
Abstract
Objective
To describe antibiotic prescription patterns in the emergency department (ED) of a tertiary healthcare center in Nepal.
Methods
This was a descriptive cross-sectional study of hospital records of patients who visited the ED.
Results
Of the 758 ED patients included in the study, 384 (50.6%) received a total of 536 antibiotic prescriptions. Common indications for antibiotic prescriptions included respiratory infection (37.5%), gastrointestinal infection (19.3%), urinary infection (10.4%), and prophylaxis (29.9%). Antibiotics listed as essential in the National List of Essential Medicines (NLEM) and generic formulations were used in 77.1% and 61.9% of the antibiotic prescriptions, respectively. Injectable antibiotics were prescribed to 54.9% of the 384 patients. Frequently prescribed antibiotics included ceftriaxone (34.1%), metronidazole (18.5%), amoxicillin + clavulanic acid (15.9%), and cefixime (14.3%). Bacterial culture testing was performed in 15.1% of the patients who received antibiotics.
Conclusions
This study showed that overuse of antibiotics, prescription of branded antibiotics, prescription of antibiotics not listed in the NLEM, prophylactic use of antibiotics, and empirical treatment of suspected infections without isolation of pathogens were all prevalent. We recommend more research to determine the causes underlying these practices and develop interventions to limit such practices.
Keywords
Introduction
In 2002, the World Health Organization (WHO) reported that more than 50% of all medicines are prescribed, dispensed or sold inappropriately, and 50% of patients do not take medications correctly. 1 Such inappropriate use of medicines, particularly antibiotics, leads to poor patient outcomes, adverse drug reactions, antimicrobial resistance (AMR), and higher total healthcare system costs. 1
AMR is one of the most worrying consequences of inappropriate antibiotic use. 2 The problem is compounded by the paucity of new antibiotic drugs being developed. The development of AMR eventually leads to substantial human morbidity, mortality, and economic burden. 2
Monitoring antibiotic prescribing patterns is essential to identify and describe the problem of inappropriate antibiotic use. It can also help to guide measures to promote appropriate use of antibiotics and to assess the effect of those measures. 1 Hence, collecting and reporting data on the use of antimicrobial agents in humans is part of the WHO Global Action Plan on Antimicrobial Resistance. 3
In Nepal, prescription of antibiotics by under-qualified health workers, inappropriate use of antibiotics, unregulated dispensing of antibiotics, and self-medication of antibiotics without prescription are all prevalent practices. 4 Consequently, a progressive increase in antibiotic resistance has been reported in Nepal. 5
The emergency department (ED) setting presents a unique set of circumstances in relation to antibiotic prescription. A substantial proportion of ED visits are prompted by infections, 6 so antibiotics are one of the most frequently prescribed medications in the ED. 6 Patients presenting to the ED may have life-threatening infections that require prompt intervention. These patients are frequently considered for empirical antibiotic administration before the causative microorganism has been cultured and identified. 6 An empirical antibiotic is usually selected after considering possible causative pathogens and their patterns of resistance in the local population.
Some community-based and hospital-based studies conducted in Nepal have reported on antibiotic usage. 5 However, a search in the PubMed database failed to identify any studies carried out in Nepal on antibiotic prescription patterns in ED settings. In this study, we aimed to determine the prevalence and describe the patterns of antibiotic prescription in the ED of a tertiary healthcare center in Nepal.
Materials and methods
Study design and setting
This was a descriptive cross-sectional study of hospital records of patients who presented to the ED of a tertiary healthcare center in Nepal from 1 February 2023 to 31 July 2023. Ethical approval was obtained from Kathmandu University School of Medical Sciences Institutional Review Committee (approval number 248/22). The study protocol conforms to the ethical guidelines of the Declaration of Helsinki of 1975, as revised in 2013. This study adhered to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. 7 All participants provided written informed consent.
Study participants and selection criteria
A systematic sampling method was used. Patients were enrolled in the study on every eighth day. All eligible patients who presented to the ED on that day were included. We excluded the records of patients aged less than 1 years. We also excluded records of patients presenting to the Obstetric and Gynecological ED, which is a separate unit at our center.
Data collection
Patient records were reviewed and relevant data were collected. Data collection was carried out by five ED medical officers. Two sessions were conducted by the ED faculty team, which included the principal investigator, to train the physicians responsible for data collection. The training sessions covered the purpose of the study, data extraction, and the format of recording prescription information. At the end of the sessions, a practice exercise was conducted in which each individual independently recorded the data of 10 patients under supervision. Each session lasted for approximately 2 hours. Once per week, follow-up sessions lasting approximately 1 hour each were conducted to guide and monitor the physicians responsible for data collection. A standardized patient information collection form was used to collect the data. Data were then entered into a spreadsheet in IBM SPSS Statistics for Windows, Version 27.0 (IBM Corp., Armonk, NY, USA). The confidentiality and anonymity of the patients were maintained during the process of retrieving the data from the records. The record files are maintained under password protection by the principal investigator.
Study variables
The variables analyzed were age, sex, indication for antibiotic use, names of antibiotics used, routes of administration, and bacterial culture report.
Operational definitions
Antibiotics
The WHO guideline on investigation of drug use in health facilities was followed. 8 Drugs classified as penicillin, other antibacterials (such as sulfa drugs), anti-infective dermatologics, anti-infective ophthalmic agents, and anti-diarrheals with antibiotics in the WHO Model List of Essential Drugs were counted as antibiotics. However, antileprotics, antituberculotics, antimalarials, antifungals, antiprotozoals, and anthelmintics were not considered to be antibiotics. 8
Essential drugs
These were defined as those drugs listed as essential in the 2021 Nepal National List of Essential Medicines (NLEM). 9
Generic names
Generic drugs were determined according to the list of generic drug names in the Nepal NLEM. 9
Study size
The sample size was calculated based on the standard formula 10 for cross-sectional studies: n = Z*P*(1−P)/d2, where Z is 1.96 for a 95% level of confidence, P is the estimated proportion of the prevalence of the primary outcome, taken as 50% for maximum sample size calculation, and d is the desired level of precision, which was set at 0.05. The calculated sample size was 384. We also considered that the WHO recommends a sample size of 600 patient encounters when investigating drug use in health facilities. 8 A total of 758 eligible patients presented to the ED during the study period and we included all their records in this study.
Statistical analysis
Continuous variables were described in terms of mean, 95% confidence interval, standard deviation, and range. Categorical variables were reported as frequencies and percentages. All statistical analyses were performed using the IBM SPSS Statistics for Windows, Version 27.0 (IBM Corp., Armonk, NY, USA).
Results
Of 758 eligible patients who presented to the ED during the study period, 384 (50.6%) were prescribed at least one antibiotic. Only the records of these 384 patients were included in the subsequent analyses. The age of patients who were prescribed antibiotics ranged from 1 to 100 years. The median age was 50 years with an interquartile range of 41 years. Among the patients prescribed antibiotics, 208 (54.2%) were men and 176 (45.8%) were women; the male-to-female ratio was 1.18:1.
Indications for antibiotic prescriptions included respiratory infection (n = 144, 37.5%), gastrointestinal infection (n = 74, 19.3%), urinary infection (n = 40, 10.4%), bacterial meningitis (n = 5, 1.3%), skin infection (n = 4, 1.0%), sexually transmitted infection (n = 2, 0.5%), and prophylactic use (n = 115, 29.9%). These findings are illustrated in Figure 1.
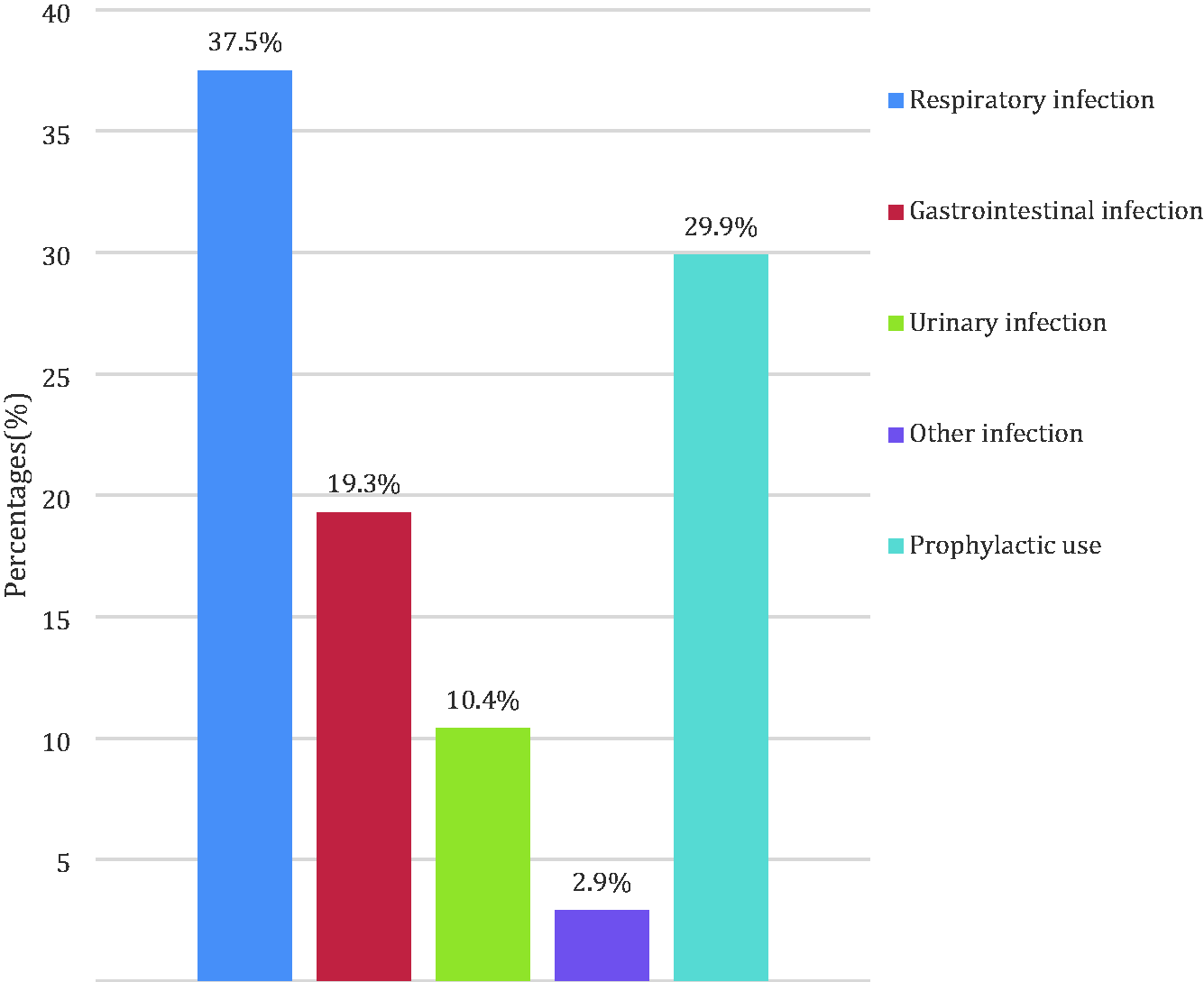
Indications for antibiotic use in the study participants (n = 384).
Of the 384 (50.6%) patients who were prescribed at least one antibiotic, 256 (66.7%) were prescribed a single antibiotic, 105 (27.3%) were prescribed two antibiotics, 22 (5.7%) were prescribed three antibiotics, and 1 (0.3%) was prescribed four antibiotics.
A total of 536 antibiotic prescriptions were made for the 384 patients. Of these 536 prescriptions, 413 (77.1%) used antibiotics listed in the Nepal NLEM. Of the antibiotic prescriptions, 332 (61.9%) used generic antibiotics.
Of the 384 patients, 211 (54.9%) received at least one antibiotic through an intravenous (parenteral) route. Of the total 536 antibiotic prescriptions, 275 (51.3%) were intravenous (parenteral) antibiotics, 247 (46.1%) were oral antibiotics, and 14 (2.6%) were topically administered. Figure 2 shows the various routes used in antibiotic prescriptions.

Routes used in antibiotic prescriptions (n = 536).
The antibiotics that were used in the study population (n = 384) were as follows: ceftriaxone (n = 131, 34.1%), metronidazole (n = 71, 18.5%), amoxicillin + clavulanic acid (n = 61, 15.9%), cefixime (n = 55, 14.3%), azithromycin (n = 49, 12.8%), cefuroxime (n = 49, 12.8%), ciprofloxacin (n = 42, 10.9%), mupirocin (n = 14, 3.6%), doxycycline (n = 14, 3.6%), flucloxacillin (n = 14, 3.6%), cefotaxime (n = 9, 2.3%), piperacillin + tazobactam (n = 6, 1.6%), nitrofurantoin (n = 5, 1.3%), amoxicillin (n = 3, 0.8%), amikacin (n = 3, 0.8%), moxifloxacin (n = 3, 0.8%), clindamycin (n = 2, 0.5%), meropenem (n = 2, 0.5%), levofloxacin (n = 1, 0.3%), ampicillin + cloxacillin (n = 1, 0.3%), and clarithromycin (n = 1, 0.3%). The prevalence of use of various antibiotics in the study population is shown in Figure 3.

Antibiotics frequently used among the study participants (n = 384).
Bacterial culture and antibiotic susceptibility testing were performed in 58 (15.1%) patients. The specimens used were urine (n = 23, 39.7%), sputum (n = 16, 27.6%), blood (n = 14, 24.1%), ascitic fluid (n = 3, 5.2%), and throat swab (n = 2, 3.4%). Of the 58 culture specimens, pathogenic organisms were isolated in 11 (18.9%). Isolated organisms included Escherichia coli (n = 6), Staphylococcus aureus (n = 2), Enterococcus (n = 1), Klebsiella (n = 1), and yeast (n = 1).
Discussion
We report that 50.6% of the patients who presented to the ED were prescribed at least one antibiotic. Other studies conducted in Nepal have reported that the percentage of patient encounters with at least one antibiotic prescription was 43.95% in an outpatient setting 11 and 44.7% in public health facilities in one district. 12 Frequent use of empirical antibiotics in the ED setting may have contributed to the higher prevalence of antibiotic use reported in our study. 6 Notably, the percentage of patients who are prescribed antibiotics should ideally be less than 30%, according to the WHO. 13
In the study population, common indications for antibiotic prescriptions were respiratory infection, gastrointestinal infection, and urinary infection. Similar findings have been reported in studies conducted in other hospitals in Nepal.11,14 In a study conducted in the United Arab Emirates, common indications for antibiotic prescription were respiratory infection (34.83%), urinary infection (34.19%), sepsis (14.83%), and gastrointestinal infection (7.09%). 15 However, in some studies, skin infection is the most common indication of antibiotic use.16,17 We attribute this disparity to the local epidemiological conditions and variations in patient populations visiting the respective hospitals, among other factors.
Among the patients who were prescribed antibiotics, one, two, three, and four antibiotics were prescribed to 66.7%, 27.3%, 5.7%, and 0.3% of patients, respectively. Another study conducted in Nepal 18 reported an even higher proportion of patients receiving multiple antibiotics. However, use of multiple antibiotics was less prevalent in studies conducted in Jordan 19 and Turkey 20 than in the present study. Lack of knowledge about appropriate antibiotic prescribing and the need for broad antibiotic coverage in settings where isolation of pathogens is not feasible are possible explanations for these findings.
In the present study, 77.1% of the prescribed antibiotics are mentioned in the NLEM of Nepal. This proportion is higher than that reported in another study carried out in a hospital in western Nepal (67.1%). 21 However, an even higher proportion was reported in a study from Guyana (91%). 22 According to the WHO, all prescriptions should be made according to the NLEM. 13 Prescribing drugs included in the NLEM is a key aspect of appropriate prescribing.1,22 Such prescribing would help to increase the availability and cost-effectiveness of medicines. In addition, the prescribed medicines would be appropriate for local disease occurrence and drug resistance patterns.1,9 The development of the NLEM took into consideration national guidelines. 1 Therefore, the proportion of drugs prescribed from the NLEM may represent a measure of the level of compliance of physicians to national guidelines.
We found that 61.9% of the antibiotic prescriptions used generic antibiotics. The proportion of generic antibiotics prescribed was 30% in a study from Guyana. 22 The WHO recommends an optimal generic prescribing rate of 100%. 13 Advertisements, the influence of pharmaceutical companies and physician beliefs that branded drugs are superior to generic drugs may be some of the reasons why branded antibiotics are prescribed.11,24 However, the use of branded rather than generic drugs can lead to increased treatment costs, confusion about drug terminology, barriers in communication among healthcare providers, and adverse drug events. 24
In this study, 54.9% of patients received intravenous (parenteral) antibiotics. Other subtypes of parenteral drug administration were not used. Patients in the ED generally require rapid intervention. Moreover, oral absorption of drugs may not be reliable in some patients presenting to the ED. Hence, intravenous or other parenteral routes of drug administration are used more frequently in the ED than in some other healthcare settings. Previous studies have reported even higher proportions of injectable antibiotic use in hospitals in South Africa (85.25%), 17 northern India (71%), 25 and Eritrea (81.4%). 26 In contrast, a study conducted in an outpatient setting in Nepal reported a much lower use of injectable antibiotics (5.06%). 11 Overuse of injectable antibiotics is also inappropriate and should be avoided. 1
In the present study, the most frequently prescribed antibiotics were ceftriaxone (34.1%), metronidazole (18.5%), amoxicillin + clavulanic acid (15.9%), cefixime (14.3%), azithromycin (12.8%), cefuroxime (12.8%), and ciprofloxacin (10.9%). In another study conducted in the public health facilities in one district of Nepal, the most frequently prescribed antibiotics were ceftriaxone (22.9%), amoxicillin (16.6%), metronidazole (12.5%), ciprofloxacin (11.4%), and cotrimoxazole (7.2%). 12 Ceftriaxone was found to be the most commonly prescribed antibiotic in several other studies conducted in Nepal. 5 A study from Pakistan reported the most frequently used antibiotics to be ceftriaxone (71.8%), cefotaxime (5.6%), metronidazole (4.7%), amoxicillin (4.7%), and ciprofloxacin (4.2%). 2 In contrast, a study carried out in Ethiopia reported the most commonly prescribed antibiotics to be amoxicillin (16.4%), ampicillin (15.0%), gentamicin (14.9%), and chloramphenicol (11.6%). 23
According to the 2023 National Antimicrobial Treatment Guidelines of Nepal, the use of ceftriaxone is recommended in patients with several diseases, including acute bacterial meningitis, severe community-acquired pneumonia, nosocomial pneumonia, enteric fever, gonorrhea, abscess, wound infection, acute appendicitis, acute cholecystitis, puerperal sepsis, postabortal infection, pelvic inflammatory disease, cervical discharge, urethral discharge, and scrotal swelling.9,27 The widespread recommendations for ceftriaxone, as well as its broad spectrum of antibacterial activity, low toxicity, and easy availability may help to explain its frequent use. 28 However, heavy use of cephalosporins such as ceftriaxone can lead to the development and multiplication of antimicrobial-resistant microorganisms. 28
In the present study, a significant proportion (29.9%) of antibiotic prescriptions were for infection prophylaxis. Prophylactic antibiotics are used in our ED for some patients presenting with trauma, snake bites, burns, and before surgical interventions. Previous hospital-based studies have reported the proportion of prophylactic antibiotic use to be 30.9% in central Nepal, 11 5.9% in western Nepal, 21 and 20.4% in northern India. 25
In the present study, bacterial culture and antibiotic susceptibility testing was conducted in 15.1% of the patients who underwent treatment with antibiotics. A study carried out in another hospital in Nepal reported bacterial culture testing in 19.8% of cases. 18 In a hospital in northern India, culture and sensitivity tests were performed in 34.7% of patients undergoing antibiotic therapy. 25 In cases of suspected infections treated with antibiotics, the National Antimicrobial Treatment Guidelines recommend ensuring that relevant microbiological tests are performed. 27 However, low utilization of bacterial culture and sensitivity tests, as in our case, can lead to prolonged and extensive use of broad-spectrum antibiotics instead of narrow-spectrum antibiotics. 29 This ultimately leads to the development of AMR and increased treatment costs.
Limitations
This study was conducted in the ED of a single healthcare center, so the findings may not be generalizable to other healthcare settings or the general population of Nepal. The study period was 6 months; therefore, we did not take into account seasonal variations in disease prevalence and antibiotic use. As reported above, microbiological tests to isolate the pathogens were not performed in most cases before initiation of antibiotics. Therefore, we were unable to report on the appropriateness of prescriptions and the antibiotic susceptibility pattern. However, we believe that these findings provide key insights that will help to clarify antibiotic prescribing patterns in Nepal.
Conclusions
This study adds to the body of knowledge related to antibiotic use in Nepal and other developing countries. We report that overuse of antibiotics, prescription of branded antibiotics, prescription of antibiotics not listed in the NLEM, prophylactic use of antibiotics and empirical treatment of suspected infections without isolation of pathogens are all prevalent in Nepal.
We recommend that more research be carried out to determine the reasons for inappropriate prescribing practices, and the development of targeted measures to promote appropriate prescription of antibiotics. Furthermore, we recommend further surveillance and assessment of antibiotic use at healthcare facilities to quantify antibiotic use patterns. Measures to improve access and compliance to the NLEM as well as national guidelines are also warranted.
Footnotes
Acknowledgements
We would like to thank all the hospital emergency department staff for their direct and indirect contributions to this study.
Author contributions
Samjhana Basnet conceptualized, designed and supervised the study. Aashish Karki and Sumina Mainali collected the data. Prabhat Silwal carried out the analysis. All the authors were involved in the interpretation of the results. Prabhat Silwal wrote the first draft of the manuscript. All the authors were involved in the preparation and review of subsequent drafts. All authors approved the final draft for publication.
Data availability statement
Data generated or used in this study are available from the corresponding author on reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study received no specific grants from any funding agency in the public, commercial or not-for-profit sectors.