
Abstract
Drug overdose can lead to a range of symptoms, including potentially life-threatening cardiac arrhythmias. However, identifying the specific causative drug upon admission can be challenging in many cases. The toxidrome approach is a method that utilizes toxidromes, which are collections of findings obtained from physical examination and ancillary tests, that may be caused by a specific toxin. In this particular case, a man presented with an unknown drug overdose that caused symptoms indicative of anticholinergic effects and abnormal electrocardiogram (ECG) findings. The ECG revealed an R wave in lead aVR, S waves in leads I and aVL, and wide QRS tachycardia with a Brugada pattern. Shortly after arrival, the patient developed cardiac arrest due to a lethal arrhythmia. Prompt initiation of venoarterial extracorporeal cardiopulmonary membrane oxygenation (VA-ECMO) was performed. Fortunately, the patient achieved full neurological recovery, and the overdosed drug was identified as diphenhydramine. When diagnosing and treating drug overdose caused by an unidentified substance, diphenhydramine toxicity should be considered when an anticholinergic toxidrome is present and a Brugada pattern is observed on the ECG. VA-ECMO demonstrates potential as a viable treatment option when initial interventions prove ineffective.
Keywords
Introduction
The number of drug overdose cases has been increasing during the past two decades. 1 Many drugs are available over the counter and easily accessible through online sources without requiring a prescription, leading to a rise in adolescents using over-the-counter (OTC) drugs for suicidal purposes. 2 Because the causative drugs in cases of intoxication are not always recognized in the emergency department (ED), identifying the specific drug and its effects during initial treatment upon admission is challenging in such cases. The toxidrome approach is a method that utilizes toxidromes, which are collections of findings obtained from physical examination and ancillary tests that may be caused by a specific toxin. This approach offers valuable clues to assist the clinician in making an accurate diagnosis. 3
Antihistamine drugs, commonly used for allergies and as sleep aids, can be easily obtained without a prescription. Diphenhydramine, a first-generation H1 receptor antagonist, can cause a variety of symptoms, including anticholinergic effects and cardiac arrhythmias. Notably, a cardiac arrhythmia detected through specific electrocardiogram (ECG) patterns is a life-threatening symptom that can lead to cardiac arrest. 4 Although drug intoxication is typically reversible, venoarterial extracorporeal cardiopulmonary membrane oxygenation (VA-ECMO) may be a beneficial intervention in patients with sustained lethal arrhythmias resulting from drug overdose,5,6 especially when initial treatments such as intravenous sodium bicarbonate are ineffective.
We experienced a case of diphenhydramine overdose in which the cause of cardiac arrest resulting from lethal arrhythmia could not be diagnosed upon hospitalization. The patient required VA-ECMO but ultimately had a favorable outcome. In this report, we emphasize the importance of utilizing the toxidrome approach, in addition to recognizing specific ECG patterns and considering VA-ECMO, in the management of patients with acute intoxication.
Case report
A man in his early 20 s was found lying unconscious and vomiting. Upon arrival of the ambulance, a drug overdose was suspected because he was in possession of a large amount of unidentified white pills within a Tupperware container (Supplementary Figure 1(a)). The tablets were white and cylindrical, with a diameter of 9 mm and height of 3 mm. They had domes with a diameter of 9 mm and height of 0.5 mm attached at the top and bottom (Supplementary Figure 1(b)). The patient and his mother agreed to receive treatment at our hospital. Four minutes before reaching our hospital, he experienced a generalized tonic-clonic seizure. The initial evaluation at the ED revealed a respiratory rate of 33 breaths/minute, heart rate of 133 beats/minute, systemic blood pressure of 92/55 mmHg, no sweating, oxygen saturation of 100% (with oxygen administration at 10 L/minute), and a Glasgow Coma Scale score of 6. The patient had mid-dilated pupils measuring 6 mm in diameter with no light reflex. No signs of injury were found on his body, and his axillary temperature was 36.3°C. Arterial blood gas analysis showed a pH of 6.683, arterial partial pressure of oxygen of 194 torr, arterial partial pressure of carbon dioxide of 152 torr, bicarbonate concentration of 17 mmol/L, lactate concentration of 23 mmol/L, sodium concentration of 152 mmol/L, and potassium concentration of 3.3 mmol/L. Tablets that resembled those shown in Supplementary Figure 1(b) but that had partially dissolved and were about to lose their shape were suctioned from the patient’s nasogastric tube. Subsequent computed tomography revealed high-density areas suggestive of a drug mass within the stomach (Supplementary Figure 2). A urine screening test for drugs and their metabolites was performed using a commercial kit (Triage DOA kit; Sysmex Inc., Kobe, Japan) to investigate acute drug poisoning. This Triage DOA kit is capable of detecting eight drugs with high potential for abuse, including benzodiazepines, cocaine, amphetamine/methamphetamine, methadone, tetrahydrocannabinol, opiates, barbiturates, and tricyclic antidepressants (TCAs), through a qualitative urine immunoassay. However, no drugs were detected in the patient’s urine. A 12-lead ECG revealed wide QRS tachycardia (QRS duration of 250 ms and QTc of 496 ms) with a Brugada pattern, an R wave in lead aVR, and S waves in leads I and aVL, suggesting that the cardiotoxicity was due to drug intoxication (Figure 1). The diagnostic approach in this case, which involved a combination of the toxidrome approach, a urine screening test, and ECG findings, was as follows (Figure 2):
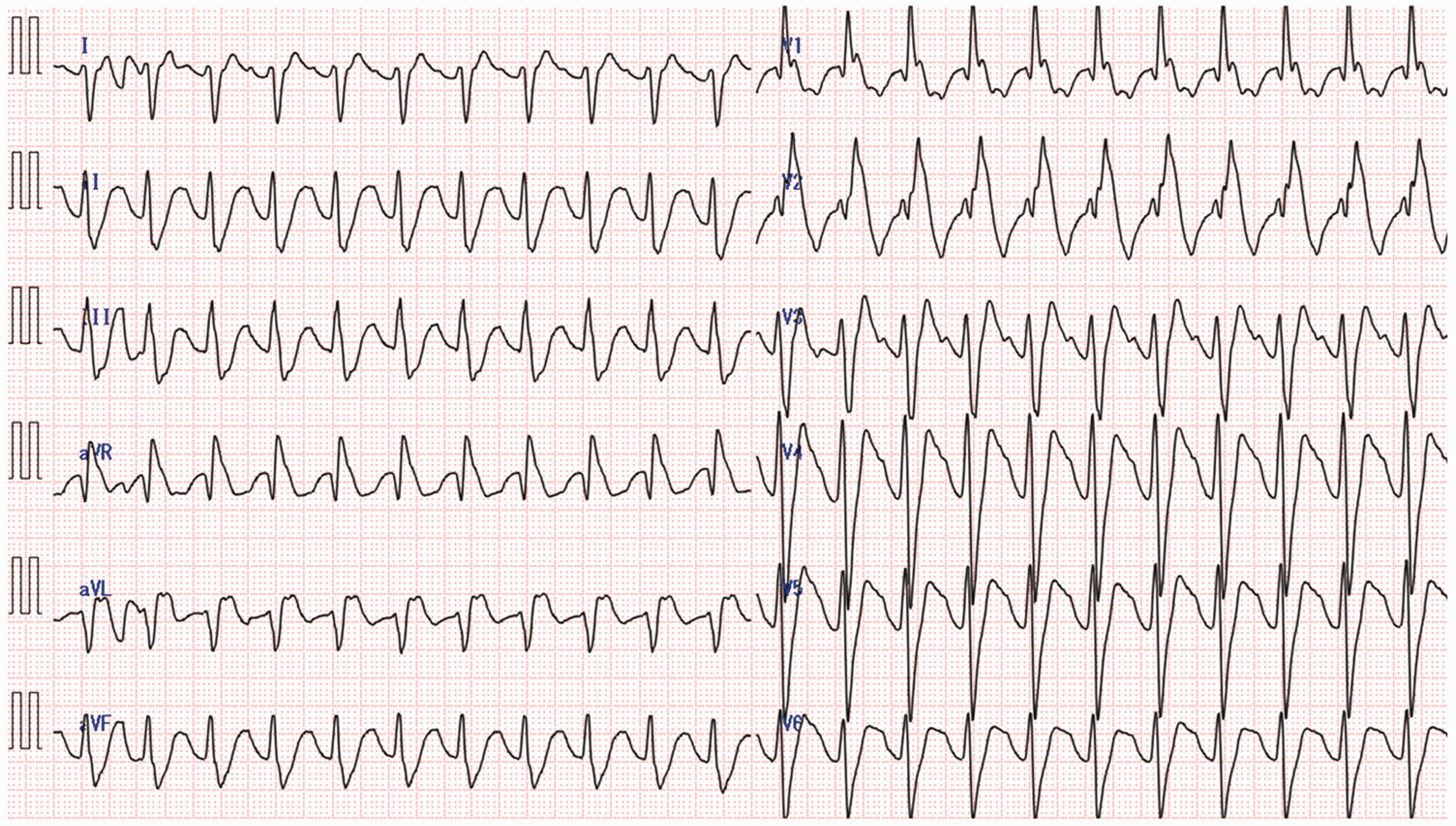
Initial electrocardiogram on arrival of patient with suspected drug overdose. The electrocardiogram revealed marked sinus tachycardia, QRS widening (250 ms) with a Brugada pattern, right axis deviation, a dominant terminal R wave in lead aVR, and QTc prolongation (496 ms). The mechanism of this cardiotoxicity was speculated to involve the blockage of sodium channels on cells in the His-Purkinje system.

Diagnostic approach in this case. The toxidrome suggested an anticholinergic toxidrome, and the Triage DOA kit results were negative. The electrocardiogram showed a Brugada pattern. The drug that matched all three of these approaches was diphenhydramine, which is an over-the-counter drug without an identification code. AMP, amphetamines; BAR, barbiturates; BZO, benzodiazepines; COC, cocaine; OPI, opiates; PCP, phencyclidine; TCA, tricyclic antidepressants; THC, tetrahydrocannabinol.
The patient’s symptoms suggested an anticholinergic toxidrome caused by an overdose of certain drugs such as diphenhydramine, TCAs, or atropine, among others.
The results of the urine screening test were negative, indicating that a TCA was unlikely to be the cause.
The specific ECG findings, such as the Brugada pattern, helped differentiate among diphenhydramine, TCAs, cocaine, and Vaughan Williams I antiarrhythmics.7–10
Upon evaluating all three approaches, the drug that matched the clinical findings was diphenhydramine, which is an OTC drug, and it lacked an identification code. Because of the ongoing hemodynamic instability caused by the cardiac arrhythmia, the patient suddenly developed asystolic cardiac arrest due to the wide QRS tachycardia before receiving sodium bicarbonate. No torsades de pointes ventricular tachycardia was observed during the initial treatments. Cardiopulmonary resuscitation was immediately initiated, and 1 mg of adrenaline was administered twice; however, asystole persisted on the patient’s ECG. Considering the possibility of a transient effect of the cardiac arrhythmia due to drug overdose, we decided to initiate VA-ECMO to provide hemodynamic support. Adequate ECMO flow was achieved within 30 minutes after cardiac arrest. Coronary angiography was performed, but no signs of coronary stenosis were found. Whole-body computed tomography revealed no cerebral hemorrhage, pulmonary embolism, or aortic dissection. The ECG showed a gradual improvement in the axis deviation and conduction abnormalities, and a normal conduction system was restored within 24 hours after intravenous infusion of sodium bicarbonate and VA-ECMO (Figure 3). The patient was successfully weaned off VA-ECMO support at 36 hours after arrival and extubated 1 day later, and his level of consciousness gradually improved. He finally informed us that he had purchased 1000 tablets of an OTC drug called Liposmin (one tablet of which contains 25 mg of diphenhydramine) online and had ingested 161 tablets (equivalent to 4025 mg of diphenhydramine) in a suicide attempt on the day of admission. The patient’s medical history confirmed the overdose of an oral OTC drug, specifically diphenhydramine; therefore, the blood and urine levels of diphenhydramine were not measured. The patient had a good neurological outcome and was discharged from the hospital with outpatient psychiatry follow-up. He provided written informed consent for the publication of this case report, which we prepared following the CARE guidelines. 11 Because this was a case report and written informed consent was obtained for its publication, ethics approval of the study protocol was not needed.
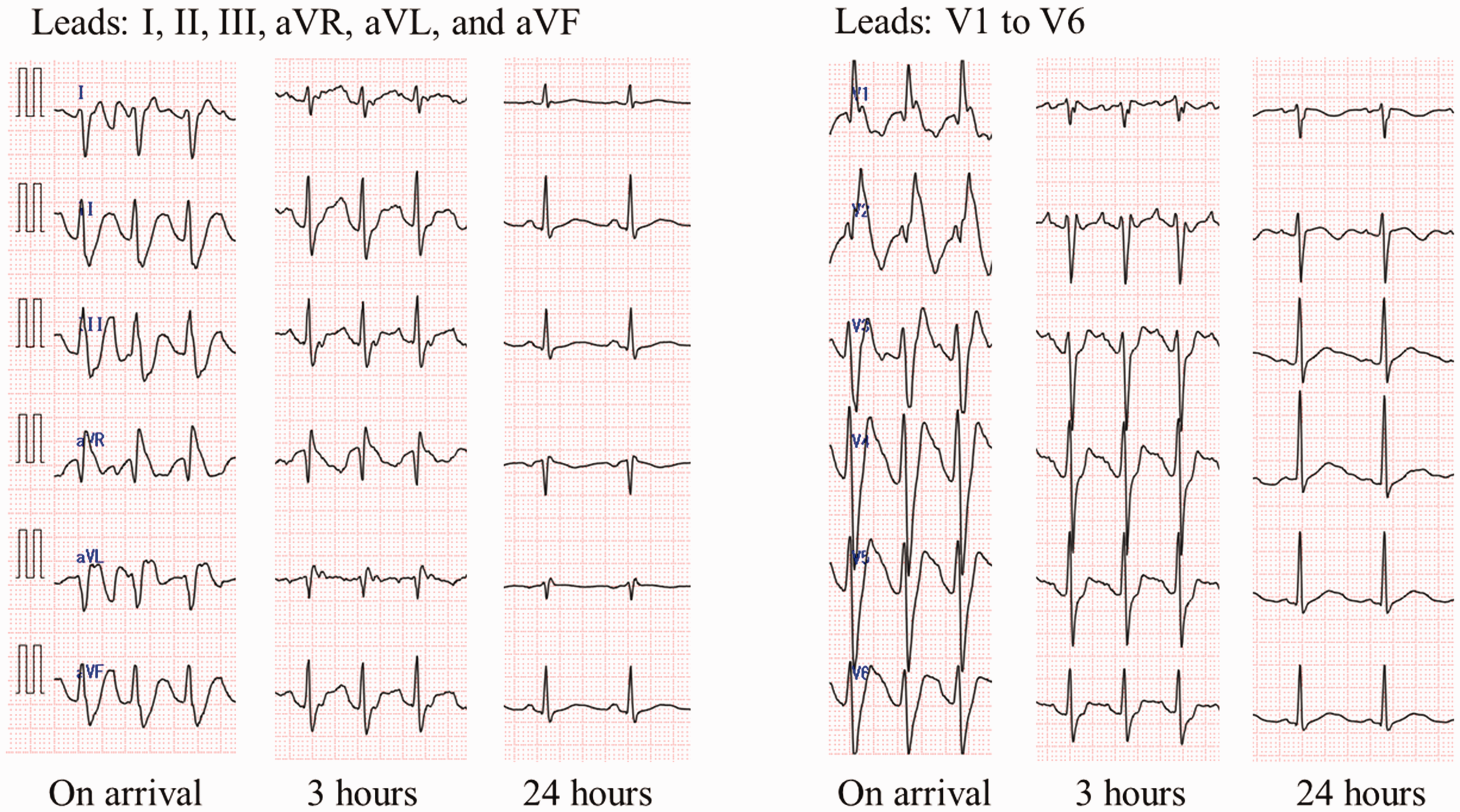
Time series of electrocardiographic changes at arrival, 3 hours later, and 24 hours later. The electrocardiogram indicated sinus rhythm after intravenous infusion of sodium bicarbonate and venoarterial extracorporeal cardiopulmonary membrane oxygenation. The high R wave in lead aVR, axial deviation, and intraventricular conduction delay gradually improved, and the normal conduction system was restored after 24 hours.
Discussion
In an ED setting, emergency physicians often encounter patients with unspecified drug overdoses, and various types of drug intoxication can lead to life-threatening arrhythmias. Upon arrival at our ED, the patient in this case exhibited tachypnea, tachycardia, and mydriasis but no diaphoresis. These symptoms suggested an anticholinergic toxidrome rather than a sympathomimetic toxidrome. 3 Such analysis is known as the toxidrome approach. Although no common global classification has been proposed for the toxidrome approach, toxidromes are often categorized into several types, including excitability, anticholinergic, cholinergic, sedative/hypnotic, opioid, and sympathomimetic toxidromes. Antihistamine drugs, including diphenhydramine, atropine, phenothiazines, anti-Parkinson’s drugs, and TCAs, are commonly used drugs with anticholinergic effects. 12
Diphenhydramine is a widely used OTC drug, but its overdose can be fatal. At a normal dose, diphenhydramine is an antihistamine that is commonly used to treat allergies, insomnia, and motion sickness. Despite being considered a relatively safe drug with a wide therapeutic range, it can cause dose-dependent toxicity. Consuming more than 1.5 g of diphenhydramine further increases the risk of seizures, coma, and death. 4 The therapeutic blood level of diphenhydramine ranges from 25 to 112 ng/mL. 13 Serum diphenhydramine concentrations exceeding 5 µg/mL can be lethal. 14 In this case, although the patient’s diphenhydramine blood level was not assessed during the initial visit, subsequent medical history interviews and information regarding the discovered drugs substantiated that the patient had consumed 161 tablets of Liposmin (equivalent to 4025 mg of diphenhydramine). This strongly indicated the ingestion of a potentially lethal dose. Because of its fat-soluble nature and large volume of distribution, excretion of diphenhydramine through hemodialysis is difficult. Diphenhydramine overdose inhibits sodium channels similarly to Vaughan Williams Ia antiarrhythmic drugs. 15 This inhibition typically manifests as tachycardia (due to anticholinergic effects), QTc prolongation with a terminal R wave in lead aVR, and occasionally a Brugada pattern. 7 Other drug overdoses that can cause a wide QRS and a Brugada pattern include TCAs, cocaine, and antiarrhythmic drugs.8–10 These ECG findings are valuable for distinguishing the specific causative agent. In our case, we were able to deduce that the OTC drug was diphenhydramine at the time of admission by considering the anticholinergic toxidrome, urine screening test, and electrocardiographic findings. Intravenous sodium bicarbonate and lipid emulsion therapy have been reported as viable treatment options in cases of diphenhydramine toxicity. 16 However, VA-ECMO is an appropriate treatment strategy when the patient’s hemodynamics cannot be maintained even with these treatments.5,17
In the ToxIC Registry, ECMO was used in 0.0004% of patients with toxicological exposures, and their survival rate was 80%. 5 Exposures included carbon monoxide/smoke inhalation, bitter almonds, methanol, diphenhydramine, antidepressants, flecainide, verapamil, analgesics, sedative drugs, and antidiabetics. While not all intoxicated patients are candidates for ECMO, ECMO can be a beneficial treatment for drug overdose when accompanied by cardiovascular arrest, sustained hypotension, cardiac arrhythmias, and poor ventilation. Previous reports have indicated favorable outcomes when using ECMO for severe toxicological exposures, particularly with pharmaceuticals such as antiarrhythmic drugs and other cardiovascular medications, diphenhydramine, TCAs, and cocaine.17–21
Conclusion
In the initial treatment of patients with overdose, it can be challenging to determine the specific drug involved. Diphenhydramine poisoning should be considered as a differential diagnosis when symptoms suggest an anticholinergic toxidrome, the absence of drug identification in the urine screening test, and the presence of a Brugada pattern on the ECG. When a lethal cardiac arrhythmia with an anticholinergic toxidrome becomes evident, it is crucial to recognize the risk of cardiac arrest. If the arrhythmia is unresponsive to initial treatments such as intravenous sodium bicarbonate, VA-ECMO holds promise as a viable treatment option.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231205449 - Supplemental material for Diphenhydramine overdose detected early by integration of toxidrome and electrocardiography and treated with venoarterial extracorporeal membrane oxygenation: a case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605231205449 for Diphenhydramine overdose detected early by integration of toxidrome and electrocardiography and treated with venoarterial extracorporeal membrane oxygenation: a case report by Masaru Matsuoka, Riku Arai, Shingo Ihara, Nobuhiro Murata, Junko Yamaguchi, Yasuo Okumura and Kosaku Kinoshita in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605231205449 - Supplemental material for Diphenhydramine overdose detected early by integration of toxidrome and electrocardiography and treated with venoarterial extracorporeal membrane oxygenation: a case report
Supplemental material, sj-pdf-2-imr-10.1177_03000605231205449 for Diphenhydramine overdose detected early by integration of toxidrome and electrocardiography and treated with venoarterial extracorporeal membrane oxygenation: a case report by Masaru Matsuoka, Riku Arai, Shingo Ihara, Nobuhiro Murata, Junko Yamaguchi, Yasuo Okumura and Kosaku Kinoshita in Journal of International Medical Research
Footnotes
Acknowledgements
We thank all the doctors and medical staff who were involved in the treatment of this patient.
Author contributions
M.M. and R.A. contributed to the writing of the case report. All authors were involved in the decision-making process regarding the treatment approach during patient care. R.A., M.M., Y.O., and K.K. engaged in discussions and the literature review while preparing the case report. All authors meet the ICMJE authorship criteria.
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.