
Abstract
Objective
To identify the factors influencing postoperative ureteral stenosis following holmium laser lithotripsy.
Methods
A retrospective study was conducted of 106 patients who underwent ureteroscopic holmium laser lithotripsy. The effects of variables including stone location, stone size, the duration of surgery, water intake, disease duration, and stone-associated polyps were investigated.
Results
Logistic regression analysis revealed significant associations of ureteral stenosis with stone location, stone size, duration of surgery, water intake, disease duration, and stone-associated polyps. Patients with proximal stones, with large stones, who underwent long surgical procedures, who drank a large amount of water, who had long-term disease, and who had stone-related polyps were more likely to develop postoperative ureteral stenosis.
Conclusion
Significant perioperative complications of holmium laser lithotripsy are associated with prolonged disease, large ureteral stones, long incarceration periods, and the presence of polyps. Surgeons should consider these risk factors during the preoperative evaluation of patients and surgical planning to minimize the risk of postoperative ureteral stenosis.
Keywords
Introduction
Ureteroscopic holmium laser lithotripsy is increasingly widely employed in clinical practice, but the quantification of the pulse energy used for this procedure remains a challenge, and the delivery of an excessive amount of energy may cause harm. 1 Previous studies have explored the underlying causes of postoperative ureteral stenosis and the potential link with the thermal injury generated during the surgery. However, there have been some limitations to these previous studies and gaps remain in the literature. 2
Some previous studies have focused on individual factors, such as the size or location of stones, but there has been a lack of research in which the roles of multiple factors have been considered simultaneously. 3 In addition, the mechanisms by which these factors lead to ureteral stenosis are not fully understood. 4 For example, the relationships of the duration of surgery and the level of water intake with the development of ureteral stenosis have not been thoroughly investigated. 5
In this study, I aimed to address these limitations by conducting a comprehensive literature review and identifying the factors influencing ureteral stenosis following ureteroscopy holmium laser lithotripsy. 6 There has been insufficient research regarding the effects of combinations of various factors, including the stone location, stone size, duration of surgery, water intake, disease duration, and presence of stone-related polyps. 7 Furthermore, there is a need for further in-depth exploration of the specific mechanisms underlying the development of ureteral stenosis. 8 By retrospectively analyzing the data for patients with ureteral stones, I aimed to achieve a more detailed understanding of the effects of these factors on postoperative ureteral stenosis. 9 The results should contribute to a more complete understanding of the mechanism of postoperative ureteral stenosis and suggest novel targets for the clinical treatment of this condition. 10
Materials and methods
Collection of data
I performed a retrospective case–control analysis of patients with ureteral calculi who underwent treatment by ureteroscopic holmium laser lithotripsy. All of the participants provided their written informed consent, clearly indicating their agreement to participate in the study. They had all undergone an initial ureteroscopic holmium laser lithotripsy within the preceding year. Owing to the challenge associated with accurately measuring the duration of stone retention in a clinical setting, the key variables to consider include the patient’s medical history, the location of the stone, the presence of polyps, stone size, the duration of surgery, and the amount of fluid consumed by the patient. The duration of the disease here refers to the time period from the onset of symptoms related to ureteral stones, such as renal colic, hematuria, and frequent urination, to the time of surgical intervention. The reporting of the study complies with the STROBE guidelines. In addition, all the patient-related information has been anonymized to ensure the privacy and confidentiality of the participants. 11 The author obtained approval for the study from the Institutional Review Board of Dongguan Songshan Lake Central Hospital on March 17, 2022 (approval number: 2022-KYSB-032).
It was specified that participants should be patients aged 18 to 65 years who had been diagnosed with ureteral stones and were eligible for holmium laser lithotripsy. Several factors were taken into account in determining this, such as the age of the participants; the completion of imaging tests, such as renal pelvic X-ray, urinary tract computed tomography (CT), or ultrasonography; the ability to communicate effectively with medical staff; agreement to undergo holmium laser lithotripsy; and the completeness of the medical records. To minimize the potential for confounding by these factors, patients who were under 18 years old or over 65 years old, were unable to communicate effectively with medical staff, had incomplete medical records, had contraindications for holmium laser lithotripsy treatment, refused this treatment, or had undergone urinary tract drainage, such as by nephrostomy, were excluded.
Surgical procedure
Following successful intubation for general anesthesia or lumbar epidural anesthesia, patients were placed in position for lithotomy. The external genitalia were disinfected with iodine solution and a drape was applied. An 8-French (9.8) Wolf ureteroscope was guided into the bladder through the urethra with the aid of a uroscope infusion pump, with monitoring by a television system. A 4-French ureteral catheter was then placed into the affected ureter to guide the ureteroscope. Upon visualization of the ureteral stones, the ureteral catheter was slowly removed and replaced with a 550-µm holmium laser fiber. Holmium laser lithotripsy was then performed with an energy of 1.5 J and a frequency of 10 times/s, which caused the stones to disintegrate into fragments with diameters of approximately 2 to 3 mm. The fragmented stones were then gently removed using stone removal forceps, except for smaller fragments, which were left in the bladder to be passed naturally subsequent to surgery. Upward exploration of the ureter was then conducted to ensure that no residual stones were present. Afterwards, a 5.0-French double-J urethral catheter was inserted into the ureter to the renal pelvis, then anchored while the bladder was emptied. The ureteroscope was then removed from the bladder and urethra, and a catheter was inserted into the bladder for drainage. The double-J ureteral catheter was removed after surgery, at a time determined by the patient’s condition (whether there were residual stones, concurrent urinary tract infection, or concurrent ureteral stenosis).
Postoperative follow-up
During the first month following surgery, the patients attended weekly health consultations, when they underwent a physical examination. Any reported discomfort or abnormal physical examination findings, such as renal percussive pain, prompted further investigation.
During the first 6 months following surgery, a monthly urologic color Doppler ultrasound was conducted to assess ureteral patency. In addition, renal function was evaluated through the measurement of serum creatinine and urinalysis. If there were any symptoms, such as kidney stone-related pain, shivering, or high body temperature, a CT scan was performed to assess the severity of fluid accumulation in the kidney and identify the location of any obstruction. Patients with suspected ureteral stenosis underwent ureteroscopy to confirm the diagnosis and evaluate the extent of the stenosis.
One year after the surgery, a comprehensive evaluation, including a clinical examination, imaging evaluation, and functional assessments, was conducted. Based on the results, further treatment was instituted as required.
Assessment of the narrowing of the ureter
The renal tissue of the participants showed no notable abnormalities on B-ultrasonography, and the renal tissue swelling had decreased to within normal range. When lower back pain, chills, or fever was present, imaging, such as urological CT and intravenous urography, was used to assess the severity of hydronephrosis and to check for possible complications during ureteroscopy. Patients with suspected ureteral stenosis underwent weekly ureteral ultrasonographic examination when mild hydronephrosis was present.
Statistical analysis
Logistic regression analysis was conducted using IBM SPSS v.23.0 (IBM, Inc., Armonk, NY, USA), with the presence or absence of ureteral stenosis used as the dependent variable and factors such as stone location, size, operation time, water consumption, duration of disease, and presence of stone-related polyps used as independent variables. Continuous data are summarized as the mean ± standard deviation and datasets were compared using Student’s t-test. Categorical data are summarized as percentages and datasets were compared using the χ2 test. Statistical significance was accepted at P < 0.05.
Results
Postoperative complications of ureteral stenosis
A total of 111 patients were recruited. Two of them had to undergo retrograde intrarenal surgery because stones had escaped into their renal pelvis. Stones were extracted from two patients using lithotripsy forceps, because of their small size and accessible position. In addition, it was difficult to insert the ureteroscope because of lower ureteral stenosis in one patient. Therefore, 106 participants were studied. An examination of the clinical data revealed that of these, six experienced ureteral stenosis or atresia, with five affecting the upper ureter and one the mid-portion of the ureter (Table 1).
Features of ureteral stenosis following ureteral holmium laser lithotripsy.

Data are n (%) or mean ± SD.
Eighty-three percent of the participants with ureteral stenosis had a disease duration of ≥3 months, whereas only 35% of those without ureteral stenosis did; only 17% of the participants with ureteral stenosis had a disease duration of <3 months, compared with 65% of those without ureteral stenosis (χ2 = 5.628, P = 0.018), suggesting that a longer disease duration is associated with a higher risk of ureteral stenosis. Regarding stone location, 83% of the participants with ureteral stenosis had stones in the upper or mid-portion of the ureter, and distally positioned stones were present in 17% of the participants with ureteral stenosis. Of the participants without stenosis, 59% had distally positioned stones and 25% had stones in the upper or mid-portion of the ureter (χ2 = 9.650, P = 0.003), indicating that proximally-positioned stones increase the likelihood of ureteral stenosis. The presence of urethral polyps also showed a significant association. In the group without urethral polyps, 17% of the participants had ureteral stenosis and 68% did not (χ2 = 6.565, P = 0.01). The mean stone diameter significantly differed between patients with and without ureteral stenosis: the mean stone diameter of patients with ureteral stenosis was 1.48 ± 0.43 cm, while that of patients without was 0.90 ± 0.50 cm (t = −6.049, P < 0.001), implying that larger stones contribute to the development of ureteral stenosis. The mean duration of surgery also differed significantly between the groups: the mean duration for patients with ureteral stenosis was 66.7 ± 32.8 minutes, while that for patients without was 37.6 ± 16.7 minutes (t = −2.837, P = 0.005), suggesting that longer procedures are associated with a higher risk of ureteral stenosis. Finally, the mean water consumption of the participants also significantly differed: the mean daily water consumption of participants with ureteral stenosis was 2500 ± 775 mL, while that of patients without was 1280 ± 656 mL (t = −5.51, P < 0.001), indicating that greater water consumption is associated with a higher risk of ureteral stenosis (Figure 1).
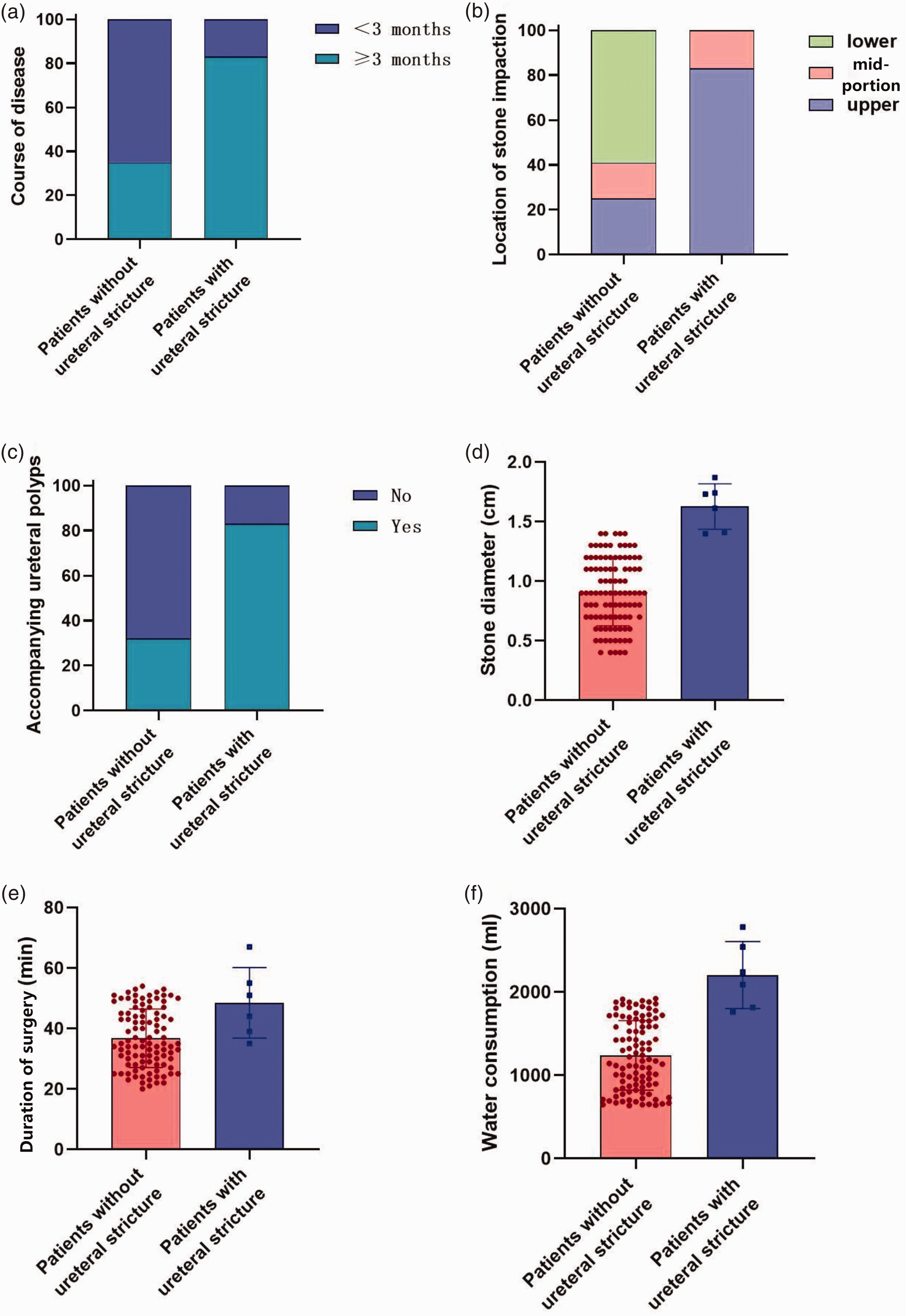
Analysis of the relationships between various parameters and the risk of ureteral stenosis. (a) Relationship between the duration of disease and ureteral stenosis. (b) Relationship between stone location and ureteral stenosis. (c) Relationship between urethral polyps and ureteral stenosis. (d) Relationship between stone size and ureteral stenosis. (e) Relationship between the duration of surgery and ureteral stenosis and (f) relationship between water consumption and ureteral stenosis.
Logistic regression analysis revealed significant associations between ureteral stenosis and several of these variables: stone location, stone size, the duration of surgery, water intake, disease duration, and the presence of stone-associated polyps (all P < 0.05). Patients with proximally-positioned stones, with large stones, who underwent long surgical procedures, who drank a lot of water, who had long-term disease, and who had stone-associated polyps were more likely to develop postoperative ureteral stenosis.
Factors that increase the risk of ureteral stenosis following ureteral holmium laser lithotripsy
Logistic regression analysis of the potential risk factors for ureteral holmium laser lithotripsy indicated that the location of the stone (odds ratio (OR) = 7.042, χ2 = 4.926, P = 0.026), stone size (OR = 3.546, χ2 = 5.273, P = 0.022), the duration of surgery (OR = 1.059, χ2 = 7.215, P = 0.007), fluid intake (OR = 1.002, χ2 = 9.482, P = 0.002), disease duration (OR = 5.231, χ2 = 5.152, P = 0.023), and the presence of stone-associated polyps (OR = 9.358, χ2 = 3.622, P = 0.03) were significant risk factors for ureteral stenosis. These findings indicate that proximally-located and larger stones, those that required longer surgical procedures to remove, greater water consumption, a disease duration of >3 months, and the presence of polyps increase the risk of ureteral stenosis.
Treatment of ureteral narrowing following ureteral holmium laser lithotripsy
Two patients with ureteral stenosis were treated using laparoscopic pyeloureteroplasty, ureterostomy, and the placement of a ureteral stent. After the surgery, three standard double-J tubes were inserted. After monitoring the patients for 6 months, the ureteral stents were removed, and intravenous pyelography revealed notable decreases in hydronephrosis.
Discussion
The purpose of the present study was to investigate the effects of various parameters on postoperative ureteral stenosis following holmium laser lithotripsy, to provide a reference for future clinical treatment. 12 Through the detailed analysis of data relating to 106 patients, I have been able to draw some important conclusions. 13
First, the location and size of the stone, the duration of surgery, fluid intake, disease duration, and the presence of stone-related polyps are closely associated with ureteral stenosis. 14 Specifically, patients with proximal stones, with large stones, who undergo long procedures, who drink a lot of fluid, who have had disease for >3 months, and who have stone-related polyps are more likely to experience postoperative ureteral stenosis. 15 These findings are consistent with the results of some previous studies, which confirms the importance of these factors in the occurrence of ureteral stenosis. 16
Second, I have shown that the risk of complications is significantly higher when surgery is required for complex situations, such as long-term disease, large ureteral calculi, a long duration of incarceration, and polyps. 17 This suggests that physicians should fully consider the characteristics of each patient when choosing the most appropriate procedure and conduct a comprehensive preoperative evaluation so that personalized treatment plans can be developed and the surgical outcomes and the risks of complications can be predicted more accurately. 18
Third, I have discussed some details of the surgical procedures involved. 19 For example, for the treatment of upper ureteral calculi, to prevent stones from moving into the renal pelvis, the water pressure used for irrigation can be reduced; this, however, can lead to difficulty with visualization during surgery and increase the risk of the ureteral mucosa being accidentally injured by the holmium laser, and thereby lead to ureteral stenosis. 20 Therefore, during surgery, physicians need to balance the importance of the treatment of the urolithiasis and the protection of the mucosa. 21
Ureteral stents are highly flexible, elastic, can be securely attached, and are effective means of drainage. Postoperative ultrasonography or pelvic X-ray can be used to show the location of the stent, which aids with the drainage of hydronephrosis and the widening of the ureter for urological procedures. The insertion of dual-J ureteral stents helps prevent urinary tract obstruction or prolonged ureteral narrowing, owing to ureteral mucosal swelling, scarring, or other factors that lead to ureteral damage.
During laparoscopic pyeloureteroplasty and ureterostomy, the primary procedure consists of excising the constricted portion of the ureter and reconnecting the damaged ends. Because of variations in the location and extent of ureteral stenosis, the surgical approach used differs, and this requires the operator to assess the state of the affected ureteral segment (Figure 2). Open surgery is frequently used as a complementary approach when other treatments for ureteral stenosis have not been successful. However, laparoscopic pyeloureteroplasty is preferred to conventional open surgery for the treatment of ureteral stenosis because it is less traumatic; has a lower risk of complications; and is associated with a shorter hospital stay, a quicker recovery, and superior surgical outcomes.
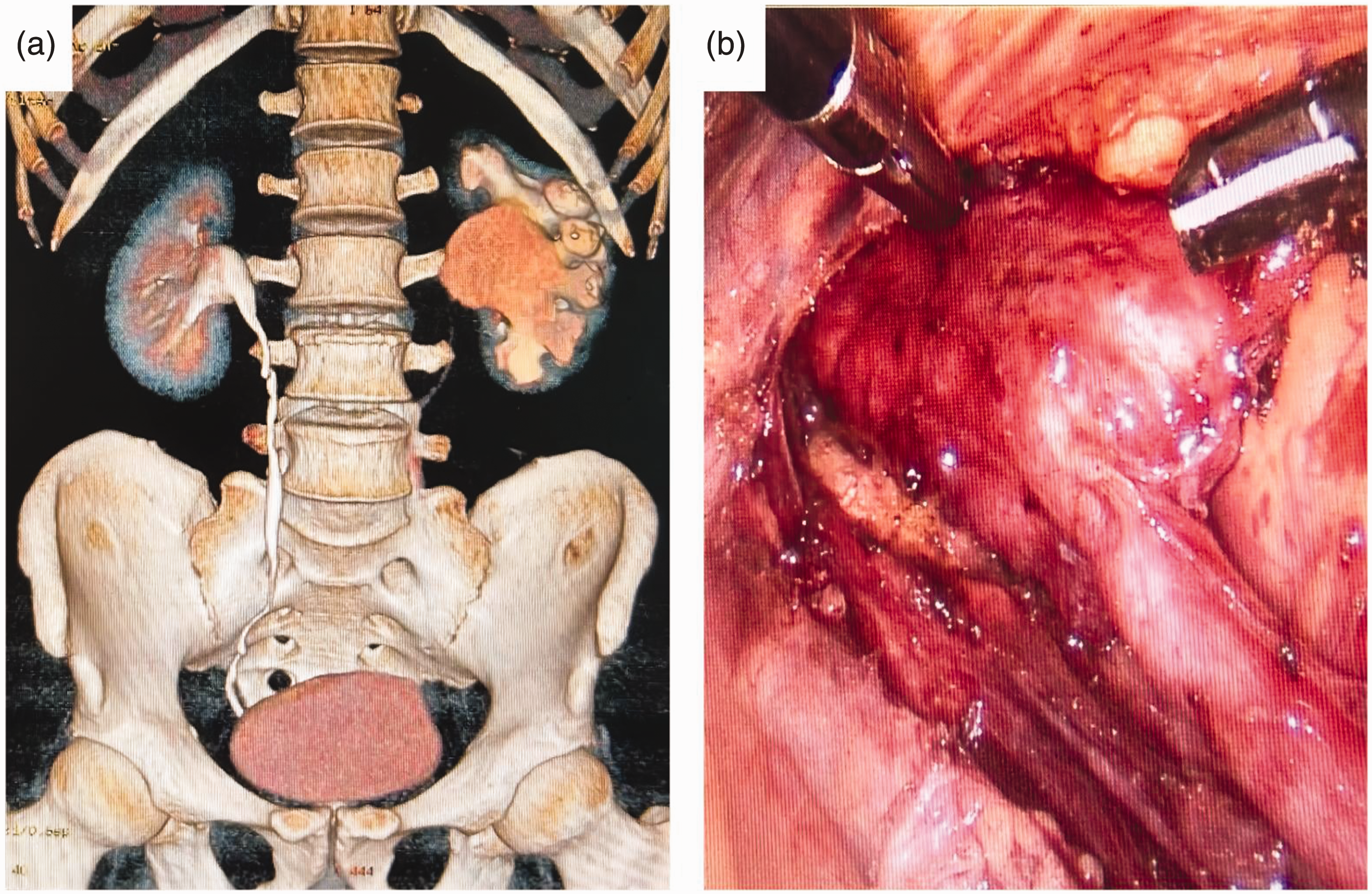
Images of a 39-year-old man who underwent laparoscopic pyeloureteroplasty because of left ureteral stenosis. (a) Preoperative computed tomography image reconstructed in three dimensions and (b) severe ureteropelvic junction obstruction was apparent intraoperatively.
In view of the present findings, I propose some measures to facilitate the balancing of the treatment of urolithiasis with the proception of the ureteral mucosa. 22 First, preoperative planning and prediction of the outcomes of the procedure should be more accurate. 23 Through detailed imaging and assessment of the disease, the location, size, and shape of the stones and the condition of the ureter should be determined, to permit appropriate preparation for the surgery. 24 Furthermore, advanced imaging techniques, such as ultrasonography and CT, can be used during surgery to more accurately characterize the situation of the stones in the ureters and patient monitoring during the procedure can be augmented using various visualization devices and auxiliary robots to improve its accuracy and safety. 25 In addition, physicians should constantly improve their surgical skills, strengthen their teamwork, shorten the procedure, and manage complex situations in a timely fashion to reduce the incidence of complications. 26
In future studies, the interactions between the identified factors should be characterized, to facilitate improvements in the prevention and treatment of ureteral stenosis. 27 For example, large, multicenter studies should be performed to verify the present findings and explore new treatment methods and technologies. 28 In addition, inter-individual variations among patients should be recognized and the effects of postoperative nursing on the prognosis of patients should be studied, such that personalized treatment and nursing programs can be formulated. 29
The present study had certain limitations. Although I have identified several factors that are associated with ureteral stenosis after holmium laser lithotripsy, further quantitative research is needed regarding the nature of the pulse energy supplied and the harm it can cause. 30 In addition, although the study has provided valuable insight into the relationship between these factors and ureteral stenosis, the specific mechanisms mediating the relationship requires further exploration. 31 Finally, the study would have benefitted from a larger sample size and a more comprehensive analysis of potential confounding factors. However, these limitations do not diminish the importance of the findings, and the study provides a solid foundation for further research in the field.
Conclusions
In the present study, I have shown that specific factors are linked to a higher probability of postoperative ureteral stenosis following holmium laser lithotripsy. In patients with sizable ureteral stones, an extended period of incarceration, and polyps, there is a notably higher risk of developing ureteral stenosis. Large ureteral stones may pose a challenge during the surgical procedure. They may require more extensive fragmentation, which prolongs the procedure and may increase the risk of damage to the surrounding tissues, including the ureteral mucosa. Long incarceration times also expose the ureter to prolonged irritation, which may also contribute to the development of stenosis. Furthermore, the presence of polyps adds complexity to the surgical procedure. Polyps may obstruct the surgeon’s view and impede the manipulation of the laser fiber, increasing the difficulty and duration of the surgery. In such cases, surgeons may have to exert more force or perform additional maneuvers to remove or debulk the polyps, which increases the risk of inadvertent injury to the ureteral mucosa. This, in turn, would increase the risk of postoperative ureteral stenosis. It is crucial for surgeons to be aware of these risk factors and to consider them during the preoperative evaluation and surgical planning. Careful consideration of the stone size, incarceration time, and the presence of polyps will help physicians anticipate potential complications and take appropriate measures to minimize the risk of postoperative ureteral stenosis.
In conclusion, this study highlights the importance of identifying risk factors that may contribute to postoperative ureteral stenosis following holmium laser lithotripsy. A better understanding of the impact of large stones, a long incarceration time, and the presence of polyps on the surgical outcomes should aid with patient selection, surgical decision-making, and overall patient care. Future research and advances in surgical techniques and equipment may further support efforts to reduce the incidence of ureteral stenosis and improve patient outcomes.
Footnotes
Acknowledgements
The author thanks the staff of the Department of Urology, Dongguan Songshan Lake Central Hospital.
Declaration of conflicting interest
The author declares that there is no conflict of interest.
Funding
This research was supported by the Dongguan Science and Technology of Social Development Program (grant no. 20221800900642).