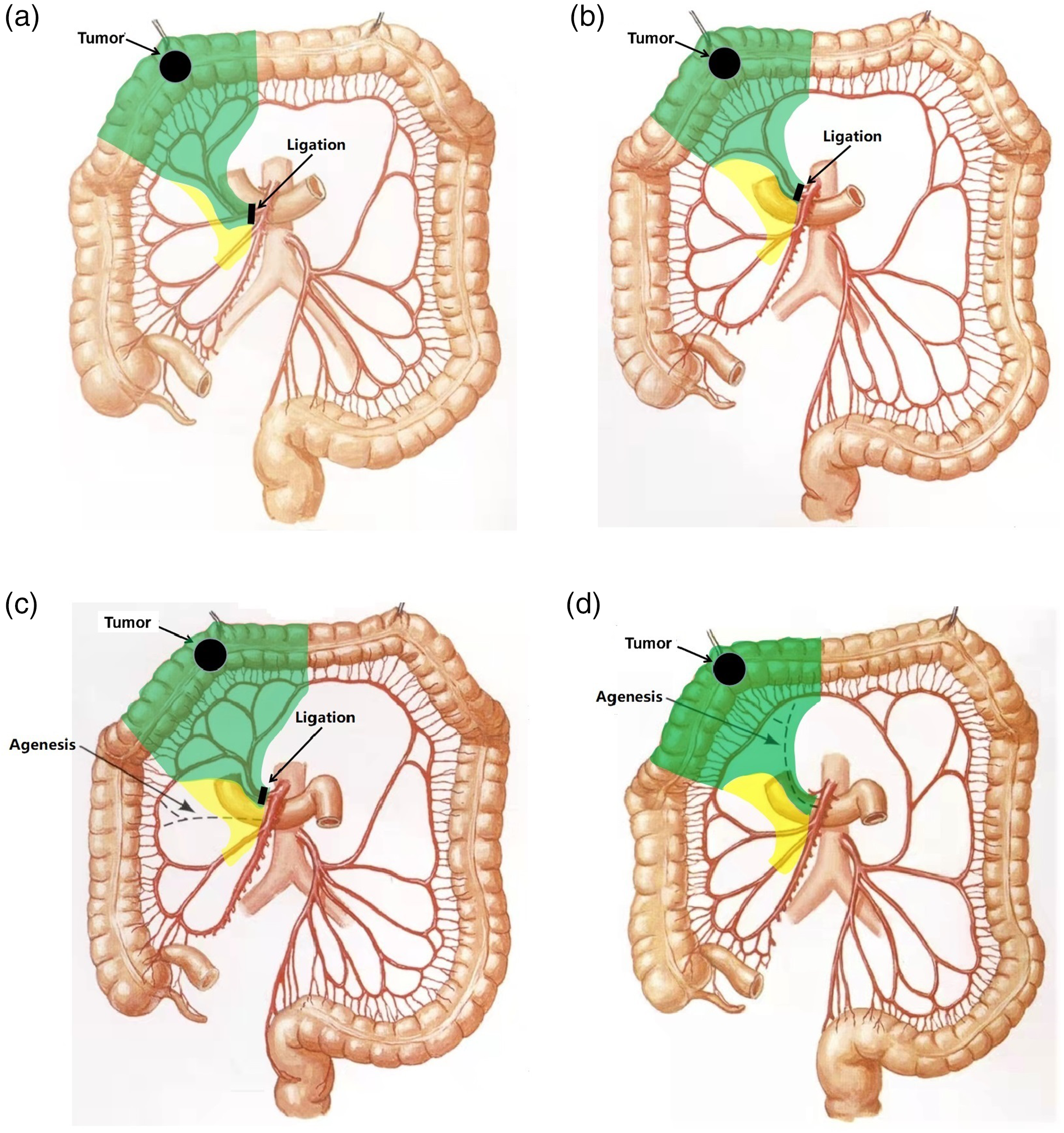
Vascular ligation locations and surgical resection ranges for the novel procedure, corresponding to four common patterns of common trunks: (a) common trunks of the RCA and MCA, (b) common trunks of the RCA and IA, (c) absence of the RCA, and (d) absence of the MCA. Anatomical images are adapted from Atlas of Human Anatomy. 3 The green area indicates D3 lymph node dissection. The green and yellow areas indicate extensive D3 lymph node dissection. RCA, right colic artery; MCA, middle colic artery; IA, ileocolic artery.

Comparison with right hemicolectomy with D3 lymph node dissection. In our procedure, the main vessels of the right-sided colon are preserved. (a) An enlarged apical lymph node surrounds the ileocolic vessels (arrow). Apical lymph node (No. 203) dissection is performed along the ileocolic vessels. (b) Apical lymph node (No. 223) dissection is performed along the middle colic artery (MCA). (c) The right colonic vein (RCV) is preserved, with careful dissection along it and (d) the accessory right colic artery (ARCA) is preserved, with careful dissection along it. IA, ileocolic artery; IV, ileocolic vein; RCV, right colic vein; GTH, gastrocolic trunk of Henle; MCA, middle colic artery; ARCA, accessory right colic artery.

(a, b) Surgical field after ED3LND. Compared with segmental colectomy with D3LND, extensive apical lymph node dissection along the superior mesenteric vessels is performed. Compared with right hemicolectomy with D3LND, the IA, IV, ARCA, and RCV are preserved in the novel ED3LND procedure. (c, d) In this case, the IA, IV, ARCA, RCV, ileocecal junction, and part of the ascending colon are preserved, while apical lymph node dissection is performed. D3LND, D3 lymph node dissection; ED3LND, extended D3 lymph node dissection; ARCA, accessory right colic artery; RCV, right colic vein; AIPDV, anterior inferior pancreaticoduodenal vein; RGV, right gastroepiploic vein; GTH, gastrocolic trunk of Henle; MCA, middle colic artery; RGA, right gastric artery; MCA, middle colic artery; RCA, right colic artery; IA, ileocolic artery; IV, ileocolic vein.
This study adopts the Chinese BMI classification system, which categorizes BMI as underweight (<18.5 kg/m2), normal (18.5–23.9 kg/m2), and overweight/obese (≥24.0 kg/m2). Postoperative adverse events were evaluated using the Clavien–Dindo classification, distinguishing between major (Clavien–Dindo grade III–V) and minor (I–II) events. Postoperative follow-up included serum carcinoembryonic antigen and cancer antigen 19-9 monitoring, abdominal computed tomography, chest X-ray or computed tomography, physical examinations, colonoscopy, and positron emission tomography scanning. None of the 42 patients underwent neoadjuvant therapy. Recurrence was detected through the aforementioned measures or histologic examinations. The most recent follow-up was conducted in March 2023.
Statistical analysis
Continuous variables are presented as mean ±standard deviation. The chi-square test, Fisher’s exact test, and the independent-samples t-test were used for statistical analysis. The Kaplan–Meier method was used to generate survival curves, and the log-rank test was employed to compare survival between the groups. All statistical analyses were performed using SPSS Version 20 (IBM Corp., Armonk, NY, USA). A P-value of <0.05 was considered statistically significant.
Results
Patient characteristics
The baseline characteristics of the patients in the two groups are shown in Table 1. There were no statistically significant differences between them. The surgical and pathological outcomes are shown in Table 2. There was a significant difference in the number of lymph nodes retrieved, apical lymph nodes retrieved, and apical lymph node metastases (P = 0.020, 0.026, and 0.045, respectively) between the two groups. Only two patients in Group 1 developed postoperative lymphoceles, which resolved on postoperative day 9 and 15, respectively. Treatment for the postoperative lymphoceles included fasting, drainage, correction of anemia and hypoproteinemia, and the use of total parenteral nutrition and somatostatin. Five patients had apical lymph node metastases in Group 2, and their surgical and pathological outcomes are detailed in Table 3.
Patients’ baseline characteristics.
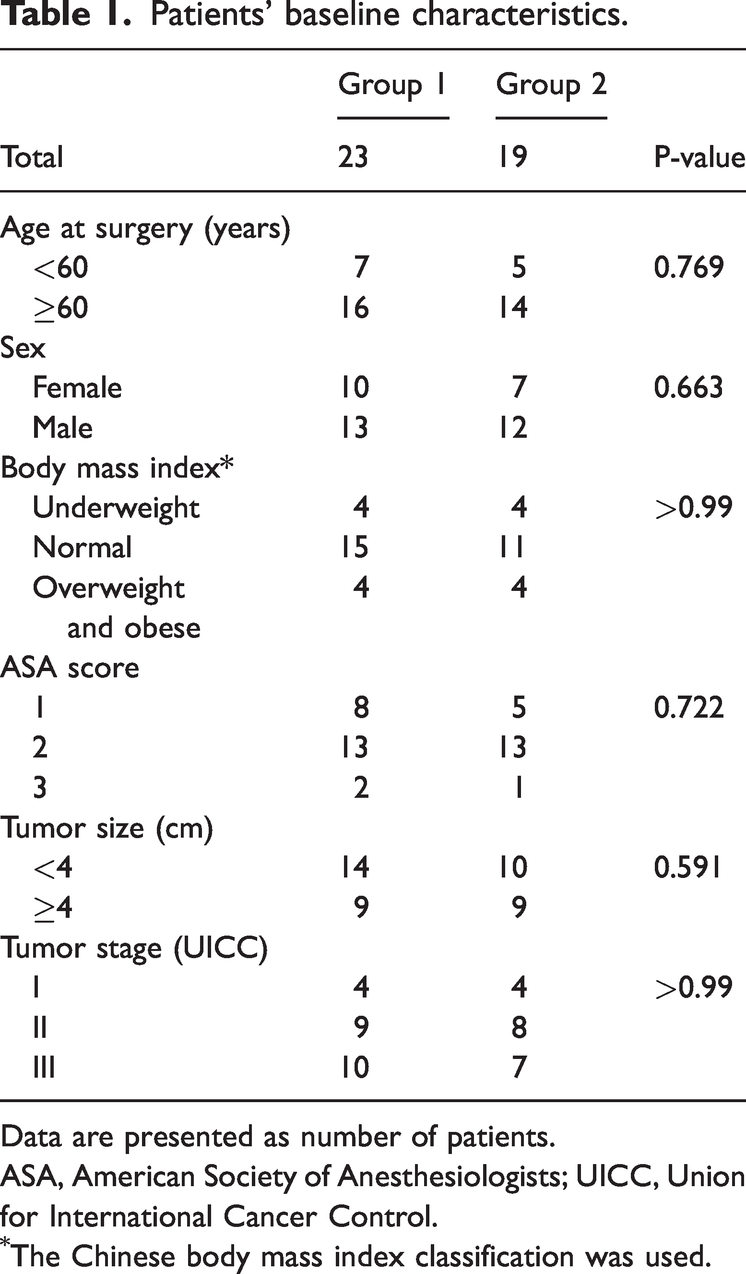
Data are presented as number of patients.
ASA, American Society of Anesthesiologists; UICC, Union for International Cancer Control.
The Chinese body mass index classification was used.
Patients’ surgical and pathological outcomes.

Data are presented as mean ± standard deviation or number of patients.
Surgical complications were analyzed using the Clavien–Dindo classification.
Surgical and pathological outcomes of the five patients with apical LNM in Group 2.
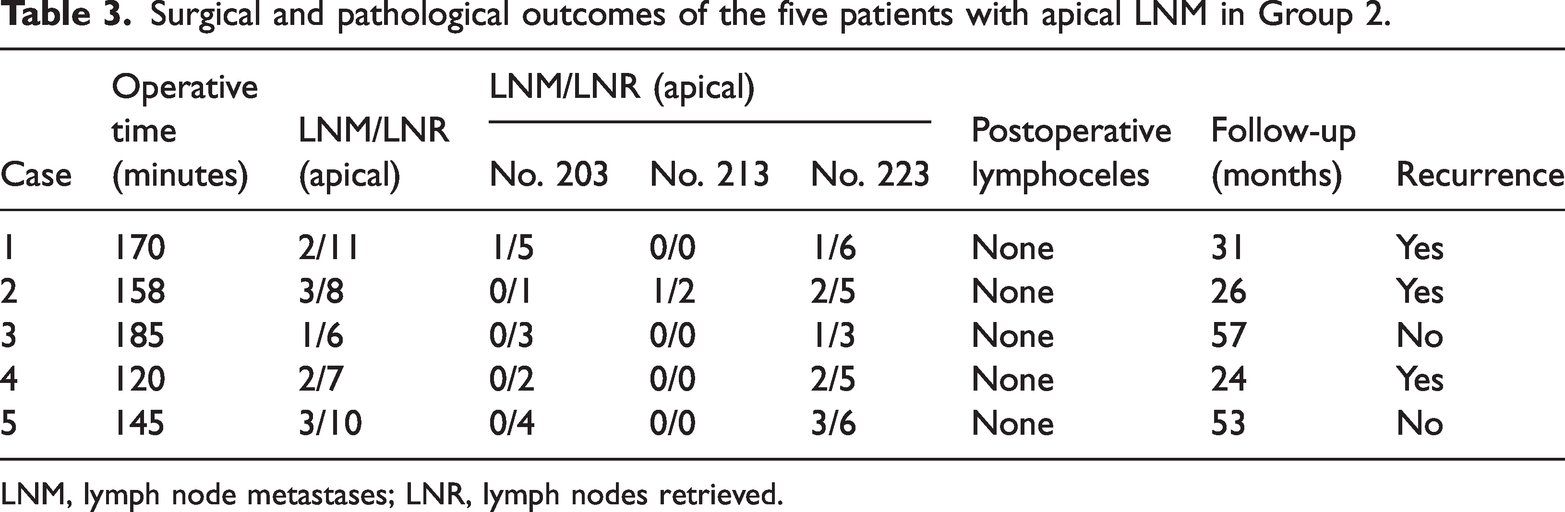
LNM, lymph node metastases; LNR, lymph nodes retrieved.
Follow-up results
During a median follow-up period of 45 months (range: 24–70 months), the 3-year DFS rate was 82.6% in Group 1 and 84.2% in Group 2. There was no significant difference in DFS between the two groups. The survival curves for DFS are shown in Figure 5.

Disease-free survival curves of Groups 1 and 2.
Discussion
Recent studies have compared segmental colectomy and right hemicolectomy for TCC management.8–11 However, a consensus on the optimal surgical approach remains elusive. The 5-year survival rate for TCC, ranging from 28% to 50%, is notably lower than that for other colorectal cancers, largely because of more extensive lymph node metastasis. 4 The number of dissected lymph nodes is a critical indicator of surgical quality and has important prognostic implications in colorectal cancer. For the pursuit of enhanced oncological outcomes, many surgeons lean toward extended right hemicolectomy for TCC, particularly involving the right transverse colon. This procedure involves ligation of the middle colic, right colic, and ileocolic vessels.4,12 By contrast, segmental colectomy focuses on ligation of the middle colic vessels only and is often considered less radical because of the lower number of lymph nodes dissected. From D3LND, inadequate attention to apical lymph nodes emerges as a primary factor. Metastasis in apical lymph nodes is correlated with a worse prognosis. 13 Although segmental colectomy is considered less intrusive in terms of surgical safety and maintains a longer normal colon length and the ileocecal junction, it falls short in terms of lymph node dissection. Preserving the ileocecal junction can alleviate hydro-electrolytic loss and facilitate adaptation to a postoperative diet. 14
According to the Atlas of Human Anatomy, 3 the lymphatic vessels of the right colon flow to the root of the superior mesenteric vessels along the main intestinal vessels, with interconnections at the root of the main vessels (Figure 1(a)). Theoretically, excision of all root lymph node groups (apical lymph nodes) could achieve optimal oncological outcomes. Laparoscopic segmental colectomy with ED3LND is designed to be less invasive while ensuring thorough oncological results. This approach emphasizes the comprehensive dissection of apical lymph nodes along the superior mesenteric vessels and their primary branches, while preserving the ileocecal junction and part of the ascending colon. By combining the strengths of segmental colectomy and right hemicolectomy, this method aims to balance oncological effectiveness with the preservation of functional outcomes. Compared with right hemicolectomy, our procedure minimizes unnecessary dissection and excision of the intestine and mesentery.
Currently, standardized surgical approaches for TCC include segmental colectomy, extended colectomy (right hemicolectomy), complete mesocolic excision, D3LND, and high middle colic vessel ligation. In this context, we have introduced a novel concept known as ED3LND, which is based on anatomical principles. Furthermore, our preliminary study has confirmed the feasibility of this procedure. Our recent comparative study showed that the number of retrieved lymph nodes and apical lymph node metastases in the ED3LND cohort were significantly higher than those in the D3LND cohort. The significant difference in the number of apical lymph node metastases between the two groups is encouraging; it serves as a preliminary demonstration of the oncological benefits of our procedure.
There was no significant difference in 3-year DFS between the two cohorts. We speculate that the limited sample size might have contributed to this outcome. Our study has some limitations, including the relatively low incidence of TCC, which may have resulted in inadequate statistical power due to the sample size. Additionally, this procedure may not be suitable for patients with a short transverse colon. Finally, although patients were randomly assigned to undergo D3LND or ED3LND, this study is still retrospective, and the reliability of the conclusions is inferior to that of a randomized controlled trial.
Conclusions
Our procedure resulted in a greater number of apical lymph nodes retrieved compared with laparoscopic segmental colectomy with D3LND, which may lead to better oncological outcomes. A large-scale prospective randomized controlled study is warranted to confirm the oncological superiority of this novel procedure. In this study, the higher incidence of apical lymph node metastases in the ED3LND group suggests that D3LND may be inadequate for patients with right-sided TCC.
Footnotes
Author’s contributions
XH conceived and designed the study, performed the operation, and drafted the article.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author declares no competing interests.
Ethics statement
The Ethics Committees of the Hunan Provincial People’s Hospital approved this study. Written informed consent regarding the operative techniques and data-use agreement was obtained from all patients before surgery.
Funding
Funding was provided by the Youth Science and Technology Talent Program of Hunan Provincial Science and Technology Department (2022RC1217), the Natural Science Foundation of Chang Sha city (kq2208110), and the High-level Talent Program of Hunan Provincial Health Commission (20240221-1015). The funding organizations had no role in the design and conduct of the study; the collection, management, analysis, or interpretation of the data; the preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.