
Abstract
Uterine rupture during pregnancy is a complication of placenta percreta. We present the case of a woman in her early 30s with a history of incomplete abortion treated by dilatation and curettage who was admitted with abdominal pain and vomiting at 30 weeks of gestation. She was diagnosed with thrombophilia and was administered anticoagulant drugs. After 10 hours of monitoring, the patient abruptly deteriorated. An emergency cesarean delivery showed a ruptured uterus due to placenta percreta. She accepted localized excision and uterine repair, and recovered well. Rupture of an unscarred uterus due to placental percreta is an extremely rare obstetric complication with high maternal and fetal mortality. This condition should be suspected in all pregnant women who have severe abdominal pain without being in labor. The treatment of uterine rupture due to placental percreta should be individualized, and repair of the uterus is possible in the majority of women.
Keywords
Introduction
Placenta accreta spectrum is used to describe the morbidly adherent placenta, and it includes placenta accreta, increta and percreta. 1 The overall incidence of placenta accreta spectrum is 1.7 cases/10,000 births. 2 Women with previous cesarean sections, placenta previa and those with previous damage to the uterine wall with a history of surgical abortion are at greater risk of placenta percreta. Placenta percreta has the potential to cause adverse events for the mother and the fetus. One of these rare adverse events is uterine rupture, which is an obstetric catastrophe with high maternal and perinatal morbidity/mortality.3–5 The clinical diagnosis of uterine rupture is challenging because of the broad variation in symptoms and progress. In all pregnant women presenting with an acute abdomen, regardless of the medical history and different trimesters, the likelihood of uterine rupture should be considered, and early surgical intervention results in a better prognosis.
We present a case of atypical uterine rupture in an unscarred uterus due to placenta percreta that occurred in the third trimester. The detailed analysis of this case could serve as a useful reference for the treatment and care of future patients with uterine rupture. The reporting of this study conforms to the CARE guidelines. 6
Case presentation
A woman in her early 30s, gravida 3, para 1, at 30 weeks of gestation was admitted to our hospital. Four years previously, she delivered a newborn vaginally and had an incomplete abortion treated by dilatation and curettage 1 year previously. In the early first trimester, she was diagnosed with thrombophilia and was maintained on aspirin 25 mg twice a day and low molecular heparin 1000 U daily, as required. No placental aberration was noted on a routine antenatal ultrasound check-up.
She was brought to our hospital by emergency medical services with the complaint of dull aching abdominal pain for 3 hours that had progressed to severe pain for an hour, associated with vomiting. Vaginal bleeding was not detected. Her pulse rate was 86 beats/minute and blood pressure was 104/62 mmHg. Her abdomen was tender and she had rebound pain but there was no shifting dullness. Cardiotocography was normal with a normal fetal heart rate and infrequent uterine contractions. Ultrasonography showed a normally developed fetus for 30 weeks of gestational age and a moderate amount of perihepatic effusion. There was no evidence of placental abruption or uterine rupture. A considerable increase in the white blood cell count (19.1 × 109/L) and neutrophil percentage (94%) was observed in laboratory tests. Coagulation was normal and the urinary amylase concentration was high at 694.0 U/L. The patient underwent an abdominal puncture owing to the possibility of intra-abdominal inflammation and hemorrhage, but this ultimately failed. She was in a fasting state, and was provided with rehydration, anti-infective treatment and an intramuscular injection of dexamethasone for fetal lung maturation. Ten hours later, the patient reported worsening of the abdominal pain. Her pulse rate increased to 108 beats/minute with a shock index of 0.95, and the hemoglobin concentration was decreased to 97 g/L. A repeated ultrasound scan suggested increased free fluid in the abdominal cavity. The gynecologist on duty quickly decided to deliver the newborn by cesarean section combined with a simultaneous exploratory laparotomy. More than 1500 mL of hemoperitoneum was removed. A tear of approximately 1 × 2 cm at the right of the uterine fundus with slow bleeding and placental tissue following removal of clots were observed (Figure 1).
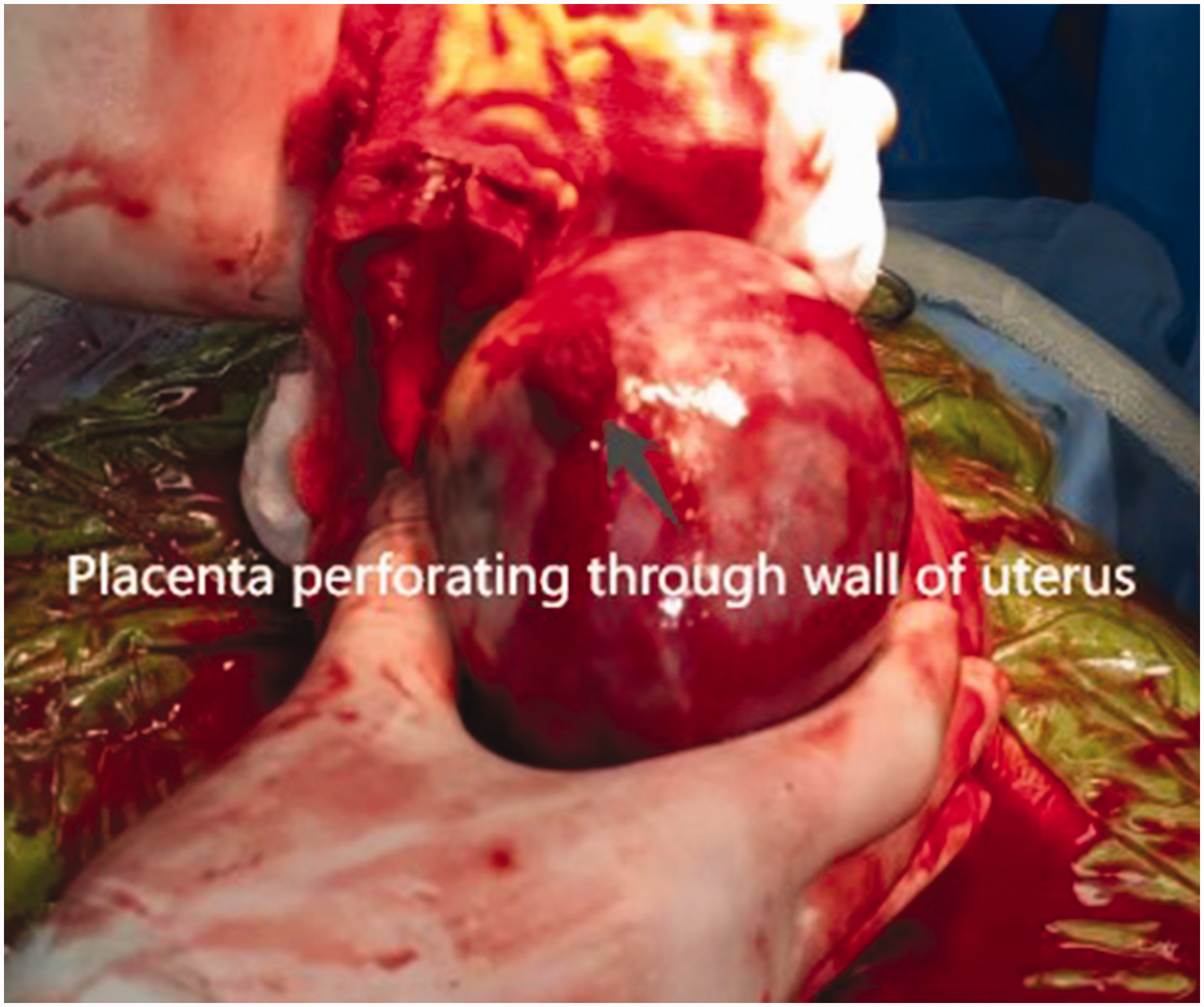
Photograph showing a tear of approximately 1 × 2 cm at the right of the uterine fundus with slow bleeding.
A female neonate with an Apgar score 8 at 5 min and a weight of 1520 g was delivered and admitted to the neonatal intensive care unit. Delivery of the placenta and manual removal of placental tissue from the rupture site and surrounding area were performed. Wedge resection of the ruptured uterine wall containing some placental tissue was then removed. Horizontal sutures followed by locking sutures were used to close the defect of the uterus. An intrauterine muscle injection of 20 IU oxytocin and an intravenous injection of 20 IU carbetocin were used to control the bleeding. No obvious laceration in the liver and spleen was observed during the examination. The hemoglobin concentration was 76 g/L at the time of surgery. The final estimated blood loss was 2.0 L, for which the patient received 3 units of packed red blood cells before being transferred to a higher level of care center with her neonate. Her posttransfusion hemoglobin concentration was 95 g/L.
Anti-infective treatment of ceftriaxone sodium was administered and her postoperative period was uneventful. Her white blood cell count was reduced to 17.0 × 109/L on the first postoperative day, and abdominal drainage and a urine catheter were in place for 2 days. She was discharged on the seventh postoperative day in a good condition and she was satisfied with the outcome. The infant was well without any neurological sequelae after a 6-month follow up. A histopathological examination showed that chorionic villi had penetrated the entire thickness of the myometrial smooth muscular layer at the site of the uterine rupture, and she was diagnosed with placenta percreta with uterine rupture.
All of the patient’s details have been removed to ensure the patient’s privacy, and written informed consent was obtained from the patient before treatment. Written informed consent for publication was not required because all of the patient’s details were de-identified. In addition, because of the nature of this study (case report), formal ethics committee approval was not required.
Discussion
Placenta percreta is an unusual cause of unscarred uterine rupture, and it is most prevalent in the third trimester of pregnancy.7–9 The risk factors for placenta percreta include previous uterine surgeries (caesarean delivery, myomectomy and metroplasty), dilatation and curettage for abortion and a previous history of manual removal of the placenta.10,11 Our patient had a prior uterine curettage, while routine obstetric ultrasound did not indicate placenta accreta spectrum, which may be related to the location of the placenta at the uterine fundus. An ultrasound scan only showed free fluid in the abdominal cavity when she was admitted to the hospital. This finding is similar to that found by Behera et al 12 and Fnon et al. 4
The signs and symptoms of uterine rupture are variable. The most common early sign is a non-reassuring fetal heart rate pattern, acute abdomen and antepartum hemorrhage.13–15 However, these features are not always evident. Before hemorrhage-induced circulatory collapse, symptoms and signs may be atypical or lacking altogether, particularly when uterine rupture is minimalized owing to the small size of the perforated wound. In the current case, the initial symptoms were only abdominal pain with nausea and vomiting, and there was no irregular fetal heart rate or vaginal bleeding. The only sonographic sign was the presence of a free blood clot in the peritoneal cavity. No irregular fetal heart rate or vaginal bleeding is unusual in placental percreta and uterine rupture. In our case, we initially misdiagnosed the patient as having liver rupture and inflammation. When the patient showed signs of shock, an emergency cesarean section was performed, the pregnancy was removed and the uterine disruption was repaired. Therefore, irrespective of the presence of risk factors, uterine rupture should be taken into account in every obstetric patient who shows hemodynamic instability or bleeding. In addition, because of the size of the uterus at 30 weeks of gestation, delivery is essential before any other abdominal surgery.
Many years previously, hysterectomy was considered as almost a panacea for treating a ruptured uterus or placenta percreta. Currently, however, many strategies of conservative therapy have been used for managing uterine rupture secondary to placenta percreta. These strategies include leaving the placenta in situ with packing, uterine curettage with packing, closing of the uterine defect, localized excision and uterine repair. Stepwise treatment or a combination of the above-mentioned strategies is frequently used, and careful patient selection and individualization are required. If the uterus is not severely lacerated, the patient has a stable hemodynamic condition, and if the patient has a further childbearing desire, conservative therapy may be arranged. These strategies also require the support of a strong surgical team. In women who choose to preserve fertility, the risk of a recurrent rupture is 4% to 19%. 16 In our case, we performed localized excision and uterine repair, and she recovered well.
Rupture of an unscarred uterus due to placental percreta is an extremely rare obstetric complication with high maternal and fetal mortality. This condition is difficult to be diagnosed, especially in non-high-risk women. This condition must be suspected in all pregnant women who have severe abdominal pain without being in labor. The treatment of uterine rupture due to placental percreta should be individualized, and repair of the uterus is possible in the majority of women.
Footnotes
Acknowledgements
The authors are grateful for the patient’s consent to be part of this study.
Author contributions
L.Z. was involved in project development, case analysis and manuscript writing.
L.H. was involved in project development, figure editing and manuscript editing.
X.H. was involved in project development, manuscript revising and other tasks (e.g., treatment procedure).
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available because they contain information that could compromise the privacy of the research participant.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Foundation of Ningbo Public Welfare Science and Technology Program (2022S036).