
Abstract
Autoimmune encephalitis (AIE) is a rapid, progressive neurological disorder characterized by nervous system inflammation. While the Graus criteria are the best known criteria for AIE diagnosis, other differential diagnoses meeting the Graus criteria must be considered before management. This narrative review discusses the most common etiologies that resemble AIE. We suggest routine exclusion of mimickers meeting the Graus criteria before confirming an AIE diagnosis. We reviewed 28 studies including 356 patients. The main initial diagnosis was AIE, then paraneoplastic limbic encephalitis and anti-N-methyl-D-aspartate receptor encephalitis. Only 194 patients met the possible Graus criteria. The most frequent conditions among the total population were dementia, other neurodegenerative diseases, and psychiatric and functional neurological disorders. AIE is often misdiagnosed, leading to unnecessary treatment. Despite publication of the Graus criteria, medical cases mimicking this condition are being published. Many neurological diseases entering the differential diagnosis of AIE could be excluded through a detailed history, neurological examination, laboratory analysis, and other investigations, including cerebrospinal fluid and brain magnetic resonance imaging. However, some differential diagnoses complied with the possible Graus criteria, with some having concurrent antineuronal antibodies, which were considered true mimickers. AIE diagnosis suspicion is primarily clinical, but a definitive diagnosis requires various diagnostic tools.
Keywords
Introduction
Autoimmune encephalitis (AIE), the third most common cause of encephalitis, with a prevalence of 13.7/100,000), 1 is a rapid, progressive neurological disorder that is characterized by inflammation of the brain and other areas of the nervous system. It is caused by an abnormal immune response 2 with production of antibodies against cell surface, synaptic, or intraneuronal antigens, also known as onconeural antibodies. 3
AIE is classified anatomically depending on its location (limbic, cortical/subcortical, striatal, diencephalic, brainstem, cerebellar, encephalomyelitis, meningoencephalitis or combined) or serologically (antibodies to intracellular antigens, antibodies to surface antigens, seronegative AIE). 2
Despite the progress that has been made in this field, the diagnosis of AIE remains clinical. 2 The Graus criteria for AIE are the most well-known criteria for AIE diagnosis, although two later studies showed that the sensitivity and specificity of these criteria did not exceed 80% and 84% to 94%, respectively.4,5 Moreover, these criteria do not take into account that AIE tends to develop gradually before manifesting the classical clinical, laboratory, and radiological picture that fulfills the diagnosis, 5 and the diffuse inflammation caused by antibodies leads to different syndromes depending on its location. 2 Those syndromes may sometimes overlap, 2 and therefore it is difficult to establish a single criterion encompassing them all. In addition, many studies concluded a final diagnosis of AIE—particularly anti-N-methyl-D-aspartate (NMDA) encephalitis—despite not achieving probable anti-NMDA criteria.6,7 Furthermore, the existence of anti-neuronal antibodies failed to be pathognomonic because 62% of patients tested positive for these antibodies, and these patients had alternative diagnoses in the study by Abboud et al. 2
To increase the complexity, the magnetic resonance imaging (MRI) results, which is the primary tool used for AIE diagnosis, can mimic those of other lesions such as stroke and tumors. Under the appropriate clinical picture, MRI results cannot differentiate between different immune-mediated conditions (AIE, sarcoidosis). 2 Once the diagnosis is made, early initiation of immunotherapy is crucial for the prognosis. 8 However, before starting immunotherapy, other possible diagnoses, some of which may benefit from this treatment such as central nervous system lymphoma, should be excluded.
Because of the above, AIE is a challenging diagnosis as almost any brain lesion can enter its differential diagnosis list, including infections, demyelinating and other autoimmune disorders, nutritional deficiencies, neurodegenerative diseases, primary brain tumors, and even primary psychiatric disorders, paraneoplastic sarcoidosis, and neurosarcoidosis.2,9 Many of these mimickers can be excluded via a detailed history, examinations, cerebrospinal fluid (CSF) findings, and radiological imaging. 8 Furthermore, AIE is usually acute, subacute, or in specific cases chronic and follows a progressive or monophasic pattern. Thus, hyperacute presentation or relapse-remitting patterns should raise suspicion of other entities such as vasculitis or multiple sclerosis. 2
This manuscript is a narrative review aiming to identify the most common etiologies that resemble AIE, focusing on the prevalence of such misdiagnoses, and discussing possible reasons for these medical errors to prevent the inappropriate use of steroids. In this study, we performed a thorough review of mimicking conditions that met the probable AIE Graus criteria and which we believe should be in the forefront of the differential diagnosis of AIE. We also suggest that these conditions should be routinely considered as possible diagnoses when performing a work-up.
Methods
Search strategy
We conducted an electronic database search for AIE mimicker studies in PubMed and Google Scholar using the following search terms: (mimic*) AND (((“Brain Inflammation”) OR (Encephalitis)) OR (encephalomyelitis)). A total of 1589 studies were found. In addition to the references, a manual search was performed. We limited the search results to English-language publications.
Inclusion and exclusion criteria
We included any type of publication (case report, case series, cohort) that included the following:
Patients with disorders that mimicked or resembled the clinical and/or radiological features of AIE All studies meeting Graus’ possible criteria People from all age groups English literature
Exclusion criteria:
Studies that did not fulfill both the clinical and radiological features of AIE Publications in which AIE was the final diagnosis or studies mentioning cases of AIE presenting as other diseases
The studies included diseases mimicking AIE such as Hashimoto’s encephalopathy, acute disseminated encephalomyelitis, Rasmussen encephalitis, Bickerstaff brainstem encephalitis, Morvan syndrome, stiff person syndrome, and other disease entities that share the same immune backgrounds (see the Limitations section).
Data collection and statistical analysis
Data extraction was performed by MZBA and MSA using Endnote X8 and Microsoft Excel to format the table. The extraction table includes the authors’ names, year, study design, number of patients, country, age, sex, presentation, initial diagnosis, etiology or final diagnosis, method of diagnosis, laboratory tests, and imaging investigations.Six authors (MZBA, MSA, MZ, TB, MT, NA) screened the studies according to the inclusion and exclusion criteria to select appropriate articles. Regarding the etiology, the data were collected using two independent methods: general and then only cases that fulfilled the possible Graus criteria.
Results
A total of 1589 studies were found. After excluding duplicate papers and applying the inclusion and exclusion criteria, we identified 28 studies for inclusion in our review. Those studies were included and formatted in the extraction table. The included studies were published between 2005 and 2023. These studies included 19 case reports, 1 case series (6 patients), 3 retrospective studies (109 + 109 + 107 patients), 4 letters to the editor, and 1 short communication (Figure 1) (Table 1).

Flow chart of the patients.
Baseline Information.

m, male; f, female.
In all studies, different types of AIE were initially proposed as diagnoses. Later, after additional tests and follow-up, these patients were given different diagnoses. (except for 83 patients in a retrospective study in which the final diagnosis was not mentioned). 5
A total of 356 patients were included, with a slight female preponderance. The patient age ranged between 3 and 93 years (Table 1).
The main presentations were new onset of seizure, altered mental status, neuropsychiatric symptoms, memory deficit, and focal neurological signs (Table 1).
The main initial diagnosis in the studies was AIE, followed by paraneoplastic limbic encephalitis and anti-NMDA receptor encephalitis (Table 2).
Initial diagnosis, method of diagnosis, and types of mimics.

DDX, differential diagnosis; HSV, herpes simplex virus; VDRL, venereal disease research laboratory; NMDA, N-methyl-D-aspartate; nm, not mentioned; MRI, magnetic resonance imaging; CT, computed tomography; AIE, autoimmune encephalitis; CSF, cerebrospinal fluid; IHC, immunohistochemistry.
The final etiologies for the total population and individuals who fulfilled the possible AIE criteria are listed in Figure 2. The total number of etiologies mentioned was 79 for those not meeting the Graus criteria for possible diagnosis and 194 for those meeting this criteria (Figure 2).
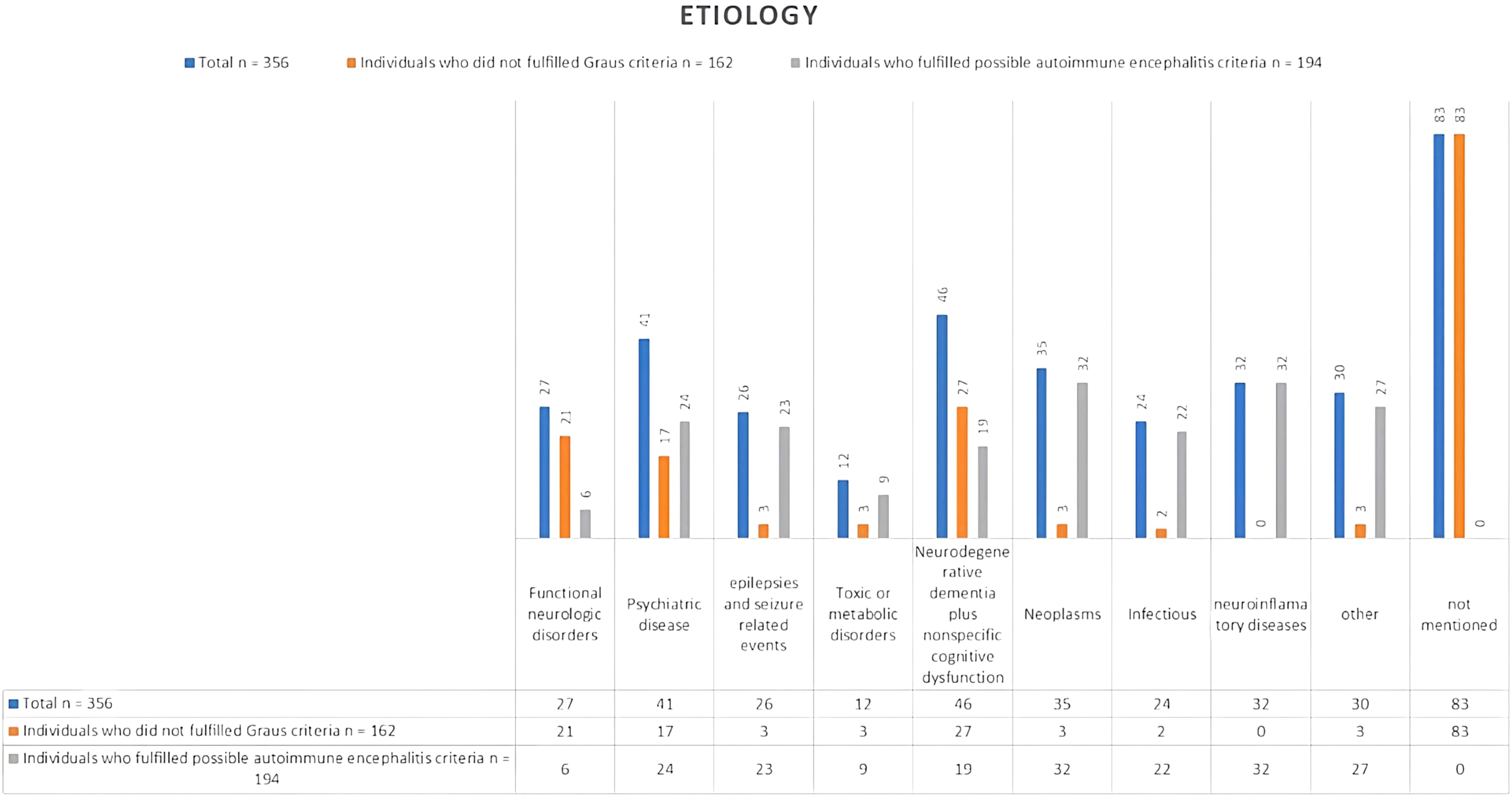
Bar chart showing the different etiologies that mimic autoimmune encephalitis.
The most common differential diagnosis lists differed between the two groups. Dementia and other cognitive disorders were most common for patients who did not meet the Graus criteria, followed by psychiatric diseases, especially conversion disorder. This finding differs from that of patients who met the possible Graus criteria, where neuroinflammatory disorders such as multiple sclerosis, along with neoplasms, were the primary considerations. Psychiatric diseases and convulsive disorders followed. The third position included infectious diseases, especially neurosyphilis. The final diagnosis was most frequently established by a brain biopsy; laboratory testing; imaging including electroencephalography (EEG), MRI, and computed tomography (CT); antibody tests; and CSF tests (Table 3).
Final diagnosis, findings, and management of autoimmune encephalitis mimics.

EEG, electroencephalography; MRI, magnetic resonance imaging; CSF, cerebrospinal fluid; nm, not mentioned; FLAIR, fluid-attenuated inversion recovery; PEG, percutaneous endoscopic gastrostomy; NMDA, N-methyl-D-aspartate; VDRL, venereal disease research laboratory; RPR, rapid plasma reagin; TPPA, Treponema pallidum particle agglutination.
EEG was performed for 24 of the most frequent abnormalities including waves with slowing and discharges (Table 3).
All patients had undergone MRI, and the most frequent findings were suggestive of a brain lesion (8 of 25 patients). CT scans were performed on 9 of 25 patients; 5 scans were unremarkable or normal, and 1 thoracic CT scan showed a hyperdense lesion of 1.6 cm in the left superior pulmonary lobe that was suspected to be carcinoma.
The other patients showed non-specific mild global atrophy, obscure cerebral gyri in the left frontal and temporal regions, or hypometabolism in the frontoparietal and parietooccipital cortices (Table 3).
In total, 117 of 356 patients showed positivity for antibodies including anti-GAD antibodies and anti-measles antibodies, low titers of glycine receptor antibodies, anti-LGI1 IgG antibodies, CASPR2-antibodies, anti-NMDA and Treponema pallidum antibodies (IgG-western blot). Thyroid peroxidase antibodies were present in 24 patients, neural autoantibodies were found in 48 patients, GAD65 antibodies were present in 14 patients, voltage-gated potassium channel complex antibodies (LGI1 and CASPR2 negative) were present in 10 patients, and NMDA receptor antibodies (cell-based assay) were present in 10 patients. In addition to IgG, anti-GQ1b antibody positivity, anti-recoverin antibodies, and anti-GluR3 antibodies were found in some cases.
CSF analysis was performed for 25 patients, and only eight tests were normal. The most common abnormalities were lymphocytic pleocytosis, elevated protein levels, and neural autoantibodies. Other abnormalities included blood-CSF barrier damage, positive oligoclonal bands, and high titers of anti-measles antibodies. In addition, positive rapid plasma reagin and Treponema pallidum particle agglutination tests and anti-GluR3 antibodies were found.
Of the 25 patients, only 2 patients had undergone a Mini Mental State Examination (raw scores 13/30 and 25/30). Other patients underwent a neuropsychiatric evaluation, which revealed profound memory loss (Table 3).
Steroids (methylprednisolone or dexamethasone) were most commonly used as initial management (11 of 25 cases). Other medications and procedures included intravenous immunoglobulins (4 cases), intravenous acyclovir (2 cases), intravenous fluids, sodium valproate, cyclophosphamide, tryptophan immunoadsorption, levetiracetam, and plasmapheresis.
The final management in most cases targeted controlling the underlying pathology that mimicked AIE.
The most frequent management strategy was chemotherapy and/or radiation (5 cases). The other strategies included penicillin G (4 cases), neurosurgery (3 cases), intravenous immunoglobulins (2 cases), isoprinosine, clonazepam, valparin, stopping pregabalin use, hydrocortisone, and fludrocortisone (Table 3).
Discussion
According to the Brighton Collaboration Encephalitis Working Group, the term encephalitis refers to encephalopathy or any other neurological symptom emerging from brain parenchymal inflammation. 10 This inflammation is initially caused by infections, followed by acute disseminated encephalomyelitis. 1 The immune basis of this inflammation was first mentioned by Corsellis et al. in 1968, when they referred to cases of paraneoplastic limbic encephalitis. 11 Later, this term expanded to be a part of AIE. 5
In this context, AIE consists of a set of neuropathies caused by an immune-mediated process and shares the presence of gray matter inflammation in the brain, which may extend to involve the white matter, meninges, and spinal cord. 2
According to the definition, AIE can be classified anatomically depending on the location (limbic, cortical/subcortical, striatal, diencephalic, brainstem, cerebellar, encephalomyelitis, meningoencephalitis, or combined) 2 or pathologically depending on the antibody type and the immune process involved 1 (cytotoxic T-cell-mediated antibodies against intracellular antigens vs antibodies against surface antigens that involve humoral immunity). 12 Seronegative AIE has also been described and may represent antibodies that have not been reported. 2
AIE symptoms vary according to the affected area of the brain and usually overlap. 2 Therefore, the diagnosis is difficult and depends on a high clinical suspicion because, first, the progression of symptoms is gradual and sometimes it takes weeks before the clinical picture becomes clear. 5 Second, MRI results demonstrate non-specific inflammatory findings or appear normal in most cases. 1
AIE is a rare disease (the incidence is approximately 3 to 9 per million) 5 but encompasses a high rate of misdiagnosed cases, 5 which may lead to medical errors because of unnecessary application of steroids and immunosuppressive therapy. Despite the publication of the Graus criteria in 2016, in which the diagnosis is classified according to its reliability as possible or definite, 5 cases mimicking AIE are still being published. This phenomenon can be understood in the following context. In two later studies4,5 the sensitivity of Graus’ criteria did not exceed 80%, and the specificity was approximately 84% to 94%, with an established linear relationship between sensitivity and AIE progression. 4 In another two retrospective studies that were conducted in leading clinics in the USA and specialist centers in Portugal, the numbers of mimicking conditions were 107 of 393 in the study by Flanagan et al 12 and 26 of 39 in the study by Costa et al., 5 and similar studies in other countries were lacking. Additionally, the prevalence of mimicking conditions greatly surpassed that of AIE. 12 Finally, the rush to order neuronal antibodies and overinterpretation of their existence was mentioned by Flanagan et al. 12 as an affecting factor because positivity for neuronal antibodies may be seen in up to 5% of patients. 12 This argument was supported by our review regarding misdiagnosis of mimicker cases, which mentioned the positivity of these antibodies, especially antibodies against GAD, CASPER2, LG-1, and NMDA.13–16
Many neurological diseases are considered in the differential diagnosis of AIE. Fortunately, many can be ruled out through a detailed history, neurological examination, laboratory analyses, and other investigations such as CSF analysis and brain MRI. 2 According to our review, neurodegenerative dementia (such as Alzheimer’s disease, dementia with Lewy bodies, Creutzfeldt-Jakob disease, behavioral variant frontotemporal dementia, vascular cognitive impairment, and normal pressure hydrocephalus) and nonspecific cognitive syndrome were the most common conditions, followed by psychiatric disorders, especially functional neurological disorders or conversion syndrome. Other diseases included neoplasms such as gliomas (glioblastoma, astrocytoma, or those not otherwise specified), lymphomas, cerebellar medulloblastoma with cerebellar cognitive syndrome, infectious encephalitis (especially viral encephalitis and neurosyphilis, even without recognizing the primary infection, human immunodeficiency virus, and residual prior viral encephalitis), seizures, and psychological reasons such as depression, anxiety, schizophrenia, and bipolar syndrome. Other causes included multiple sclerosis, small vessel vasculitis, neurosarcoidosis, toxic-metabolic causes including medication, delayed neuropsychiatric syndrome of carbon monoxide poisoning, non-immunotherapy responsive progressive cerebellar degeneration with cerebellar cognitive syndrome, Kleine–Levin syndrome, mitochondrial encephalomyopathy, lactic acidosis, stroke-like episodes, adrenal insufficiency, and Wernicke encephalopathy. Four other cases were also mentioned, including common variable immunodeficiency, neuroendocrine tumor with a merkel cell carcinoma immunophenotype, pregabalin abuse, and 4-aminopyridine toxicity. It should be noted that the last case did not meet the Graus 2016 criteria because of the presence of a clear cause of encephalopathy, as the patient had mentioned taking medication and had hyperacute development of symptoms. This result is different from that of the retrospective study by Flangan et al., when considering cases that did not meet the probable Graus criteria. 12 That study focused on AIE mimickers in the adult population and functional neurological disorders followed by dementia. This discrepancy is possibly attributable to the larger sample size of our study. It is important to note that these findings should be interpreted with respect to the patient's age. 17 Functional neurological disorders were predominant in the pediatric group, followed by epilepsy. 18 Genetic diseases such as mitochondrial diseases and leukodystrophies are also important differential diagnoses. Additional conditions to consider, as per Dalmau and Graus, include new-onset refractory status epilepticus, pediatric autoimmune neuropsychiatric disorder associated with streptococcal infection, and the closely linked pediatric acute-onset neuropsychiatric syndrome. 17
Some differential diagnoses complied with the possible Graus criteria, and some even included concurrent antineuronal antibodies. These were considered to be true mimickers. Unfortunately, because of the significant heterogeneity among the study designs, we could not perform a major review and only attempted to highlight the mimickers.
The most common mimickers in this category were neuroinflammatory diseases, which included the same number of patients as those with neoplasms. This was followed by seizures and epileptic disorders, along with psychiatric disorders and infectious diseases, and finally dementia and other cognitive disorders. One study also noted that Susac’s syndrome is a significant differential diagnosis for individuals meeting Graus' possible criteria, 8 with no published cases yet.
AIE and its mimics can affect both sexes equally. There is a negligible difference in sex preponderance according to our study and studies of Diogo Costa et al. 5 and Eoin P. Flanagan et al. 12 The median age for this disease is 61.7 ± 15.5 years. 2 However, it affected individuals aged from 3 to 93 years.
Symptoms of AIE and its mimics are similar, depending on the area that they affect. In general, the most common symptoms reported in the medical literature and in our study were altered mental status (most common), seizures, movement disorders, neuropsychiatric symptoms, working memory deficits, focal neurological signs, and other symptoms such as ataxia, autonomic dysfunction, paraparesis or tetraparesis, visual loss, and generalized pain. 2
In two literature reviews1,10 concerned with syphilis and glioblastoma and their potential to mimic AIE, the symptoms were not different from the symptoms reported above. Nevertheless, in two cases, the presence of speech disorders, progressive forgetfulness, and apathy was noted in patients with syphilis.13,19 This was also true for glioblastoma, in which in addition to language dysfunction, right-side hypoesthesia and homonymous lateral hemianopia were reported. 20
Suspicion of an AIE diagnosis in a patient relies on the clinical presentation. 5 However, reaching a definitive diagnosis requires a variety of diagnostic tools, primarily MRI. It should be noted that brain biopsy, despite its morbidity, remains the gold standard for these diseases. 10 Fortunately, it is not usually indicated, 2 but in most of our reviewed cases, it was used to confirm the diagnosis. Therefore, we suggest that it should be performed in complicated cases to prevent a delay in treatment.
MRI remains the most critical component in the diagnosis of neurological disorders and was used in all cases reviewed thus far because of its importance. Graus noted that detecting bilateral limbic encephalitis is the only definitive method for diagnosing AIE, as other types of AIE present with nonspecific inflammatory changes. 8 AIE appears as a bilateral hyperintense lesion on T2/fluid attenuated inversion recovery (FLAIR) sequences. This pattern has been observed in many other diseases, some of which only imitate AIE radiologically (such as herpes simplex encephalitis, status epilepticus, mesial temporal sclerosis, and posterior cerebral artery infarct). 12 Other diseases are real mimickers. For example, according to our results, neurosyphilis and AIE have the same MRI findings. Another challenging example is Creutzfeldt–Jakob disease, which according to Macchi’s review, 21 tends to exhibit the same radiological picture as AIE. One exception was observed by Zuhorn et al., 15 in which no MRI abnormality was detected.
EEG is essential to examine AIE and its mimics. A normal pattern, focal or diffuse slowing, periodic discharges, and extreme delta brush are all common in both AIE and its mimics. However, in our view, EEG was not very useful in differentiating among these diseases, except for Creutzfeldt–Jakob disease, where EEG (disease-typical periodic sharp wave complexes, which are different from those observed in AIE) is considered crucial based on the diagnostic calcification established by the World Health Organization. The main problem is that this pattern usually emerges in later stages of the disease. 22
As shown by the Graus criteria, the CSF plays a pivotal role in the diagnosis of AIE. Detection of antineuronal antibodies and moderate lymphocytic pleocytosis, with a count of less than 100 cells, are the typical findings. CSF analysis was performed in most cases and revealed nonspecific abnormalities. However, it can be useful in detection of Treponema pallidum and other infections. 23 It is important to note that the absence of pleocytosis does not exclude the possibility of an AIE diagnosis. 1 In our review of mimickers, the most common abnormalities were lymphocytic pleocytosis, elevated protein levels, and even a concurrent presence of neural autoantibodies, which led to misdiagnosis.13–16
Brain CT was used in nine of the studied cases. Five of those nine cases had normal results. This finding demonstrates the small role of CT in disease diagnosis. Nonetheless, CT could be helpful when considering paraneoplastic cases or extra-neurological syndromes. Otherwise, it has a low priority.
In conclusion, accurate and rapid diagnosis of AIE and administration of immunosuppressants, especially methylprednisolone, is essential to prevent death. According to our study, we suggest that a rapid screen for these mimickers, especially those that meet the Graus criteria, such as glioma, seizures, and syphilis, is essential and should be included in the Graus criteria and within the primary work-up. Additionally, risk is involved in the hurried use of immunosuppressive drugs. Unfortunately, the lack of adequate studies and the heterogeneity in the present cases prevented us from focusing on studies that met the Graus criteria. We also recommend that larger studies should be carried out in the future focusing on these mimickers in particular.
Limitations
In our study, we focused on mimickers of limbic AIE in particular because of the absence of clear boundaries between diseases considered an AIE subtype and those deemed an independent entity and the presence of many other diseases with immunological backgrounds, such as acute disseminated encephalomyelitis, Bickerstaff’s brainstem encephalitis, Hashimoto encephalopathy, and Rasmussen's disease. Another important point is that the criteria focus on syndromes with a subacute presentation, leading to the exclusion of chronic syndromes such as stiff person syndrome and Morvan syndrome.
24
The latter can be caused by both immunological and non-immunological pathologies. Low numbers of studies with some heterogeneity among them (28 cases and three retrospective studies). We considered that all of the 25 included cases had met the Graus criteria theoretically by having a logical reason to deny other differential diagnoses, especially in the cases of acute medication toxicity (4-aminopyridine toxicity).
Footnotes
Author contributions
MSA: Conceptualization, Methodology, Writing – Original Draft; MM: Conceptualization, Software, Writing – Original Draft; MT: Investigation, Writing – Original Draft; NA: Investigation, Writing – Original Draft; TB: Writing – Original Draft; MZBA: Conceptualization, Methodology, Writing – Review & Editing.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.