
Abstract
Objective
To analyze the predictive value of the triglyceride-glucose (TyG) index and neutrophil-to-high-density lipoprotein ratio (NHR) for in-hospital major adverse cardiac events (MACE) after percutaneous coronary intervention (PCI) in patients with acute ST-segment elevation myocardial infarction (STEMI), and to establish an associated nomogram model.
Methods
In this retrospective study, we collected data from consecutive STEMI patients who underwent PCI from October 2019 to June 2023 at the Second People’s Hospital of Hefei and the Second Affiliated Hospital of Anhui Medical University, as training and validation sets. Stepwise regression and multivariate logistic regression analysis were performed to screen independent risk factors, and a nomogram model was constructed and evaluated for its predictive efficacy.
Results
The TyG index, NHR, urea, diastolic blood pressure, hypertension, and left ventricular ejection fraction were independent risk factors for in-hospital MACE after PCI, and were used to construct the nomogram model. The C-index of the training and validation sets were 0.799 and 0.753, respectively, suggesting that the model discriminated well. Calibration and clinical decision curves also demonstrated that the nomogram model had good predictive power.
Conclusion
In STEMI patients, increased TyG index and NHR were closely related to the occurrence of in-hospital MACE after PCI. Our constructed nomogram model has some value for predicting the occurrence of in-hospital MACE in STEMI patients.
Keywords
Introduction
Acute ST-segment elevation myocardial infarction (STEMI) is characterized by an acute onset, rapid progression, and poor prognosis. Percutaneous coronary intervention (PCI) is usually the primary strategy for its treatment. 1 The inflammatory response and abnormal lipid metabolism are thought to play an essential role in the formation and rupture of atherosclerotic plaques, which are also the main pathophysiological mechanisms in the development of STEMI.2,3
Insulin resistance is a risk factor for coronary atherosclerosis; it leads to abnormal metabolic pathways for nutrients, including blood lipids and glucose, by reducing sensitivity to insulin’s metabolic effects. In addition, insulin resistance promotes the development of atherosclerosis by triggering pathological conditions such as inflammation, vasoconstriction, and thrombosis.4,5 Several studies have demonstrated that the serum triglyceride-glucose (TyG) index is significantly correlated with results from the gold-standard test for insulin resistance (the hyperinsulinemic euglycemic clamp test), and its simple and economically accessible advantage makes its clinical application more effective. 6 Recent studies7,8 have shown that TyG index levels are associated with arterial plaque characteristics and long-term prognosis in STEMI patients, thus providing medical evidence that the TyG index may be used as a risk stratification indicator in STEMI patients; however, no studies have explored the correlation between this index and short-term prognosis in STEMI patients.
Chronic inflammation and abnormal lipid metabolism play a crucial role in the pathophysiology of atherosclerosis, leading to adverse cardiovascular events and death. 9 As pro-inflammatory cells, neutrophils have recently been implicated in various stages of atherosclerosis, which can aggravate endothelial dysfunction. Monocytes are recruited into atherosclerotic lesions, activating macrophages and promoting foam cell formation, whereas neutrophils can lead to plaque instability. Neutrophils are also the first cells to respond when acute myocardial infarction occurs. Furthermore, they are essential cells for inflammatory infiltration and the removal of necrotic tissue during myocardial infarction.
In contrast to neutrophils, high-density lipoprotein cholesterol (HDL-C) is considered a protective factor against atherosclerosis. Its main cardioprotective mechanisms include reverse cholesterol transport, antioxidant properties, and anti-inflammatory effects in endothelial cells. 10 Previous epidemiological studies have demonstrated that HDL-C is a significant predictor of both mortality and cardiovascular mortality in patients with myocardial infarction. 11 The neutrophil-to-high-density lipoprotein ratio (NHR) is the ratio of neutrophils to high-density lipoprotein; this index reflects the collective inflammatory response and blood lipid metabolism level, and is recognized by the majority of cardiovascular researchers.
Few studies have explored the value of the TyG index combined with the NHR for predicting in-hospital major adverse cardiac events (MACE) after PCI in STEMI patients. The aim of the present study was therefore to investigate the correlation between the combined TyG index and NHR and in-hospital MACE after PCI in STEMI patients. We also aimed to clarify the value of a nomogram model, established using the combined TyG index and NHR, for predicting in-hospital MACE after PCI in STEMI patients, to provide new ideas for clinical prognostic risk stratification in STEMI patients.
Materials and methods
Study population
We conducted a retrospective study of consecutive STEMI patients who underwent emergency PCI at the Second People’s Hospital of Hefei from October 2019 to June 2023, as the training set. Simultaneously, we also collected data from STEMI patients who underwent PCI in the Emergency Department of the Second Affiliated Hospital of Anhui Medical University, as the validation set (to evaluate the value of the model). All patient details were de-identified. The inclusion criteria were as follows: (1) met the diagnosis and treatment criteria of acute myocardial infarction; 12 (2) had myocardial infarction as the first attack; (3) were aged >18 years old; and (4) had complete clinical data. The exclusion criteria were as follows: (1) had a previous myocardial infarction; (2) had severe metabolic system diseases; (3) had severe liver, kidney, or other organ dysfunction; (4) had a severe infection; (5) had coagulation dysfunction; or (6) had cardiac adverse events before the detection of fasting blood glucose and triglyceride levels. For MACE, we defined the primary endpoint as cardiac death; the secondary endpoints were myocardial reinfarction, malignant arrhythmia, and severe acute heart failure. A diagnosis of acute heart failure was dependent on the following: clinical manifestations such as shortness of breath, orthopnea, pulmonary rales, or pink foamy sputum; N-terminal pro b-type natriuretic peptide >450 ng/L in patients ≤50 years old, >900 ng/L in patients >50 years old, >1800 ng/L in patients >75 years old, and >1200 ng/L in patients with renal insufficiency (glomerular filtration rate <60 mL/minute). Malignant arrhythmias included severe sinus bradycardia (≤40 beats/minute), high-grade or third-degree atrioventricular block, ventricular tachycardia, and ventricular fibrillation; cardiac arrest was classified as a special type of malignant arrhythmia. The present study was a retrospective study; it was granted ethical exemption from the Ethics Committee of the Second People’s Hospital of Hefei and the Second Affiliated Hospital of Anhui Medical University, and informed consent was not required for any patients. The reporting of this study conforms to Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 13 The study flowchart is shown in Figure 1.
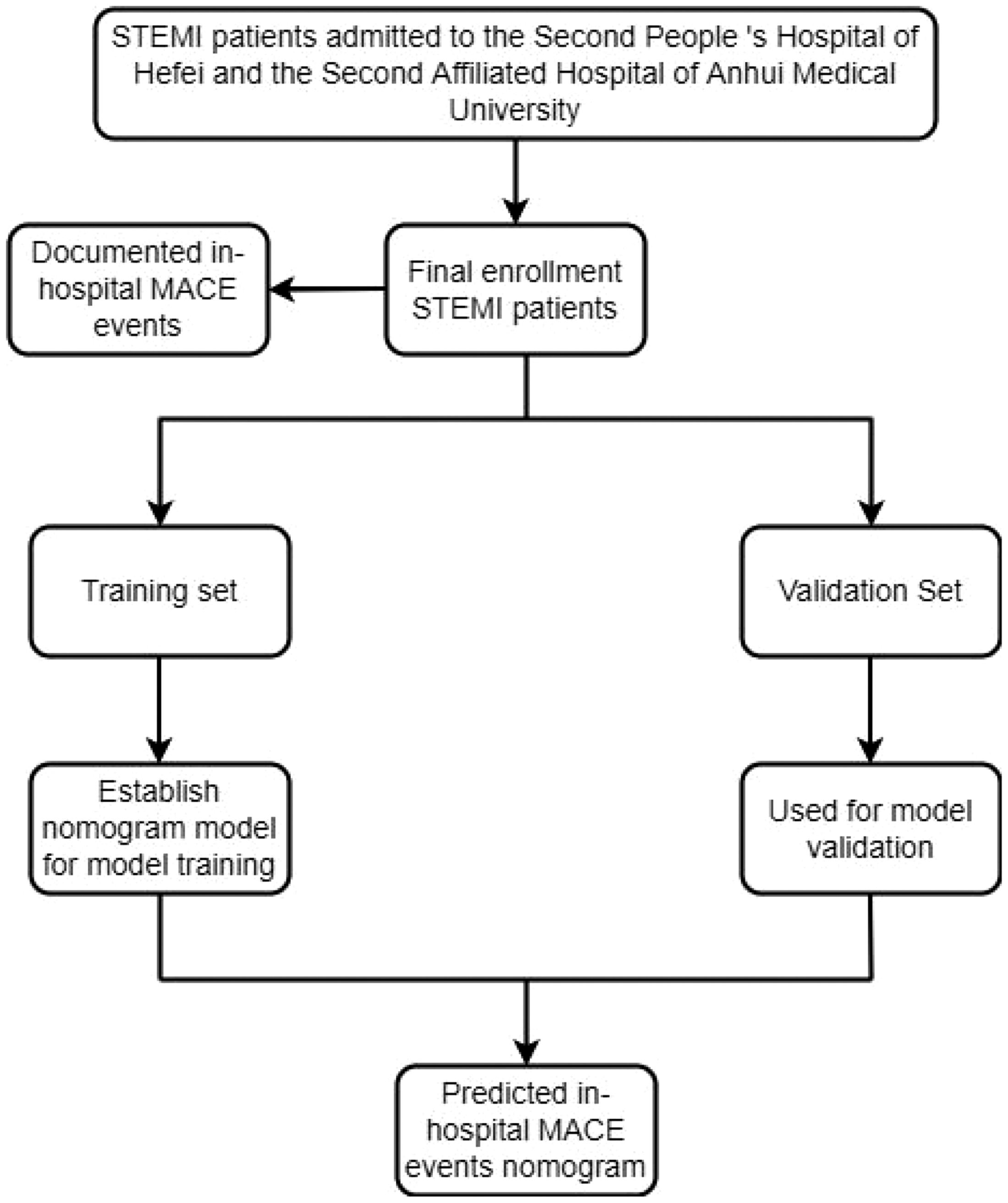
Study flowchart.
Study methods
Data collection
Demographic characteristics and clinical data at admission were collected from STEMI patients through a hospital electronic medical record system. These data included age, sex, body mass index, smoking status, hypertension, diabetes, systolic blood pressure, diastolic blood pressure (DBP), lymphocytes, monocytes, red blood cells, hemoglobin, platelets, glycosylated hemoglobin, albumin, urea, creatinine, uric acid, direct bilirubin, indirect bilirubin, total cholesterol, low-density lipoprotein cholesterol, left ventricular ejection fraction (LVEF), TyG index (calculated as fasting triglyceride [mg/dL] × fasting glucose [mg/dL]/2), and NHR.
Nomogram establishment and verification
The stepwise regression backward method and multivariate logistic regression were used to analyze the independent factors influencing MACE after PCI in STEMI patients. Predictive nomogram models were constructed using the predictors, and C-index and receiver operating characteristic (ROC) curves were plotted to assess the efficacy of the models for predicting the risk of MACE after PCI in STEMI patients. Model fit was evaluated using the Hosmer–Lemeshow test, and model calibration was assessed using the Brier score. The calibration and clinical decision curves were then drawn; the clinical decision curve was used to analyze the net benefit rate of the nomogram model for predicting MACE after PCI in STEMI patients.
Statistical methods
Statistical analysis and plotting were performed using IBM SPSS Statistics for Windows, version 26.0 (IBM Corp., Armonk, NY, USA), and R, version 4.2.1 (www.r-project.org). Independent sample t-tests were used to compare measurement data between the two groups. The enumeration data adoption rate was expressed, and the chi-squared test was used to compare the two groups. Furthermore, the stepwise regression backward method and multivariate logistic regression were used to analyze the independent risk factors affecting MACE after PCI in STEMI patients. The random forest algorithm was also used to rank the importance of variables. Finally, the C-index, area under the ROC curve (AUC), calibration curve, and clinical decision curve were calculated. All analyses were performed using two-sided tests, and P < 0.05 was considered significant.
Results
Comparisons of baseline data and laboratory test indicators between the training and validation sets
There were 398 training sets from STEMI patients; 112 (28.14%) developed in-hospital MACE after PCI. There were 253 validation sets from STEMI patients; 75 (29.64%) developed in-hospital MACE after PCI. There were significant differences in red blood cells, hemoglobin, albumin, and total cholesterol indexes between the training and validation sets (P < 0.05); there were no significant differences in any other indexes (Table 1).
Comparison of baseline data and laboratory parameters between the training and validation sets in patients with ST-segment elevation myocardial infarction.

All values are provided as the mean ± standard deviation unless otherwise indicated; *P < 0.05.
BMI, body mass index; DBP, diastolic blood pressure; LDL-C, low-density lipoprotein C; LVEF, left ventricular ejection fraction; NHR, neutrophil-to-high-density lipoprotein ratio; SBP, systolic blood pressure; TyG, triglyceride-glucose index.
Baseline data and laboratory parameters of in-hospital MACE after emergency PCI in STEMI patients in the training set
There were significant differences in age, diabetes, hypertension, systolic blood pressure, DBP, monocytes, glycosylated hemoglobin, urea, creatinine, uric acid, albumin, indirect bilirubin, LVEF, NHR, and TyG index levels between the MACE and non-MACE groups in the training set (P < 0.05); there were no significant differences in any other indicators (Table 2).
Comparison of baseline data and laboratory parameters between the MACE and non-MACE groups after emergency percutaneous coronary intervention in patients with ST-segment elevation myocardial infarction in the training set.

All values are provided as the mean ± standard deviation unless otherwise indicated; *P < 0.05.
BMI, body mass index; DBP, diastolic blood pressure; LDL-C, low-density lipoprotein C; LVEF, left ventricular ejection fraction; MACE, major adverse cardiac events; NHR, neutrophil-to-high-density lipoprotein ratio; SBP, systolic blood pressure; TyG, triglyceride-glucose index.
Construction and validation of a risk prediction model for in-hospital MACE after PCI in STEMI patients
Analysis of risk factors for in-hospital MACE after emergency PCI for STEMI
Factors with significant differences in Table 2 were used as independent variables. Stepwise regression was performed using STEMI patients with or without in-hospital MACE after PCI as dependent variables for variable screening. Finally, seven important variables—uric acid, hypertension, NHR, DBP, urea, LVEF, and TyG—were selected. Using the significant variables screened by stepwise regression as independent variables, we included whether patients developed in-hospital MACE after PCI as the dependent variable in the multivariate logistic regression analysis. The NHR (odds ratio [OR]: 1.119, 95% confidence interval [CI]: 1.044–1.2), TyG index (OR: 2.494, 95% CI: 1.655–3.757), hypertension (OR: 0.451, 95% CI: 0.259–0.787), DBP (OR: 0.97, 95% CI: 0.953–0.988), urea (OR: 1.286, 95% CI: 1.152–1.436), and LVEF (OR: 0.962, 95% CI: 0.94–0.985) were all independent risk factors for in-hospital MACE after PCI in STEMI patients (P < 0.05; Figure 2). The random forest algorithm revealed that the TyG index and NHR were crucial independent risk factors that affected MACE after PCI in STEMI patients (Figure 3).
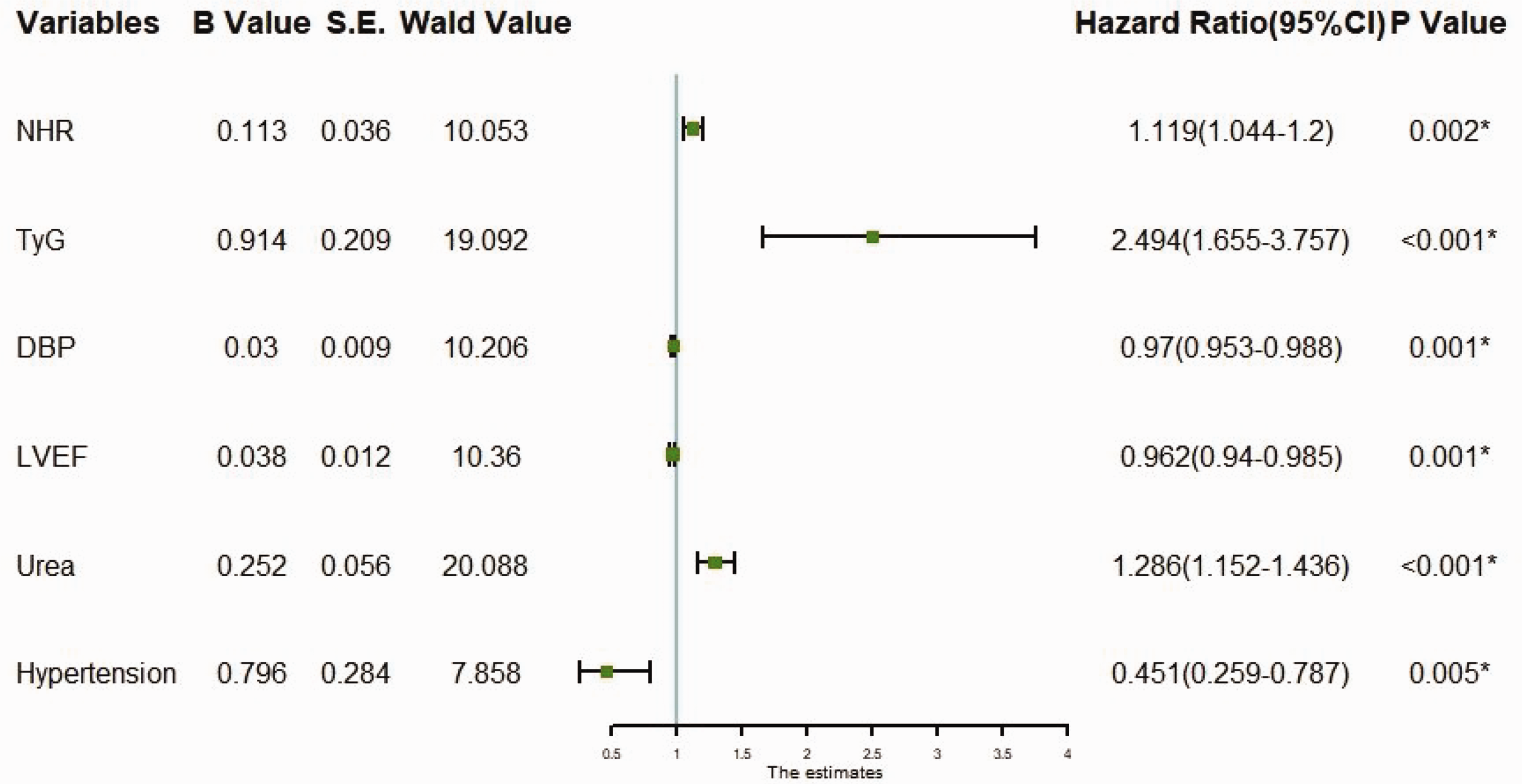
Forest plot for multivariate logistic regression analysis. DBP, diastolic blood pressure; LVEF, left ventricular ejection fraction; NHR, neutrophil-to-high-density lipoprotein ratio; TyG, triglyceride-glucose index.

Random forest variable importance ranking. DBP, diastolic blood pressure; LVEF, left ventricular ejection fraction; NHR, neutrophil-to-high-density lipoprotein ratio; TyG, triglyceride-glucose index.
Establishment of the nomogram model
A nomogram of the predictive model for in-hospital MACE after emergency PCI in STEMI patients according to the independent risk factors is presented in Figure 4. Each predictor variable corresponds to a specific score on the horizontal axis of the nomogram score, and the scores corresponding to the six predictor variables are summed to obtain a total score. The total score (corresponding to the prediction value of the risk of in-hospital MACE, shown at the bottom of the nomogram) demonstrated that patients with higher total scores were more likely to have in-hospital MACE.

Nomogram of in-hospital major adverse cardiac events after percutaneous coronary intervention in patients with ST-segment elevation myocardial infarction. DBP, diastolic blood pressure; LVEF, left ventricular ejection fraction; NHR, neutrophil-to-high-density lipoprotein ratio; TyG, triglyceride-glucose index; *P < 0.05.
Validation of the nomogram model
The C-index of the training set was 0.799 (95% CI: 0.746–0.852) and that of the validation set was 0.753 (95% CI: 0.691–0.815), suggesting good model discrimination. The AUC of the training set was 0.799 (95% CI: 0.746–0.852) and that of the validation set was 0.753 (95% CI: 0.691–0.815), suggesting good model accuracy (Figure 5). The Hosmer–Lemeshow goodness-of-fit test revealed that the nomogram model fitted well (χ2 = 2.501, P = 0.2864). Furthermore, the Brier score was 0.18, and the results of the calibration curve analysis demonstrated that the calibration curve of the nomogram model for predicting in-hospital MACE after PCI in STEMI patients was close to the ideal curve in the training and validation sets (Figure 6). In addition, clinical decision curve analysis revealed that the nomogram model provided additional clinical benefit when the risk threshold for in-hospital MACE after PCI in STEMI patients was 0.1 to 0.78 (Figure 7).
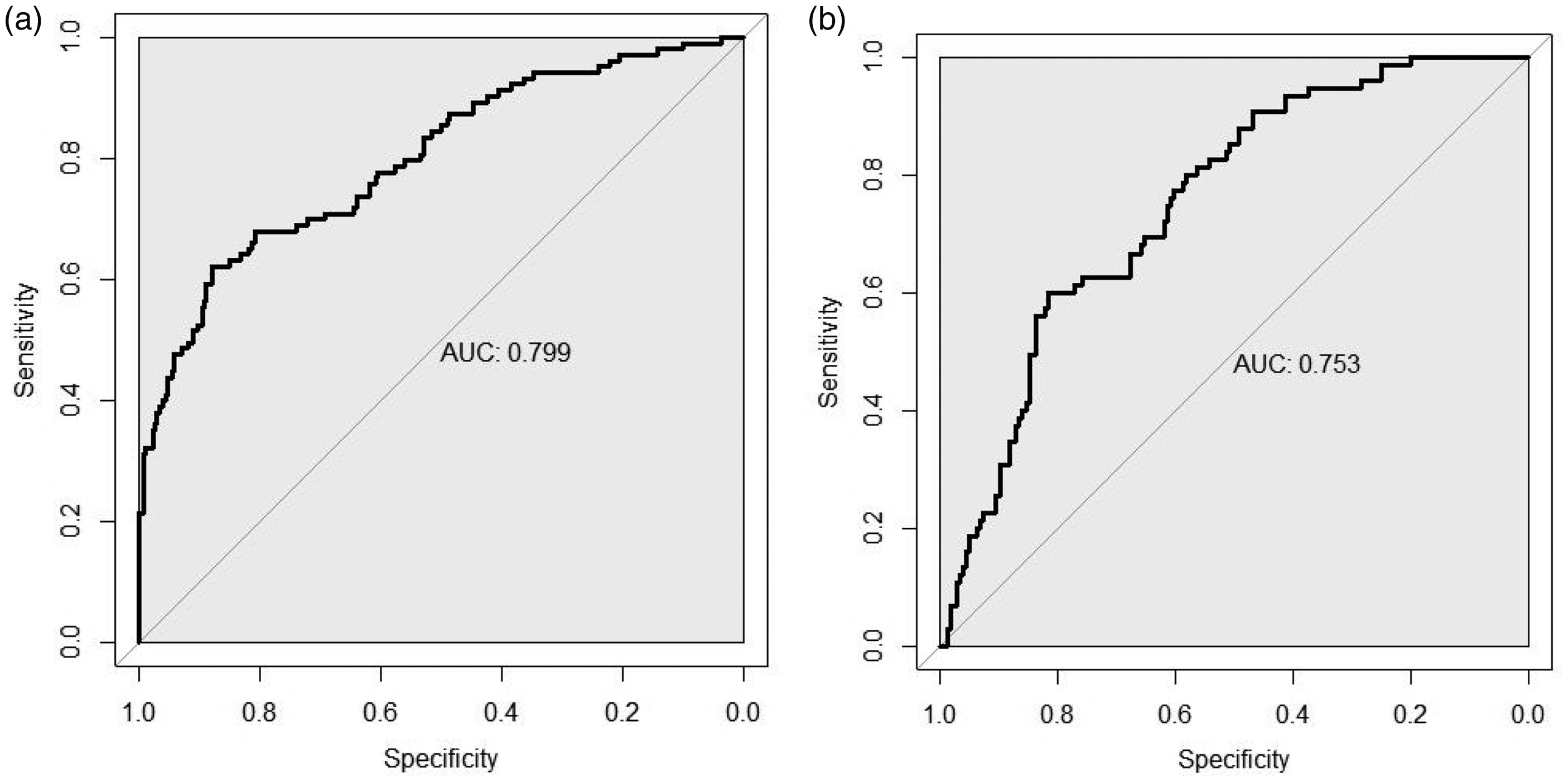
ROC curves to assess the predictive efficacy of the model for predicting the occurrence of major adverse cardiac events after percutaneous coronary intervention in patients with ST-segment elevation myocardial infarction. (a) Training set ROC curve and (b) validation set ROC curve. ROC, receiver operating characteristic.
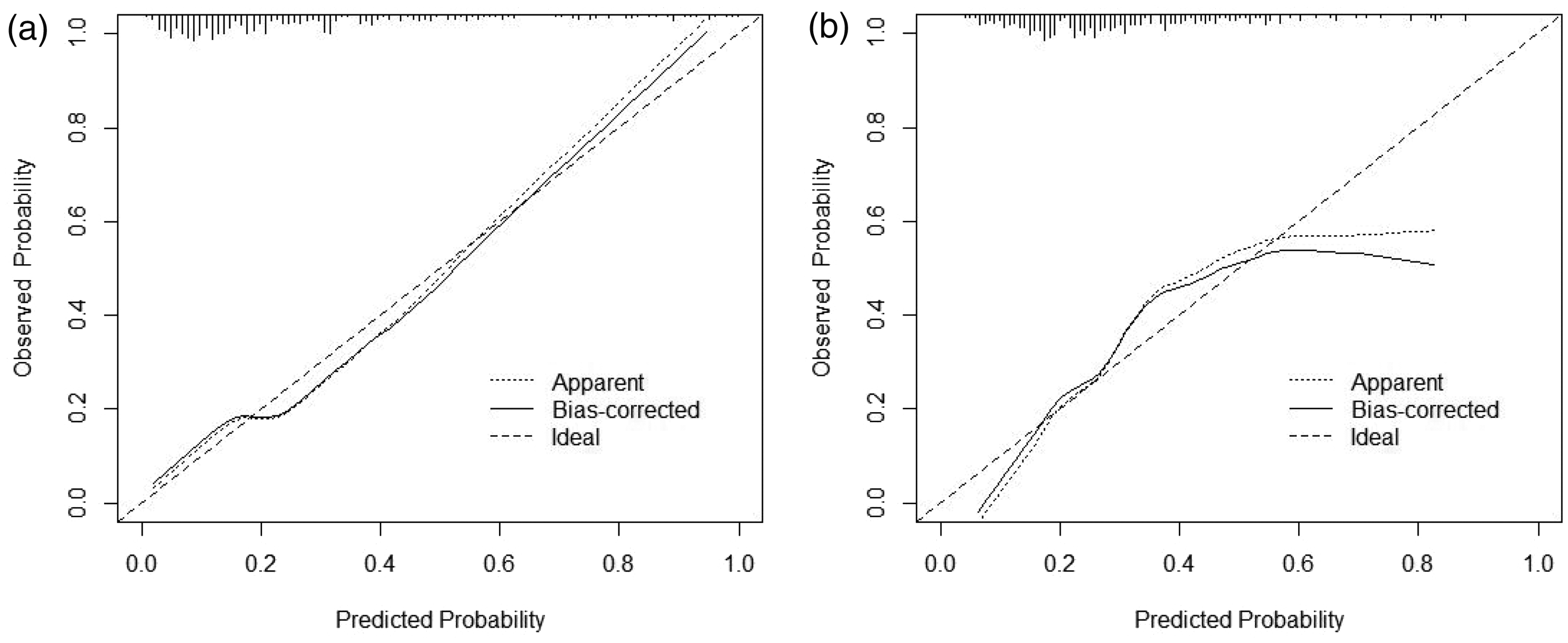
Calibration curves. (a) Training set calibration curve and (b) validation set calibration curve.

Clinical DCA for the nomogram models. (a) Training set DCA and (b) validation set DCA. DCA, decision curve analysis.
Discussion
In the present study, we analyzed the independent factors predicting MACE in STEMI patients, including TyG, NHR, urea, DBP, hypertension, and LVEF. An individualized nomogram for predicting MACE in STEMI patients was established using these indicators, and the discrimination, prediction accuracy, and clinical effectiveness of the model were evaluated, all of which were good. The model also had good discrimination, prediction accuracy, and clinical effectiveness in the validation population. Together, our results suggest that this model may be valuable for clinical application. In the current study, individualized nomograms were drawn; the indicators included commonly used indicators for STEMI patients that are easy to collect. Using nomograms, the short-term prognosis of patients may be judged more intuitively and accurately, thus leading to timely and active intervention for high-risk patients and guided communication with patients’ families in the clinic.
Acute coronary syndrome remains a common cause of cardiovascular death worldwide, and its incidence—including STEMI, non-STEMI, and unstable angina pectoris—is increasing. 14 Of these syndromes, STEMI is gradually decreasing but non-STEMI is increasing, thus increasing the economic burden on the global healthcare system and threatening human health and development. 15 Although the mortality rate of STEMI patients has decreased with the development of PCI, antithrombotic therapy, and secondary prevention, the incidence of myocardial infarction-related complications such as heart failure and arrhythmia has gradually increased to become an essential factor affecting the prognosis of STEMI patients. 16 Therefore, the early identification, prevention, and management of complications in patients with myocardial infarction remains a critical research direction in the development of cardiovascular disease.
Several studies have demonstrated that the TyG index is an independent predictor of the development and prognosis of cardiovascular disease;17,18 however, there is no definitive conclusion regarding the cut-off value. Furthermore, it has been reported that the TyG index in patients with acute coronary syndrome19,20 has some predictive value for MACE, as an independent factor of known traditional cardiovascular risk factors. Jin et al. 21 conducted a clinical follow-up observational study of 1282 patients with stable coronary heart disease, and reported that the TyG index was directly proportional to the risk of cardiovascular events; the risk increased by 21.2% for each standard deviation increase in the TyG index (hazard ratio = 1.212, 95% CI: 1.075–1.366, P < 0.05). Similar results were reported in patients with cardiovascular disease in the general population. 22 Moreover, the TyG index is not only associated with acute coronary syndrome, but is also associated with heart failure, 23 stroke, 24 and atrial fibrillation. 25 Similar to previous studies, the present results indicate that STEMI patients with a higher TyG index have a greater risk of MACE after PCI, and an increased risk of subsequent cardiovascular events.
Neutrophils are the first line of defense against pathogen invasion in the human body. They play a crucial role in innate immunity and atherosclerosis, particularly in the inflammatory response to atherosclerosis pathogenesis. 26 Neutrophil recruitment is critical for the inflammatory transformation and regression of myocardial infarction; increased neutrophil recruitment is related to poor prognosis in myocardial infarction. 27 Similarly, HDL-C has a number of physiological activities, of which the most studied and recognized is its role in enhancing the excretion of excess cholesterol from peripheral tissues to the liver, thereby inhibiting the development of atherosclerosis. 28 HDL-C has antioxidant, anti-inflammatory, and antithrombotic effects, and its role in blood circulation cannot be neglected. 29 Furthermore, Li et al. 30 demonstrated that HDL-C is a protective factor for multivessel disease in young men with acute myocardial infarction. Similarly, Park et al. 31 reported that low HDL-C levels increase the risk of cardiovascular death and recurrent myocardial infarction in patients with acute myocardial infarction treated with PCI and statins, whereas high HDL-C levels may reduce the risk of cardiovascular events, particularly in patients with STEMI. Similar to previous findings, our results indicate that STEMI patients with higher neutrophil levels and lower HDL-C levels have a higher risk of cardiovascular events.
In the present study, DBP was lower in STEMI patients who developed in-hospital MACE after PCI than in those who did not develop in-hospital MACE. When predicting the risk of early MACE in patients with STEMI, a severely impaired LVEF (<30%–40%) indicates worse left ventricular systolic function, lower blood pressure, and larger myocardial infarct size after myocardial infarction, which are reportedly strongly associated with adverse events and high mortality after myocardial infarction. 32 Similarly, in a study of 417 patients with acute myocardial infarction, LVEF < 40% was an independent predictor of a combined endpoint of death, congestive heart failure, and recurrent acute myocardial infarction 30 days after acute myocardial infarction. 33 A study of 28,771 patients with heart failure, left ventricular dysfunction, or both after acute myocardial infarction demonstrated that the risk of all types of death increases with decreasing LVEF. 34 Consistent with previous reports, the present findings suggest that STEMI patients with lower LVEF are more prone to MACE events during hospitalization.
Renal dysfunction in STEMI patients is reportedly one of the most important predictors of in-hospital and long-term mortality. 35 Serum creatinine levels are also closely related to prognosis after treatment. 36 In the present study, urea levels were significantly higher in the group with MACE than in the group without MACE, and elevated blood urea levels were an independent risk factor for MACE after PCI in STEMI patients. The early restoration of effective myocardial reperfusion in STEMI patients is critical for reducing acute mortality and improving prognosis; however, interventional or medical therapy is often limited by renal function and serum creatinine levels. Therefore, serum creatinine and urea levels should be used as significant predictors of prognosis when creating individualized treatment regimens, and risk stratification should be performed according to renal function status and blood urea nitrogen and creatinine levels, to effectively reduce mortality and improve hospital outcomes.
Hypertension is a significant risk factor for coronary heart disease. 37 Moreover, myocardial infarction is one of the most common cardiac insults in hypertensive patients. Hypertensive patients have left ventricular hypertrophy caused by increased long-term peripheral resistance. Left ventricular hypertrophy predisposes patients to myocardial infarction because of increased oxygen consumption and a relatively reduced myocardial capillary density. Furthermore, target organs (especially the heart) are compromised in hypertensive patients. MACE events are therefore likely the result of myocardial ischemia and reduced cardiac systolic and diastolic function.
Shortcomings remain in the present study. First, the study was a two-center investigation with a limited sample size, and thus cannot avoid bias. Second, in terms of model validation, further validation from a multicenter, large-scale prospective study is required. Third, data on the use of lipid-lowering or hypoglycemic drugs were not included. For the clinical application and promotion of our model, large-sample, multicenter clinical data are therefore needed; these data will provide evidence to support the further exploration of factors that influence in-hospital MACE after PCI in STEMI patients, and will help to optimize the nomogram model.
Conclusion
The present findings indicate that NHR, TyG index, urea, systolic blood pressure, hypertension, and LVEF are risk factors for in-hospital MACE after PCI in STEMI patients. Our nomogram model for in-hospital MACE risk prediction after PCI in STEMI patients, which was constructed using the aforementioned influencing factors, had good discrimination, calibration, and clinical effectiveness. It may therefore be an effective tool for the early clinical prediction of in-hospital MACE risk after PCI in STEMI patients, thus achieving early detection, reporting, and treatment, and improving the prognosis of patients.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241258181 - Supplemental material for Establishment and validation of a nomogram model containing a triglyceride-glucose index and neutrophil-to-high-density lipoprotein ratio for predicting major adverse cardiac events in patients with ST-segment elevation myocardial infarction
Supplemental material, sj-pdf-1-imr-10.1177_03000605241258181 for Establishment and validation of a nomogram model containing a triglyceride-glucose index and neutrophil-to-high-density lipoprotein ratio for predicting major adverse cardiac events in patients with ST-segment elevation myocardial infarction by Zhi-Chao Xu, La-Mei Pang, Min Chen and Guang-Quan Hu in Journal of International Medical Research
Footnotes
Acknowledgement
The authors thank Caoyang Fang for statistical support.
Author contributions
ZCX collected and analyzed the data and wrote the manuscript; LMP analyzed the data and critically analyzed and accepted the final manuscript; MC analyzed the data and approved the final manuscript; GQH analyzed the data, wrote the manuscript, and accepted the final manuscript. All authors read and approved the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.