
Abstract
Pheochromocytoma crisis is rare but potentially fatal if not recognized early and properly managed. Here, a woman in her 20s with a paraganglioma-induced pheochromocytoma crisis, who was successfully treated by veno-arterial extracorporeal membrane oxygenation (VA-ECMO) and interval tumor resection, is described. In July 2022, the patient was brought to hospital with a complaint of sudden-onset of palpitations with vomiting. The patient developed cardiorespiratory failure with hypoxia. Computed tomography scan showed pulmonary oedema and a mass anterior to the inferior vena cava. She was transferred to the intensive care unit and treated with VA-ECMO. The patient’s ECMO was withdrawn after 6 days without any complications. After hemodynamic stabilization, the patient underwent tumor resection 4 months later. The postoperative course was uneventful and she was discharged on postoperative day 7. Histopathological analysis confirmed a paraganglioma. VA-ECMO may play a significant role in saving lives and providing time for accurate diagnosis and specific treatment of a patient with pheochromocytoma crisis. Appropriate individual management can help avoid the occurrence of ECMO complications.
Keywords
Introduction
Pheochromocytomas and paragangliomas are rare neuroendocrine tumors arising from chromaffin cells of the adrenal medulla or extra-adrenal tissues. They mainly synthesize, secrete, and release a large number of catecholamines, such as norepinephrine, epinephrine, and dopamine. 1 Pheochromocytoma crisis is a rare but life-threatening condition that may lead to multiple organ failure and hemodynamic instability caused by uncontrolled catecholamine release. The crisis is the primary clinical manifestation in some patients with pheochromocytoma or paraganglioma, which increases the difficulty of clinical diagnosis. 2 Therefore, preoperative intensive care is essential to rescue patients experiencing a pheochromocytoma crisis. In the present article, a case of paraganglioma-induced pheochromocytoma crisis treated with veno-arterial (VA)-extracorporeal membrane oxygenation (ECMO), without any complications, is presented, with the aim that the described experience may provide some useful information for the treatment of these patients.
Case report
A woman in her 20s, with a history of hypertension, was brought to the emergency department in July 2022 with sudden onset of palpitations with vomiting for the previous 6 h. On examination, she was alert, tachycardic (138 beats/min), and hypertensive (140/80 mmHg). Emergency chest computed tomography (CT) revealed multiple patchy consolidation grid shadows in both lungs (Figure 1(a)). Abdominal CT revealed a slightly low-density soft tissue mass (measuring 2.9 × 3.1 cm) anterior to the inferior vena cava (Figure 1(b)).

Representative preoperative emergency computed tomography (CT) imaging findings in a female patient in her 20s who presented with sudden-onset palpitations and vomiting: (a) axial plane chest CT showed multiple patchy consolidation grid shadows in both lungs; and (b) axial plane abdominal CT showed a slightly low-density soft tissue mass anterior to the inferior vena cava.
Following CT, the patient’s heart rate was 160 beats/min, respiratory rate was 40 breaths/min and percutaneous oxygen saturation decreased to 61%. She underwent emergency intubation; however, her circulatory failure was worsening, with her blood pressure dropping to 55/31 mmHg despite being administered vasoactive drugs (0.3 µg/kg/min epinephrine and 3 µg/kg/min metaraminol). Key laboratory test results upon initial presentation are shown in Table 1.
Key laboratory test results upon initial presentation of a female patient in her 20s who presented with sudden-onset palpitations and vomiting.

A pheochromocytoma crisis was suspected and the patient was immediately transferred to the intensive care unit (ICU). In the ICU, the patient exhibited paroxysmal hypertension (220/100 mmHg) and hypotension (55/31 mmHg). Pulse indicator continuous cardiac output (PiCCO) hemodynamic monitoring was performed with left femoral artery catheterization. Initial results showed central venous pressure (CVP) 15 mmHg, cardiac index (CI) 2.5 L/min/m2, systemic vascular resistance index (SVRI) 2650 dynes × s × cm–5 × m2, global end diastolic index (GEDI) 700 ml/m2, and extravascular lung water index (EVLWI) 19 ml/kg. The patient’s bedside transthoracic echocardiogram indicated markedly diffuse left ventricular systolic dysfunction with a visual estimated left ventricular ejection fraction (LVEF) of 33%. Despite 100% inspired oxygen, high positive end-expiratory pressure (PEEP; 12 cmH2O), and deep sedation, she continued to be profoundly hypoxemic.
Therefore, VA-ECMO treatment was initiated at 14 h following initial presentation to the emergency department, via an operation in the ICU ward. Catheters were inserted into the left femoral artery (replacing the PiCCO catheter) and the right femoral vein. The diameters of the femoral artery and internal femoral vein catheters were 17 and 21 Fr, respectively (Medtronic, Minneapolis, MN, USA). In addition, a 6F distal perfusion tube was used to improve distal perfusion. The operation took 30 min to complete.
The ECMO parameters were as follows: the flow rate was 3 L/min after ECMO was initially turned on; 3.12 L/min on day 1; 3 L/min on day 2; 3 L/min on day 3; 2.9 L/min on day 4; 2.02 L/min on day 5; 2 L/min on day 6; and 2 L/min on day 7. A heparin mini-pump was used for intravenous anti-coagulation, targeting activated partial thromboplastin time of 40–60 s.
The first blood gas analysis, after establishing ECMO, revealed a lactic acid level of 6.69 mmol/L. At ECMO operation day 1, bedside transthoracic echocardiogram indicated LVEF 27%. The patient’s circulation was improved (blood pressure was 100/65 mmHg with 0.3 μg/kg/min norepinephrine). Ventilator condition was reduced to FiO2 40%, and PEEP was 4 cmH2O. Lactic acid decreased to normal levels the next day. The dose of vasoactive drugs and the ECMO flow rate was gradually reduced over the following few days, and the patient’s hemodynamic parameters gradually stabilized. The patient’s bedside transthoracic echocardiogram indicated LVEF 45% after being on ECMO for 4 days. ECMO was withdrawn 6 days later. The patient was weaned and extubated the next day. Fortunately, she did not experience any complications.
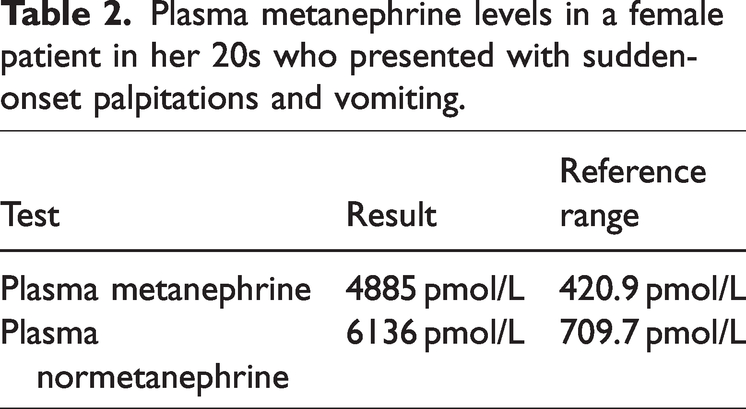
The patient underwent an enhanced CT examination at 9 days following initial presentation, which indicated paraganglioma (Figure 2). Plasma metanephrine levels were elevated more than 8-fold (Table 2), confirming a diagnosis of paraganglioma.

Representative enhanced computed tomography images (left, axial plane; right, coronal plane) in a female patient in her 20s who was treated with veno-arterial extracorporeal membrane oxygenation for suspected pheochromocytoma crisis after presenting with sudden-onset palpitations and vomiting. The blue arrows indicate paraganglioma.
Plasma metanephrine levels in a female patient in her 20s who presented with sudden-onset palpitations and vomiting.
Subsequent 131I-MIBG imaging suggested increased uptake of mid-abdominal radioactivity. Somatostatin receptor imaging showed increased expression between the abdominal aorta and inferior vena cava, consistent with paraganglioma. No lymph node metastasis or remote metastasis was observed, and genetic test results were also normal. The patient underwent laparoscopic surgery 4 months later. Intraoperatively, the tumor was adjacent to the inferior vena cava, abdominal aorta and duodenum. Pathological findings showed that the tumor was 3.5 × 3.5 × 3 cm in size. Histopathological analysis of the specimen confirmed the diagnosis of paraganglioma. The Ki-67 expression level was 5%. The patient’s postoperative course was uneventful and she was discharged 7 days after surgery. A timeline of the clinical condition progress and major management of the patient is summarized in Table 3. Written informed consent to all treatments was obtained from the patient herself or her family members. The study was approved by the Ethics Committee of Beijing Jishuitan Hospital (approval No. K2023-012-00). Informed patient consent to publish was not deemed necessary as all patient details have been de-identified. The reporting of this study conforms to CARE guidelines. 3
The timeline of case progression of a female patient in her 20s who presented with sudden-onset palpitations and vomiting.
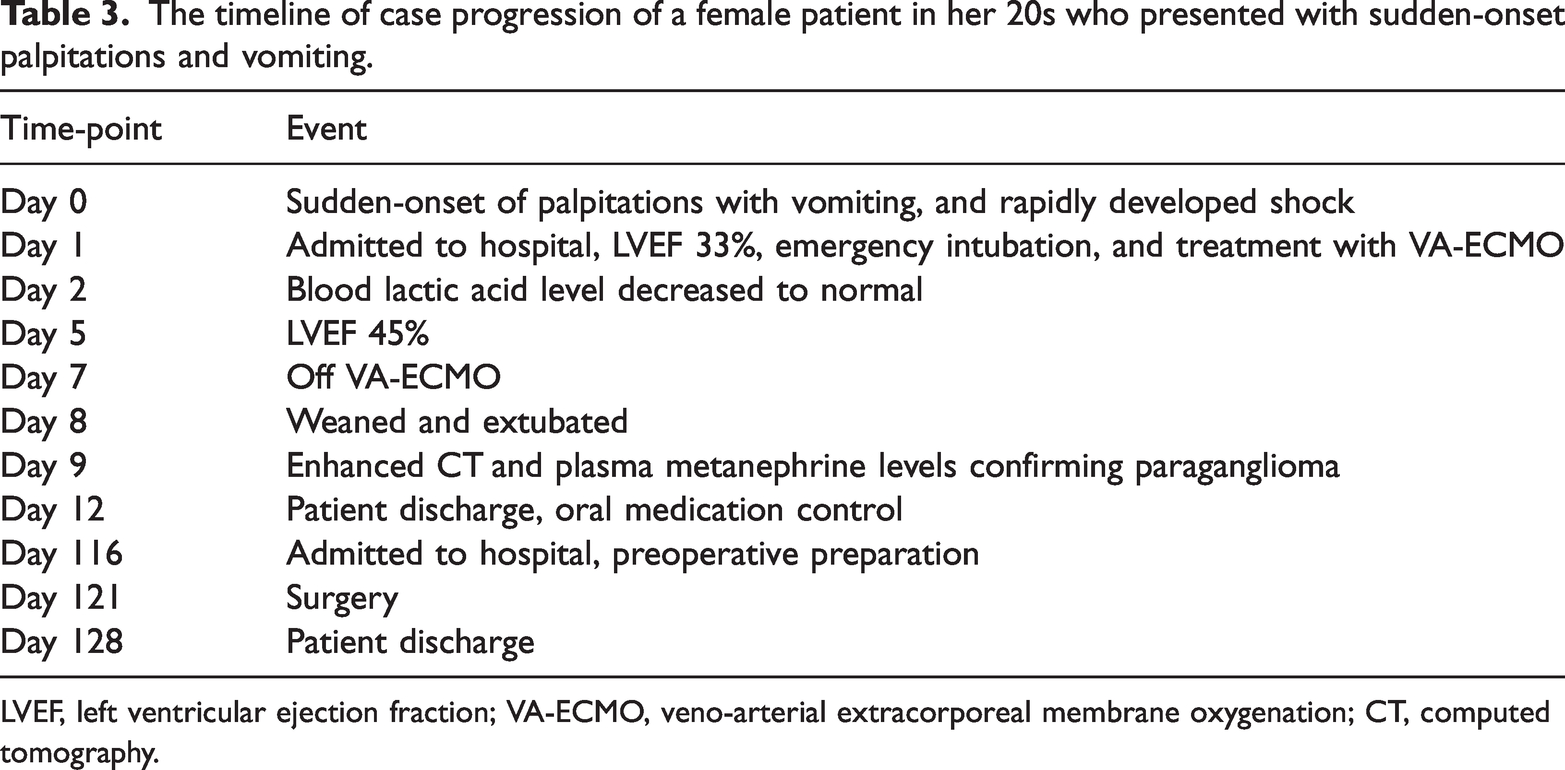
LVEF, left ventricular ejection fraction; VA-ECMO, veno-arterial extracorporeal membrane oxygenation; CT, computed tomography.
Discussion
Pheochromocytoma crisis is rare but potentially fatal if not recognized early and managed properly. 4 In the present study, the case of a female patient who presented with a life-threatening pheochromocytoma crisis, characterized by respiratory and hemodynamic failure due to a paraganglioma, is described. The patient had an acute onset and rapidly progressed to shock refractory to pharmacological treatment. Early diagnosis and treatment are essential to prevent permanent organ damage and save lives, however, the symptoms are often non-specific, raising challenges.
Rapid recent advancements in extracorporeal circulation support technology have led to the development of ECMO, which has been successfully applied in the treatment of pheochromocytoma crisis.2,5 The most common mode is VA-ECMO because it provides full circulatory support and improves tissue oxygenation in situations of cardiogenic shock combined with severe pulmonary edema.6,7 In the present case, VA-ECMO was successfully applied to support the patient through the critical stage of paraganglioma, and she recovered nearly normal myocardial systolic function within 7 days. The present patient was similar to previously reported cases, in that they shared the same clinical characteristics and the same short duration of ECMO support, and most adrenalectomy procedures were delayed after myocardial recovery. 5 As seen in the present case, the reversible nature of the clinical course means that relatively brief exposure to catecholamine leads to striking metabolic abnormalities rather than irreversible necrosis. Rapid reversibility makes severe cardiac dysfunction induced by pheochromocytoma and paraganglioma that is refractory to drug therapy a perfect indication for extracorporeal circulatory support. 8 In such cases, VA-ECMO might be the only way to prevent death. 5
Extracorporeal membrane oxygenation may not only be life-saving, but may also offer clinicians more time for additional diagnostic tests and planning appropriate treatment. The radical treatment of pheochromocytomas and paragangliomas is tumor resection. 1 There is no consensus about the timing of surgery, 9 but for ICU patients with intractable phaeochromocytoma crisis, urgent surgery has been associated with increased morbidity, except in those with hemorrhagic phaeochromocytoma or life-threatening crisis. The present patient underwent multidisciplinary consultation, detailed preoperative preparation, and postoperative ICU care. The tumor was removed several months later and the patient recovered. Hemodynamic stabilization may allow delayed elective tumor resection under more appropriate circulatory conditions and adequate preoperative preparation.
Although ECMO can save lives, there may be several disadvantages and potential adverse events. Complications are common, including bleeding, infection, stroke, renal function damage, leg ischemia and other factors.10,11 In the present case, the patient had a history of hypertension, and attention was paid to precise blood pressure management targets. In addition, a distal perfusion tube was used to improve distal perfusion and avoid lower limb ischemia. It is suggested that ECMO management should be individualized for patients experiencing pheochromocytoma crisis.
Conclusions
The present study reports the case of a patient who presented with a life-threatening pheochromocytoma crisis due to paraganglioma. VA-ECMO was applied to successfully support her through the critical stage and finally radical resection of the tumor was performed. The successful treatment of this patient affirms the importance of ECMO in the clinical management of such cases. Appropriate individual management may contribute to avoiding the occurrence of ECMO complications.
Footnotes
Acknowledgements
The authors wish to acknowledge all those who cared for this patient, including those in Vascular Surgery at Beijing Jishuitan Hospital and Peking Union Medical College Hospital.
Author contributions
Mengqi Tong wrote the manuscript. Hao Wang, Ying Bai, and Shan Wang reviewed, and revised the manuscript. All authors read and approved the final manuscript.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research was supported by funds from the 2023 Guo Jia Lin Chuang Zhong Dian Zhuan Ke Jian She Projects.