
Abstract
The penetration of a peritoneal dialysis catheter into the intestinal cavity is a clinically rare complication. In the present retrospective clinical case series, 11 patients with uraemia who received continuous ambulatory peritoneal dialysis and attended hospital between 2019 and 2023 are described. The median patient age was 61.91 ± 11.33 years. All patients had previously experienced peritoneal dialysis-related peritonitis and were clinically cured by infusing sensitive antibiotics into the abdominal cavity. Colonoscopy was utilised to locate the penetrating catheter and close the perforation with a titanium clip once the catheter had been removed via an external approach. Following a 2–4-week fast, the perforations healed in all 11 patients. The present authors’ experience illustrates that directly removing the catheter and clamping the perforation opening under the guidance of colonoscopy is simple to operate with few complications compared with traditional open surgery.
Keywords
Introduction
According to global data, approximately 11% of patients with end-stage renal disease (ESRD) receive peritoneal dialysis treatment, an important alternative therapy for ESRD, and this number is increasing year by year.1–3 There are many complications related to peritoneal dialysis, but global reports on cases of peritoneal dialysis catheters penetrating the intestinal cavity are rare. Early clinical diagnosis is often difficult, and the cure rate is extremely low. Therefore, patients with uraemia undergoing peritoneal dialysis, in which the peritoneal dialysis catheter had penetrated into the intestinal cavity, were reviewed in the present case series. Furthermore, relevant studies in the published literature were reviewed and are discussed with the aim of improving the clinical understanding and treatment of catheter penetration in peritoneal dialysis.
Patients and methods
The present case series included patients with uraemia who attended 184 Hospital, Yingtan, Jiangxi Province, China for diagnosis, and who had received continuous ambulatory peritoneal dialysis between 2019 and 2023. The database of the hospital dialysis centre was screened for relevant patients. Data regarding history of peritonitis, clinical manifestations, laboratory tests, imaging results, diagnosis and treatment plans of the included patients were extracted from the database.
Approval by the institutional ethics committee was not deemed necessary because the study did not involve human trials or any treatment other than standard hospital care. All patient details were deidentified for this retrospective case series, so informed consent to publish the case data and accompanying images was not required.
In addition to hospital case data, the PubMed and Google Scholar databases were searched for relevant articles published between 1920 and 2023 in English or Chinese, using the keywords: ‘peritoneal dialysis associated peritonitis’, ‘intestinal perforation’, ‘catheter removal’, and ‘titanium clip closure’.
Results
A total of 11 patients with uraemia who underwent continuous ambulatory peritoneal dialysis were included in this case series, comprising six male and five female patients, with a mean age of 61.91 ± 10.65 years (range, 46–76 years), a mean 24-h urine output of 300 ± 250 ml, and a main diagnosis of uraemia and non-continuous bed rest peritoneal dialysis. All patients had experienced peritoneal dialysis-related peritonitis, with nine patients having experience it more than twice. In nine patients, catheters had penetrated the sigmoid colon, and in two patients, catheters had penetrated the rectum (Table 1).
Demographic and clinical characteristics of patients with uraemia who experienced peritoneal dialysis-related peritonitis included in the case series.
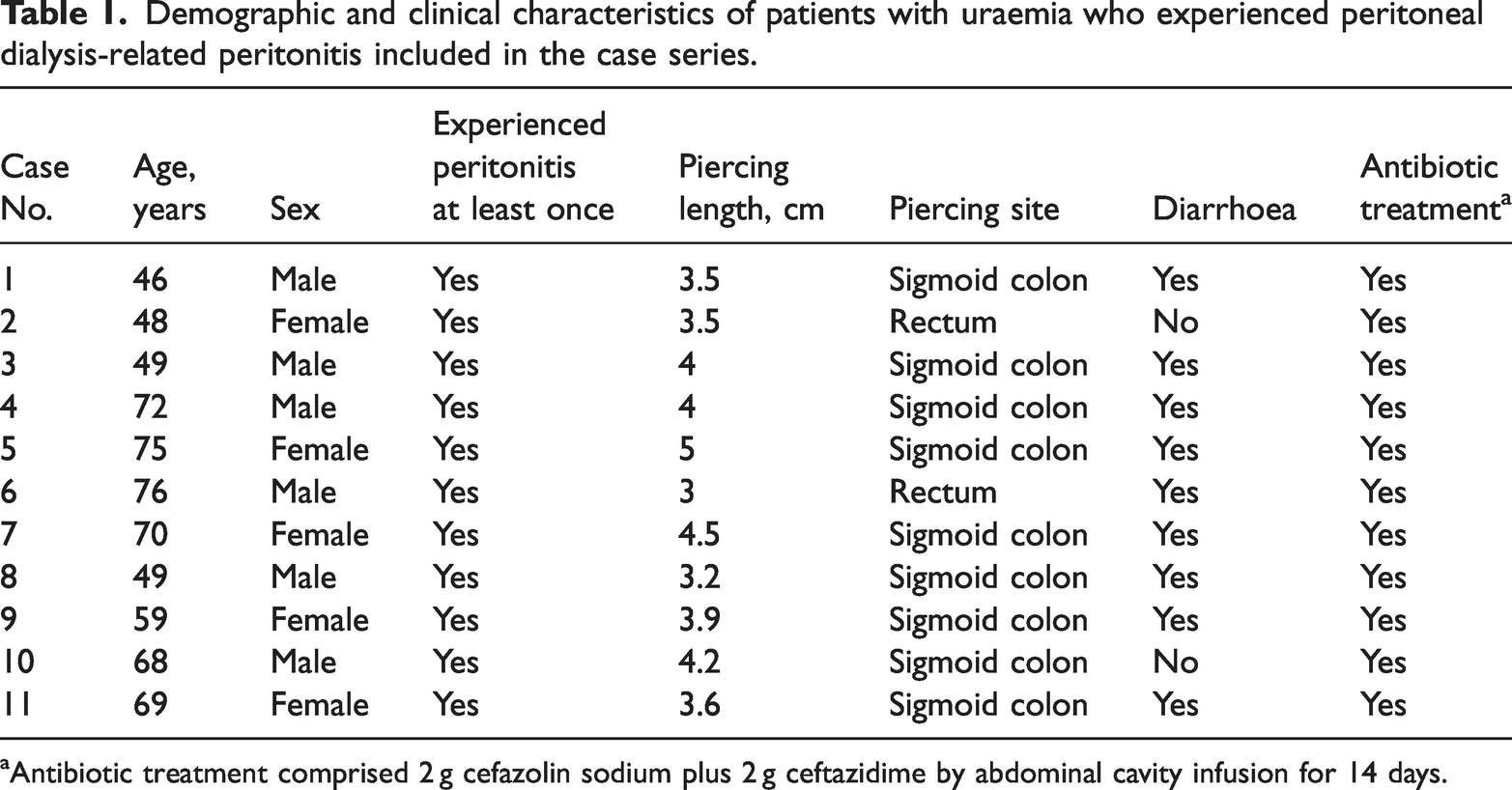
Antibiotic treatment comprised 2 g cefazolin sodium plus 2 g ceftazidime by abdominal cavity infusion for 14 days.
Of the 11 included patients, all had experienced catheter perforation into the intestinal tract during peritoneal dialysis. The patients had symptoms of abdominal pain, primarily across the entire abdomen, presenting as persistent distension and pain. The drained dialysis fluid was turbid, and laboratory tests on the drained dialysate showed a white blood cell count greater than 0.1 × 109/L and a neutrophil ratio greater than 50%. After intraperitoneal antibiotic infusion, the symptoms of abdominal pain and related test results returned to normal in all patients. Intestinal perforation caused by peritoneal catheters is a rare but severe complication with a high mortality rate. 4 Diagnosis is difficult, because early symptoms and signs are similar to peritoneal dialysis-associated peritonitis, and lack specific typical symptoms. Early diagnosis via symptoms and radiological imaging is also difficult,4,5 but perforation may be detected through endoscopic methods.6,7 Contrast media was used to assess the 11 patients in the present case series. After infusing contrast agent through the peritoneal dialysis fluid, a CT scan was immediately performed, which confirmed the presence of contrast agent in the intestinal tract. (Figure 1). After an abdominal dialysis catheter penetrates the intestinal cavity, there is inflammation and exudation in the abdominal cavity, which can easily cause intestinal adhesions. Conventional surgery for repairing intestinal perforation carries a higher risk and often results in poor outcomes.
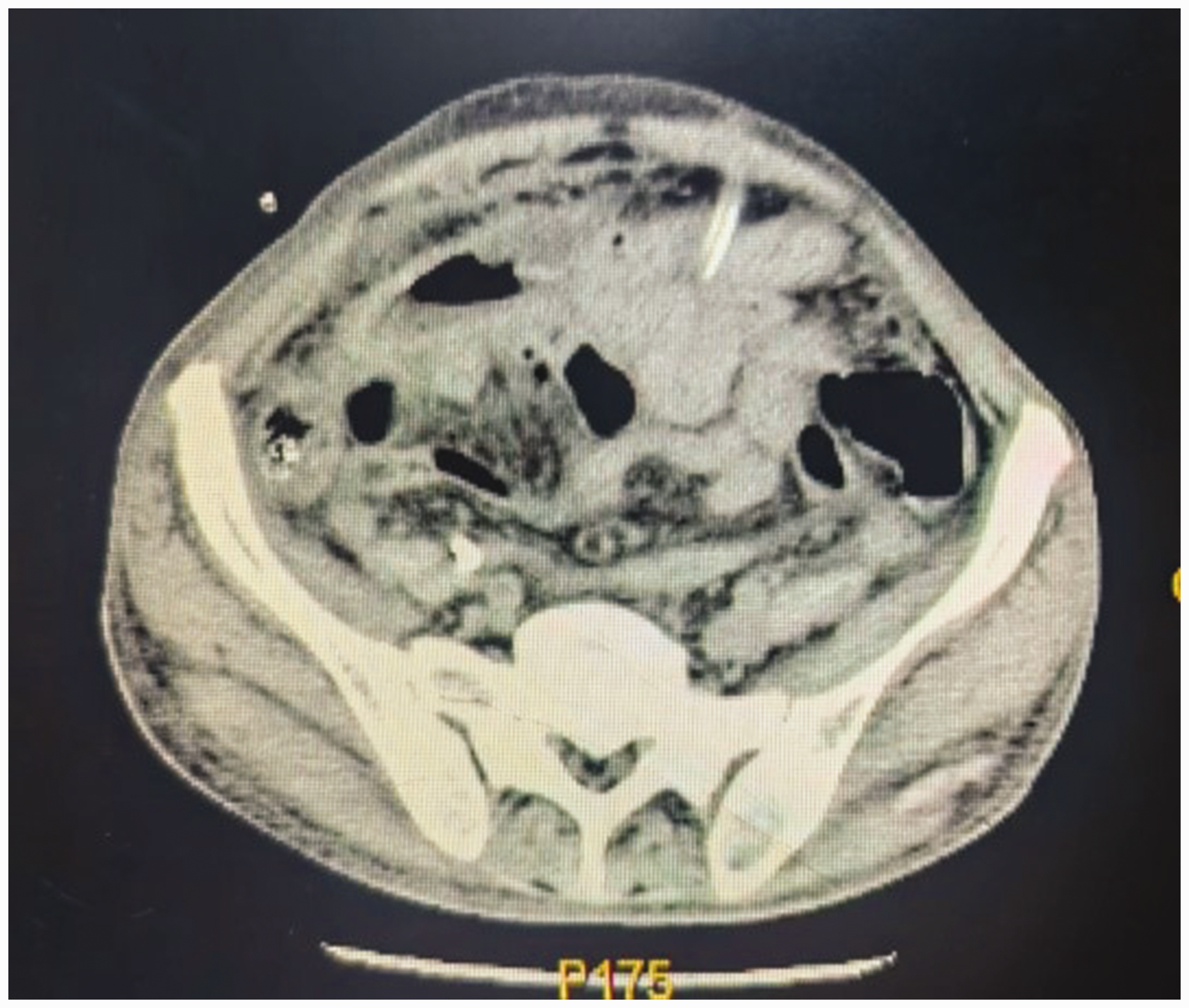
Representative abdominal computed tomography scan image (axial plane) confirming the position of the peritoneal dialysis catheter in a patient with uraemia who experienced peritoneal dialysis-related peritonitis.
Among the 11 cases in the present series, whose peritoneal dialysis catheters had penetrated into the intestinal cavity, the site of catheter penetration into the intestinal tract was located through colonoscopy. Once located, a relatively fast, simple, effective, and minimally invasive manual method was adopted for removing the peritoneal dialysis catheter from the outside, as previously described, 8 while immediately closing the intestinal perforation with a metal titanium clip (Figures 2 and 3), according to a previously published method. 9
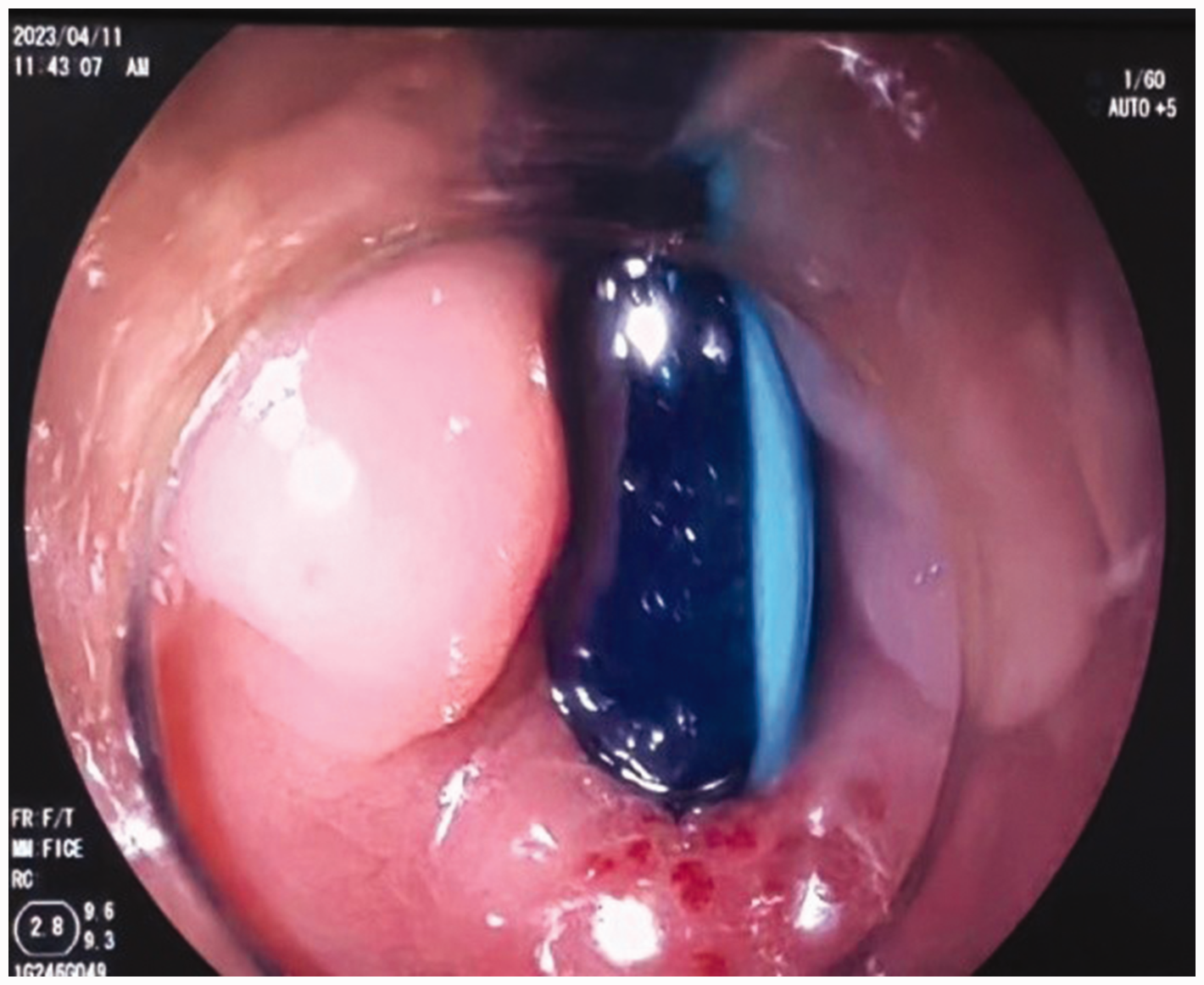
Representative colonoscopy image revealing the peritoneal dialysis catheter and the perforation site in a patient with uraemia who experienced peritoneal dialysis-related peritonitis.

Representative colonoscopy image showing titanium clips used to close the dialysis catheter perforation site in a patient with uraemia who experienced peritoneal dialysis-related peritonitis.
Following treatment, the 11 patients were fasted for 2–4 weeks. In seven cases, the titanium clips fell off between 14 and 18 days after fasting, and in four cases, the clips fell off between 22 and 28 days after fasting. All clips were excreted from the intestine, and all patients underwent follow-up colonoscopy on the next day, showing that the perforation had healed.
Discussion
At present, there are few reports on cases of peritoneal dialysis causing abdominal dialysis catheters to penetrate the intestine. Early diagnosis is difficult, and the cure rate is extremely low. 10 The incidence of intestinal perforation is reported to be 0.1%, but its complications are usually serious, often due to other factors, such as intestinal tumours, acute and chronic enteritis, and mesenteric ischemic diseases.11–13 Penetration of a peritoneal dialysis catheter into the intestinal cavity in patients with peritoneal dialysis may be related to the occurrence of bacterial or fungal peritonitis caused by repeated abdominal infections. In addition, factors such as high abdominal pressure, improper placement of the catheter, formation of an abdominal sinus tract and intestinal adhesions, prolonged indwelling of the catheter, and repeated rubbing of the catheter against the intestinal wall,14–16 increase the risk of the peritoneal dialysis catheter penetrating the intestinal cavity. According to the published literature,17–19 a paediatric patient was reported with the peritoneal dialysis catheter visibly protruding from the anus. Abdominal X-ray showed no free air, and a small perforation of the sigmoid colon was visualized by laparoscopy. The perforation was effectively repaired and the catheter was removed simultaneously, but the procedure caused significant trauma. However, in recent years, the introduction of new devices has improved the success rate of endoscopic closure of intestinal perforations. The over-the-scope clip is a nitinol clip that resembles a ‘trap’ in shape and can grasp more tissue than traditional clips, allowing for the closure of larger perforations, and metal titanium clips have been successfully used to close perforations in the duodenum and colon.20–22 Peritoneal dialysis-associated peritonitis has an adverse effect on the abdominal cavity and intestinal tract and is also an important factor causing the peritoneal dialysis catheter to penetrate into the intestinal cavity. There is a persistent micro inflammatory state in the body of patients with ESRD, and peritoneal dialysis-associated peritonitis is the most common associated infection.23,24 The incidence of peritoneal dialysis-associated peritonitis is reported to be 0.06–1.66 times/patient/year in China, and 0.14–0.17 times/patient/year worldwide, with a cure rate of only 90%.25–27 Serious complications of peritoneal dialysis may also cause adhesions in the abdominal sinus and intestinal tract, encapsulated peritoneal fibrosis or sclerosing encapsulated peritonitis.28–30 Common causes of peritoneal dialysis-associated peritonitis include advanced age, adjuvant peritoneal dialysis, higher body mass index, low serum albumin, intestinal infection, and improper peritoneal dialysis procedures. Intestinal infections may easily cause inflammation and exudation of the intestinal wall, thickening or thinning of the intestinal wall, and intestinal adhesions. In addition, the metabolic products of bacteria (such as p-cresol, trimethylamine, and H2S) affect the structure and function of the intestinal barrier,31–33 and also the structure and function of the intestinal epithelial cell barrier.34,35 At the same time, chronic kidney disease affects the metabolism of colonic microorganisms. 36 The greater omentum of the abdominal cavity may wrap around the fixed peritoneal dialysis catheter, and with other factors mentioned above, may cause the peritoneal dialysis catheter to penetrate the adjacent intestinal cavity. This incidence rate is rare, but often serious.
In summary, the main complications of peritoneal dialysis are infection-related, followed by mechanical-related complications. Peritoneal dialysis catheter-related visceral injuries are uncommon, with intestinal or bladder perforations being the primary concerns, and intestinal perforations can be catheter-related or delayed. The incidence of catheter-related intestinal perforation is relatively low, at <1%, 37 with common causes being the blind insertion of catheters using trocars during catheter placement or performing other procedures (such as omentopexy or adhesiolysis) at the same time as the catheterization in the presence of abdominal adhesions. Risk factors for delayed intestinal perforation include cessation of peritoneal dialysis treatment for >1 month without regular lavage, diverticular inflammation of the intestines, systemic amyloidosis involving the intestines, or peritonitis.19,38 Intestinal perforation during the catheterization process is often difficult to detect, leading to delayed intestinal perforation. If faecal odour is detected during the catheterization process, intestinal perforation should be considered; clinical manifestations of delayed intestinal perforation include severe watery diarrhoea (caused by catheter insertion into the intestinal lumen), abdominal muscle tension, abdominal pain, hypotension, and the catheter tip protruding from the anus. Patients with ESRD often have low immune function and are in a micro-inflammatory state. When peritoneal dialysis-associated peritonitis occurs, the intestinal flora is disordered, and the structure and function of the epithelial cell barrier are damaged, making the intestines more prone to adhesion or obstruction. The greater omentum in the abdominal cavity may wrap around and fix the peritoneal dialysis catheter. If the peritoneal dialysis catheter remains in the abdomen for an extended period, with its tip closely pressed against the intestinal wall and under significant abdominal pressure, the catheter can easily penetrate the weaker parts of the intestinal wall. Some perforations caused by catheters are asymptomatic due to the growth of granulation tissue around the catheter, which prevents intestinal faeces or bacteria from entering the abdominal cavity. This condition is known as asymptomatic intestinal perforation and is relatively rare. The external diameter of the peritoneal dialysis catheter is approximately 7 mm. If the catheter is removed with a temporary halt of peritoneal dialysis, as well as fasting and waiting for the perforation to heal itself without repairing the intestinal perforation site, the process may take longer and be more difficult to heal due to a lowered immune system in patients with uraemia. There is significant individual variation in this process, however, once a peritoneal dialysis patient experiences an intestinal perforation caused by the catheter, whether it was mistakenly inserted into the intestinal tract during placement or the perforation was related to previous peritonitis or intestinal diseases, failure to address the issue promptly will affect the efficiency of dialysis.
Conclusion
Intestinal perforation caused by a peritoneal dialysis catheter may be diagnosed by examination of the drained peritoneal dialysate composition and abdominal CT scans. As patients with peritoneal dialysis often have intestinal adhesions, it may be difficult to locate the perforation site and safely separate adjacent intestinal tubes using conventional surgical laparotomy. In such cases, fasting to empty the intestines and using an external manual method to remove the peritoneal dialysis catheter, while closing the perforation site with a titanium clip under colonoscopy guidance, might be a treatment method worthy of clinical promotion.
Footnotes
Acknowledgements
The successful completion of this study could not have been achieved without the help and support of many individuals. The authors are grateful to all members of the laboratory who provided substantial assistance during the experiments.
Author contributions
All authors read and approved the final manuscript.
Study design: XX, FH; Literature search: XX, FH, XT; Manuscript preparation: XX, FH, XT, MW, RW.
Data accessibility statement
The data supporting the findings of this study are available within the article.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.