
Abstract
Tibial tubercle avulsion fractures (TTAFs) are rare but typical in children and adolescents and Osgood-Schlatter disease (OSD) may be involved in their pathogenesis. However, few publications have reported the relationship between OSD and TTAF. A 16-year-old healthy male adolescent presented with pain, swelling and limited range of motion of the right knee following sudden acceleration while running. Based on the radiographic evidence, the patient was diagnosed with an avulsion fracture of the right tibial tubercle and OSD. Open reduction and internal fixation were performed using two cannulated screws and two Kirschner wires. The patient returned to preinjury activity levels at the 12-month follow-up postoperatively. This case report aimed to highlight this unique injury pattern. For patients with TTAFs, not only should the fracture be treated, but the cause of the fracture, such as OSD, should also be given appropriate treatment.
Introduction
Tibial tubercle avulsion fractures (TTAFs) are rare but typical in children and adolescents, accounting for 3% of all proximal tibial fractures and 1–2% of all epiphyseal injuries. 1 They mainly affect teenagers who participate in jumping and sprinting sports (such as basketball and football); injuries in adults are rare. 2 Osgood-Schlatter disease (OSD), commonly described as tibial tubercle osteochondrosis or aseptic necrosis of the tibial tubercle epiphysis, is inflammation of the bony tissue traction at the junction of the patellar tendon and tibial tubercle. 3 It is caused by repeated movements and overuse during rapid growth periods. 4 Thus, patients with OSD are at an increased risk for avulsion fractures due to repeated weakening of the cartilage and maturation of the patellar tendon fibrocartilage.5,6 This current case report describes the diagnosis and treatment a male adolescent with pre-existing OSD and an avulsion fracture of the right tibial tubercle who was admitted with pain, swelling and limited range of motion of the right knee following sudden acceleration while running.
Case report
In September 2020, a 16-year-old healthy male adolescent (body mass index, 35 kg/m2) presented to the Department of Orthopaedics, The Second Hospital of Jilin University, Changchun, Jilin Province, China with pain, swelling, and limited range of motion of the right knee following sudden acceleration while running. Prior to the injury, he experienced anterior knee pain after strenuous activity that resolved with rest and therefore did not seek medical attention. On examination, the patient’s right knee was swollen. A prominent deformity was observed in the tibial tubercle region of the affected knee, although the overlying skin was intact. The patient could neither straighten nor raise his right knee. Signs of neurovascular impairment were not observed. The radiographs of the right knee indicated ‘avulsion fracture of the right tibial tubercle and OSD’ (Figure 1). Computed tomography with three-dimensional reconstruction of the right knee showed ‘avulsion fracture of the right tibial tubercle and OSD’ (Figure 2). This patient was diagnosed with an Ogden Type IIIA TTAF with preexisting OSD. 6

Preoperative radiographs of the right knee of a 16-year-old healthy male adolescent who presented with pain, swelling and limited range of motion of the right knee following sudden acceleration while running: (a) anteroposterior and (b) lateral radiographs showing Osgood-Schlatter disease (red arrow) and an avulsion fragment of tibial tubercle fracture (yellow star). The colour version of this figure is available at: http://imr.sagepub.com.

Preoperative computed tomography (a–c) and three-dimensional model reconstruction (d and e) of the right knee of a 16-year-old healthy male adolescent who presented with pain, swelling and limited range of motion of the right knee following sudden acceleration while running showing Osgood-Schlatter disease (red arrow) and a medially rotated avulsion fracture fragment (yellow star). The colour version of this figure is available at: http://imr.sagepub.com.
Given the significant displacement of the tibial tubercle fracture, conservative treatment was difficult and ineffective in reducing the fracture. The next day, the patient underwent open reduction under epidural anaesthesia. An anterior midline incision was made at the inferior border of the patella of the right knee following effective anaesthesia. The patellar tendon and tibial tubercle were sequentially exposed by incising the skin and the deep fascia. The fracture fragment extended from the tibial tubercle and proximal tibia to the anterior edge of the tibial plateau. The avulsion fracture fragment was displaced proximally by the patellar tendon traction and rotated medially (Figure 2). The fracture was reduced in the knee extension position. Fixation was performed using two cannulated screws and two Kirschner wires; and a negative-pressure drainage tube was placed in the incision (Figure 3). Passive movement of the right knee joint revealed that the fracture fragment was firmly fixed without displacement.
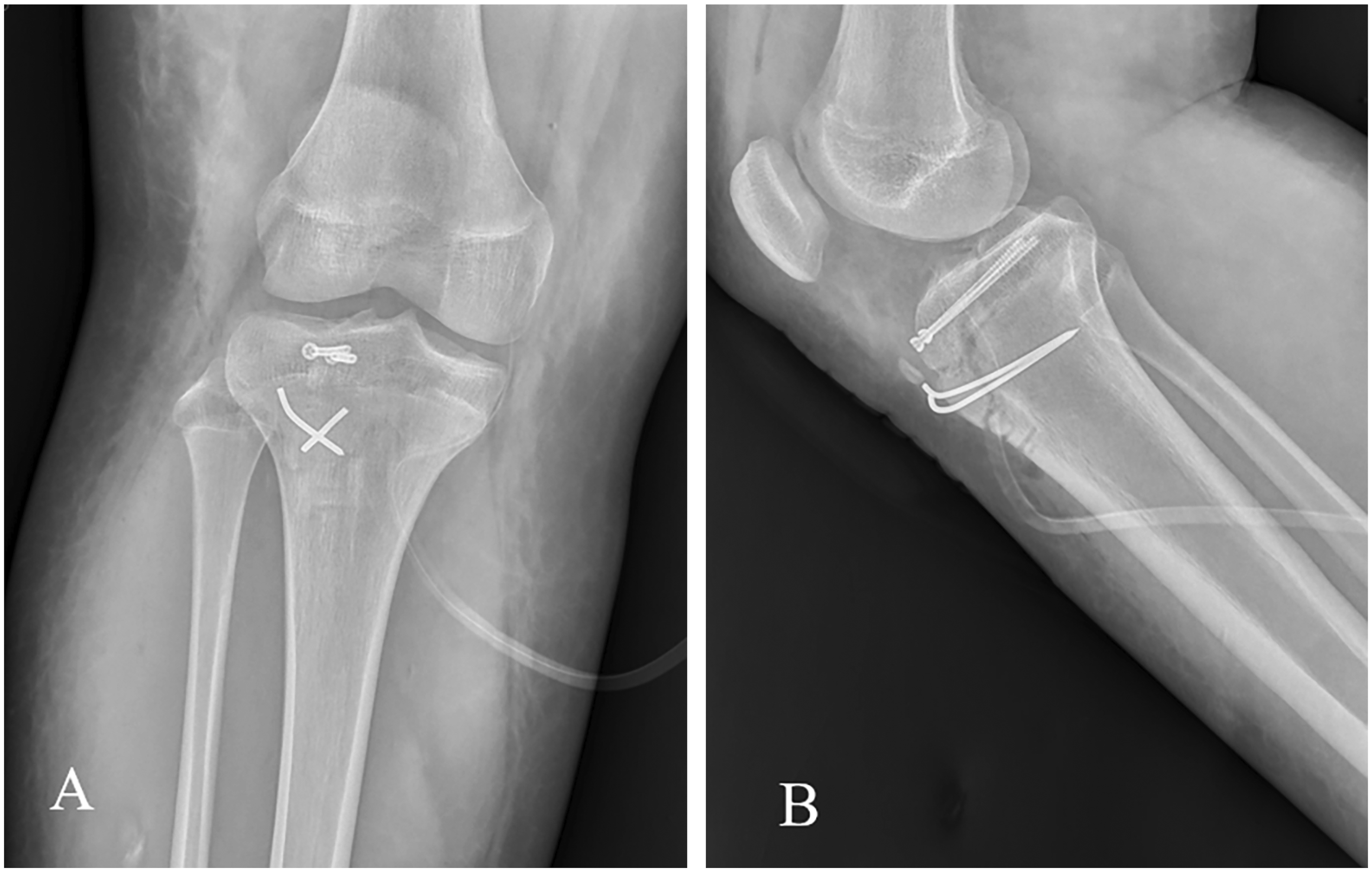
Postoperative radiographs of the right knee of a 16-year-old healthy male adolescent who presented with pain, swelling and limited range of motion of the right knee following sudden acceleration while running: (a) anteroposterior and (b) lateral radiographs showing fixation with two cannulated screws and two Kirschner wires.
Two weeks postoperatively, the stitches were removed and the wound healed. The knee was immobilized in a knee brace for 4 weeks postoperatively. After 4 weeks, the patient was instructed to perform knee range of motion exercises and quadriceps strength exercises. At 3 months postoperative follow-up, the affected knee joint could move from 0° to 120°. The implants were removed at 12 months postoperatively, while the patient had returned to preinjury activity levels. Also, there was no more pain in the front of the knee after activities.
Written informed consent was obtained from the patient's parents for treatment and publication of this case report. Due to the nature of this study, ethics committee approval was not required. The reporting of this study conforms to the CARE guidelines. 7
Discussion
The tibial tubercle is a skeletal bulge 3 cm distal to the tibial plateau. It is the most anterior border of the proximal tibial epiphysis and participates in proximal tibia growth. 8 The epiphysis of the tibial tubercle is not yet fused with the tibial shaft in adolescents younger than 18 years; the epiphysis in males close later than that in females.8,9 The tibial tubercle that is composed of fibrocartilage gradually transforms into columnar cartilage as the epiphysis matures. 10 The columnar cartilage structure is weak and cannot withstand the tension exerted by the knee extensor mechanism. The tibial tubercle is also the attachment point of the patellar tendon on the tibia. Therefore, when the quadriceps contracts, force can be transmitted through the patellar tendon to the tibial tubercle. 11 The muscle strength of the quadriceps is greater in males than in females, which loads more pressure on the tibial tubercle during muscle contraction. 11 In summary, males have later epiphyseal closure, stronger quadriceps strength, and more participation in sports than females, which explains why males are more susceptible to these injuries. Injuries to the knee extension mechanism are rare; with one case report describing how TTAF was mistakenly diagnosed as a fracture of the inferior pole of the patella. 12
Osgood-Schlatter disease is a clinical condition characterized by pain, tenderness and soft tissue swelling at the tibial tubercle. 13 The prevalence of OSD in adolescents is 9.8% and is more common in males. 14 The lack of movement restriction may further contribute to severe bone damage by repetitive contraction of the quadriceps muscle, which can lead to TTAFs. Case series studies have shown that 20–75% of TTAFs in adolescents were diagnosed with OSD.15,16 A typical complication of advanced OSD is the appearance of painful but unfused ossicle near the attachment of the patellar tendon. 17
The TTAF classification (Types I–III) was first proposed by Watson-Jones in 1955. Type I fractures involve a mild avulsion of the tibial tubercle with a slight displacement of the distal tubercle. Type II fractures extend to the proximal tibial epiphysis. Type III fractures affect the knee joint. The classification system was adjusted according to the displacement and comminution of fractures (adding subtypes A and B) and this has become the most popular classification system at present. 6 Type IV was subsequently introduced, which is an avulsion of the entire proximal epiphysis. 18 The addition of subtype C to type I fractures related to patellar tendon injury was subsequently advocated. 19 Finally, type V injuries (a combination of type IIIB and type IV injuries creating a ‘Y’ configuration) were added. 8
To the best of our knowledge, there are some case reports of patients with preexisting OSD before the development of TTAF, but these reports did not discuss the relationship between the two in detail.20 –23 In this current case, a rare low-energy injury induced TTAF. It is our opinion that OSD damages the tendon-bone junction of the patellar tendon and the tibia, which greatly increases the risk of TTAF. A recent study found that patients with OSD had a larger posterior tibial slope compared with controls. 24 It is speculated that patients with OSD will unevenly distribute the force from the extensor mechanism to the patellar tendon to the anterior and posterior segments of the tibia, resulting in unbalanced tibial growth and increased posterior tibial slope. The increased posterior tibial slope will generate greater anterior translational force on the tibia when bearing axial load, which will increase the risk of TTAF. A previous study found an increased posterior tibial slope in both OSD and TTAF patients. 25
For TTAFs without obvious displacement (displacement < 2 mm) in adolescents, long leg plaster fixation in the knee extension position can be used for 4–6 weeks.2,26 Tibial tubercle fractures are mostly caused by high-energy injuries. Fractured fragments often show considerable displacement and require surgical treatment. The key points of treatment are to reconstruct the integrity of the knee extension mechanism and to restore knee stability. 27 As an important part of the knee extension mechanism, the tibial tubercle is subject to strong forces when the knee is flexed and extended. Therefore, anatomical reduction and strong internal fixation are required to prevent the TTAF fragments from displacing or damaging surrounding tissues. Currently, the commonly used surgical and fixation methods include percutaneous prying reduction and Kirschner wire fixation, open reduction and tension band wire fixation, hollow screw fixation and anatomical plate fixation. 28
In the current case, the patient's tibial tubercle fracture block was considered large and the effect of single-use Kirschner wire fixation was unreliable. There is the possibility of utilizing needle withdrawal and re-displacement of the fracture piece, but plate fixation may cause secondary damage to the epiphysis. Single-screw fixation has a poor anti-rotation ability. Therefore, two hollow screws combined with two Kirschner wires were chosen in the current case. Aside from increasing the fixed area, it also produces strong compressive stress on the fracture block, which can resist the traction force on the tibial tubercle when the knee joint is flexed and extended. It can effectively control the rotation and avoid secondary displacement. OSD is a self-limiting disease and it is treated conservatively with rest, ice and quadriceps exercises. 29 However, for patients who fail conservative treatment, arthroscopic surgery can be used to remove the ossicles to avoid damage to the patellar tendon by open surgery. 30
Tibial tubercle avulsion fracture is often caused by violence, and clinicians should pay attention to related injuries such as patellar tendon injury, meniscus injury and anterior cruciate ligament injury. Depending on the fracture type, displacement, and associated injuries, early recognition and treatment usually yield good results. Magnetic resonance imaging may be helpful in properly staging lesions and reducing the possibility of unexpected intraoperative findings.
There are several limitations. A single case report is not enough to provide effective credibility and further studies are still needed to confirm our point of view, but this current case report provides a new perspective to understand the relationship between OSD and TTAF. The coincidence of TTAF and OSD may result from a specific group of patients who, due to their sports discipline, are more exposed to overloads in the tubercle region of the tibia and the closer attachment to the tibia in the knee extensor mechanism.
In conclusion, although TTAFs are rare, their incidence has increased with increased participation in sports in recent years. However, there is often a favourable outcome after surgery. This case report found that OSD, a potential risk factor, may influence the incidence of TTAF. Therefore, while treating TTAF, physicians should also pay attention to the treatment of OSD.
Footnotes
Author contributions
Z.Y.Z. and H.R.Z. contributed equally to this work. Z.Y.Z. and H.R.Z.: conceptualization, writing – original; F.Z.Z. and A.W.: data collection; X.N.L.: writing – review & editing, supervision, funding acquisition. All authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This work was supported by 2023 Science and Technology Project of Jilin Provincial Department of education (no. JJKH20231226KJ).