
Abstract
Objective
To identify risk factors associated with snakebite severity and determine whether tourniquet use can affect the severity and outcome of snakebites.
Methods
The clinical data of patients who sustained limb snakebites from 1 March 2021 to 31 October 2022 were reviewed. The patients were divided into three groups according to snakebite severity: mild (517 cases), moderate (112 cases), and severe (8 cases). We compared the clinical data of mild versus moderate to severe snakebites. Multivariate logistic regression was used to determine the independent risk factors for moderate to severe snakebites.
Results
The study involved 637 patients. There were statistically significant differences in age, tourniquet use, onset time, white blood cell increase, platelet decrease, creatine kinase (CK) increase, activated partial thromboplastin time shortening, and length of stay between patients with mild snakebites and those with moderate to severe snakebites. Multivariate logistic regression analysis showed that age, tourniquet use, and CK increase were independent risk factors for moderate to severe snakebites.
Conclusion
The overall severity of snakebites in Chongqing is mild, and the prognosis is good. Age, tourniquet use, and CK increase are independent risk factors for the severity of snakebites. We do not recommend tourniquet use after snakebites in Chongqing.
Introduction
Snakebites are a recognized medical problem and common injury, especially in rural areas of tropical developing countries. Their impact on public health has largely been ignored by medical science.1–3 The exact burden of snakebite is difficult to assess, but an estimated 63,400 deaths occurred worldwide in 2019. 4 Millions of snakebites are estimated to occur in China every year. Venomous snakebites account for 100,000 to 300,000 of these cases annually, and the fatality rate is approximately 5%. 5 No epidemiological surveillance and reporting system has been established in China, and the incidence of snakebite is seriously underestimated. 5 The effect of snake venom on the body can be classified as neurotoxic, hemotoxic, cytotoxic, or mixed. 6 The main snake species that causes injuries in Chongqing, China is Trimeresurus mucrosquamatus, which harbors hemotoxic venom.7,8 The main clinical manifestations of T. mucrosquamatus snakebites are swelling of the injured limb and thrombocytopenia secondary to abnormal bleeding and coagulation function.9,10
In on-site self-rescue and pre-hospital first aid, the domestic diagnosis and treatment guidelines still recommend the use of a tourniquet to immobilize the limbs of patients with neurotoxic snakebites. However, excessive and prolonged compression must be avoided to prevent ischemic necrosis of the limb. 5 The latest editions of Chinese medical textbooks suggest that running should be avoided after a snakebite. Additionally, the proximal end of the injured limb should be immediately bound at the scene with a cloth or other object, the tightness of which should be controlled to slightly weaken the arterial pulse of the lower limb. The ligation is then released for 1 to 2 minutes approximately every 30 minutes to avoid adversely affecting the blood circulation and causing tissue necrosis. 11
Application of a tourniquet after a snakebite limits the spread of venom to other parts of the body and delays the onset of systemic toxicity.12,13 However, the use of a tourniquet concentrates the venom in the affected limb, thereby increasing local tissue damage. 14 Moreover, releasing the tourniquet may cause venom flooding, leading to shock, pulmonary embolism, and death. 15 Some clinical practices and guidelines discourage tourniquet use because of uncertain benefits and the potential for worsening local tissue damage.16–20 Therefore, tourniquet use after snakebites remains controversial. The present study was performed to retrospectively analyze the clinical characteristics of patients with limb snakebites, identify related factors affecting the severity of snakebites, and explore the effect of tourniquet use on the severity of snakebites in Chongqing to provide evidence for clinical decision-making.
Methods
Eligibility criteria
This retrospective cohort study was conducted at the Chongqing Emergency Medical Center, a 1200-bed hospital in Chongqing, China. We reviewed the data of patients who were hospitalized for limb snakebites from 1 March 2021 to 31 October 2022. This study was performed in accordance with the ethical requirements in the Declaration of Helsinki and approved by the Ethics Committee of Chongqing Emergency Medical Center. Anonymized data were used in this study, and patients’ individual identities are not disclosed; therefore, the requirement for informed consent was waived. The reporting of this study conforms to the STROBE statement. 21
The inclusion criteria were a confirmed diagnosis of limb snakebite and the completion of laboratory tests during the hospital stay. The exclusion criteria were a history of thrombocytopenia, platelet dysfunction, or coagulopathy and missing data.
Definitions
Tourniquet use
At the time of this study, our institution did not have a specific medical tourniquet for snakebites, and medical staff rarely applied tourniquets to patients with snakebites. Instead, the use of tourniquets was mainly an on-site self-rescue measure after a snakebite; therefore, it was difficult to accurately quantify the pressure of the tourniquet. In this study, tourniquet use was defined as the application of any restraint device (non-standard tourniquet) to the limb for more than 30 minutes after the snakebite; we did not assess the tourniquet binding pressure. The non-tourniquet group comprised patients who sustained limb snakebites and had no restraint applied to the limb.
Snakebite severity
Snakebite severity was graded using the snakebite severity scale, 5 which takes into account the site of injury, systemic symptoms and signs, and laboratory parameters (Table 1). Mild, moderate, and severe snakebites were defined as scores of 0–3, 4–7, and ≥8, respectively. Because the severity of a snakebite has not been precisely defined, the patient’s highest score during treatment was used for severity scoring in this study.
Snakebite severity scale.
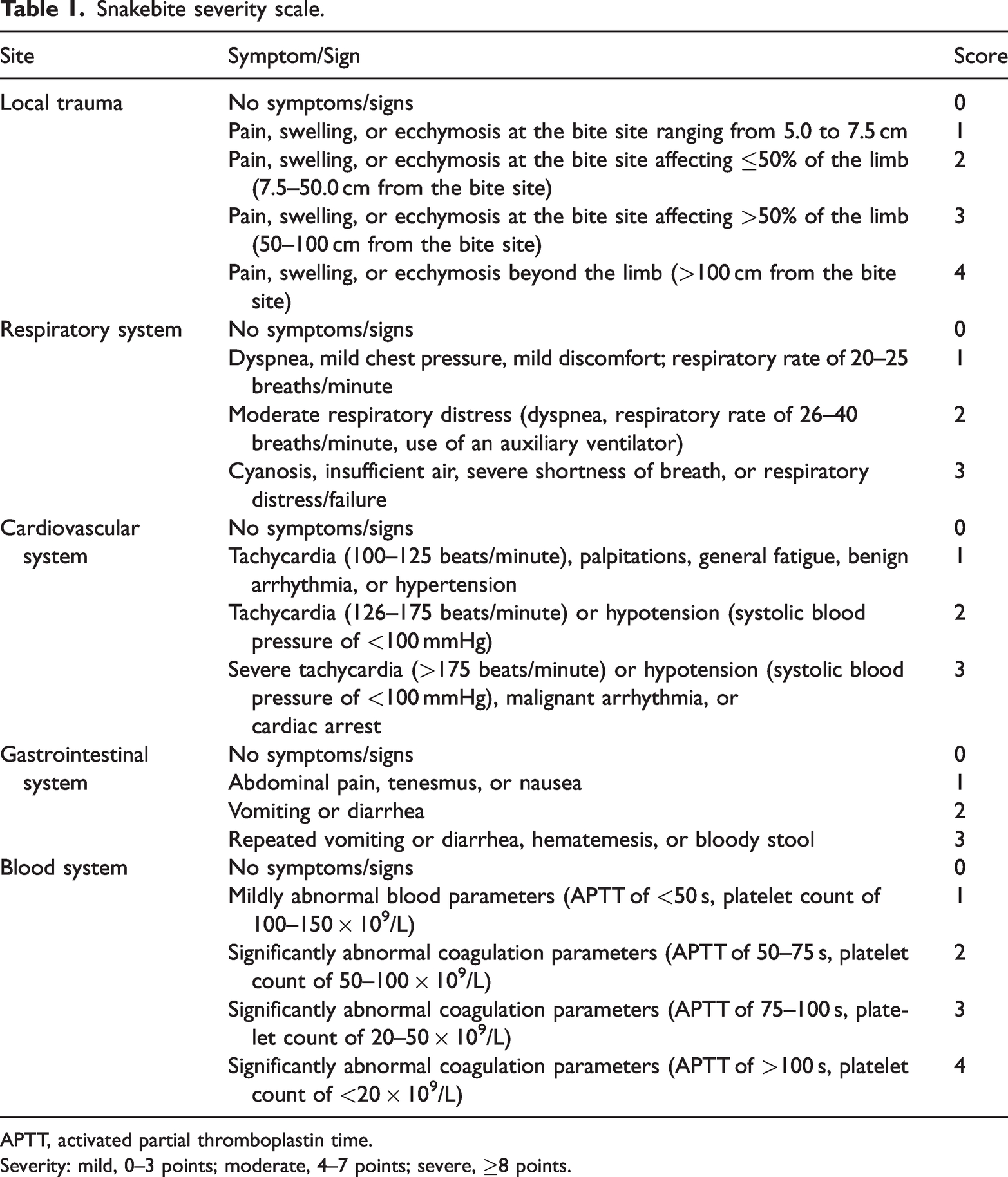
APTT, activated partial thromboplastin time.
Severity: mild, 0–3 points; moderate, 4–7 points; severe, ≥8 points.
Data collection
Data were gathered from the hospital’s electronic medical records and archived patient charts. The following data were collected: demographic characteristics (age, sex, onset time from snakebite to admission, and tourniquet use time from limb restraint to tourniquet release), comorbidities (hypertension and type 2 diabetes mellitus), local wound characteristics (bite site, pain, ecchymosis, and swelling), general condition (vital signs and gastrointestinal symptoms such as pain, nausea, vomiting, diarrhea, and hematemesis or hematochezia), respiratory symptoms (dyspnea, chest tightness, tachypnea, and cyanosis), central nervous system symptoms (headache, weakness, dizziness, chills, and paresthesia), blood indices (white blood cell count, platelet count, creatine kinase (CK) concentration, and activated partial thrombin time), clinical outcome (amputation, mortality, and length of stay (LOS)), therapeutic measures (all patients received standard treatment according to the guidelines for diagnosis and treatment of injuries caused by common animals (2021 edition) established by the National Health Commission), 5 and follow-up (all patients were followed up for >3 months after discharge).
Statistical analysis
SPSS 27.0 software (IBM Corp., Armonk, NY, USA) was used to analyze the data. Continuous numerical variables are expressed as mean ± standard deviation, and one-way analysis of variance was used to compare normally distributed data. Data with a skewed distribution are presented as median and interquartile range and were compared using the Mann–Whitney U test. Categorical variables are expressed as the number and percentage of cases and were analyzed with the chi-square test or Fisher’s exact test. Multivariate logistic regression analysis was used to determine the independent risk factors for moderate to severe snakebite. A P value of <0.05 was considered statistically significant.
Results
Clinical characteristics of all patients with snakebites
In total, 637 patients were enrolled after application of the inclusion and exclusion criteria (Figure 1). They comprised 394 men and 243 women with a mean age of 55.1 ± 15.7 years. The main region in which the snakebites occurred was the lower limb, and the foot was the most common site. According to the snakebite severity scale, the patients were divided into three groups: those with mild (517 cases, 81.2%), moderate (112 cases, 17.6%), and severe snakebites (8 cases, 1.2%). Because of the small number of patients with severe snakebites, the patients were divided into two groups for the statistical analysis (mild vs. moderate to severe).

Study flow chart.
Clinical characteristics of patients with mild versus moderate to severe snakebites
All patients had a small amount of bleeding and ecchymosis at the bite site on admission with different degrees of pain and swelling of the injured limb. Some patients had nausea, vomiting, tachycardia, and other symptoms after the snakebite. The comparative analysis showed significant differences in age, tourniquet use, tourniquet use time, onset time, blood parameters at admission (white blood cell count, platelet count, CK concentration, and activated partial thromboplastin time), and LOS between the two groups (P < 0.05). There were no significant differences in sex, bite site, or comorbidities between the two groups. The moderate to severe snakebite group had a higher rate of abnormal blood parameters and tourniquet use, a higher proportion of tourniquet use time of >1 hour, and a longer LOS (Table 2).
Clinical characteristics of patients with mild versus moderate to severe snakebites.

Data are presented as mean ± standard deviation, n (%), or median (interquartile range).
WBC, white blood cell; PLT, platelet; CK, creatine kinase; APTT, activated partial thrombin time.
Independent risk factors for moderate to severe snakebites
The results of the univariate analysis of moderate to severe snakebites are shown in Table 3. These variables were included in the multivariate analysis. Table 4 shows the results of the multivariate analysis for moderate to severe snakebites. Age (odds ratio (OR), 1.018; 95% confidence interval (CI), 1.001–1.034; P = 0.034), tourniquet use (OR, 9.584; 95% CI, 5.702–16.108; P < 0.001), and an increase in the CK concentration (OR, 3.051; 95% CI, 1.865–4.991; P < 0.001) were identified as independent risk factors for moderate to severe snakebites.
Univariate analysis of risk factors for moderate to severe snakebites.

OR, odds ratio; CI, confidence interval; WBC, white blood cell; CK, creatine kinase.
Multivariate regression analysis of risk factors for moderate to severe snakebites.

OR, odds ratio; CI, confidence interval; WBC, white blood cell; CK, creatine kinase.
Clinical outcomes
Amputation
One patient with a severe snakebite underwent amputation because of limb ischemia and necrosis caused by strapping the lower leg with nylon rope for 4 hours after the snakebite.
Mortality
No multiple organ failure, major bleeding, or death occurred in any patients. The eight patients with severe snakebites mainly had severe secondary thrombocytopenia (platelet count of <20 × 109/L).
LOS
Patients with moderate to severe snakebites had a longer LOS than patients with mild snakebites.
Discussion
In this study, we found that the independent risk factors affecting the severity of snakebites in Chongqing were age, tourniquet use, and an increase in the CK concentration. Some studies have identified an association between age and adverse outcomes after snakebites. One study analyzed the risk factors for snakebite-induced acute kidney injury (AKI) to provide guidance for the prevention and early treatment of AKI. The multivariate logistic regression analysis showed that age may be an independent risk factor for snakebite-induced AKI. 22 Another study analyzed risk factors associated with acute liver injury after Agkistrodon snakebite in Nanchang, China. The multivariate logistic regression analysis showed that age was an independent risk factor for acute liver injury after Agkistrodon bites. 23 Some studies have suggested that age is not associated with snakebite severity or mortality. One study analyzed the influencing factors of the severity of T. stejnegeri snakebites in patients who first visit the hospital. Six independent variables were included in the logistic regression equation: age, underlying diseases, injury season, length of time to arrival at the hospital after the bite, proximal limb ligation, and wound irrigation. The authors concluded that age was not a risk factor for the severity of the patient’s condition on admission. 24 A retrospective study in a rural tertiary care hospital in central India was performed to determine which risk factors on admission were associated with in-hospital mortality after snakebite envenomation, and the results showed that age was not a significant predictor of mortality in hospitalized patients with snakebites. 25 The influence of age on the severity and adverse outcomes of snakebites remains controversial and requires more clinical studies.
A prospective study in the Philippines revealed the effect of tourniquet application on 36 hospitalized patients with neurotoxic symptoms after being bitten by a Filipino cobra. This study showed that tourniquet application delayed the onset of symptoms in 94% of patients. Four patients developed complete respiratory paralysis during tourniquet removal and required artificial ventilation. Therefore, the authors recommended the use of tourniquets in the Philippines only after a cobra bite had been established and in cases in which the tourniquet could be removed under controlled hospital conditions. 26 In one study of tourniquet use among 37 patients with Russell’s viper bites, venom antigen levels were measured by enzyme-linked immunosorbent assay in the proximal and distal ends of the tourniquet and in venous samples before and after tourniquet release to determine whether these ligations delayed venom movement from the bite site. The results showed that in most patients (29/37), the tourniquet did not prevent or sufficiently delay the spread of venom from the bite site. However, the presence of venom antigens in 8 of 37 patients suggests that some tourniquets may limit systemic uptake of venom, thereby delaying the onset of severe symptoms. Therefore, it cannot be concluded that tourniquets are completely useless. 27 Many authors have recommended that tourniquets should not be used in patients with snakebites because of the risk of aggravating local complications and the development of tissue ischemia and gangrene.28–33 A Brazilian study comparing the clinical and laboratory data of patients with and without a tourniquet after a Crotalus durissus bite showed that tourniquet use in the field was ineffective in reducing the severity of C. durissus injuries, and new strategies are recommended to persuade people not to use a tourniquet in Brazil. 28 In a case report from Benue Valley, Nigeria, inappropriate application of a tourniquet after a bite from a viper snake triggered local complications leading to death. 29 Venom is associated with local necrosis, which may be enhanced by the obstruction of venous return and lymphatic flow. Therefore, tourniquets are not recommended in first aid for snakebites. 29 An overview of systematic reviews identified several important findings regarding tourniquet treatment for snakebites. 19 There were no significant differences in the occurrence of acute renal failure, acute respiratory failure, hemorrhagic syndrome, multiple organ dysfunction syndrome, death, or disability between patients treated with a tourniquet and patients who received no tourniquet or first aid. No multiple organ failure, massive bleeding, or death occurred in any patients in the present study, suggesting that the overall prognosis of snakebites in Chongqing and surrounding areas is good. This is consistent with the results of an epidemiological survey of snakebites in Chongqing. 8 The multivariate logistic regression analysis in the present study showed that tourniquet use was an independent risk factor for moderate to severe snakebites, indicating that tourniquet use may increase the severity of snakebites. One patient in our study developed ischemic necrosis and underwent amputation because of prolonged strapping of the limb with a tourniquet, suggesting that inappropriate first aid measures may cause more damage than the snake envenomation itself.
CK is a biochemical marker of rhabdomyolysis, and an increased CK concentration may be an indicator of cell necrosis or tissue damage after acute and chronic muscle injury. 34 Both limb snakebites and tourniquet application may cause muscle damage and increase the CK concentration.35,36 One study analyzed the risk factors for snakebite-induced AKI and showed significant differences between the AKI and non-AKI groups in age, time interval from snakebite to antivenin therapy, CK concentration, blood myoglobin concentration, advanced age, regional lymphadenopathy, incision drainage, and hemoglobin concentration. High CK is considered a risk factor for snakebite-induced AKI. 22 Our multivariate regression analysis showed that an increased CK concentration was an independent risk factor for moderate to severe snakebite, suggesting that patients with an increased CK concentration at admission may have a more severe condition and a worse prognosis. More studies are needed to clarify the effect of an increased CK at admission on the severity and adverse outcomes of snakebites.
Our study revealed certain findings regarding the field management of snakebites in Chongqing. First, age, tourniquet use, and increased CK were independent risk factors for the severity of snakebites. Second, the overall severity of snakebites was mild (81.2%), and the prognosis was good. Third, the use of a tourniquet in self-rescue at the scene after snakebites may increase the severity of snakebites and even increase the risk of serious complications (limb ischemia and necrosis). In China, people’s understanding of the use of tourniquets after snakebites comes from the recommendations in diagnosis and treatment guidelines and books.5,11 The clinical manifestations and severity of venomous snakebites vary with the distribution of venomous snake species in different regions, 6 making it necessary to adopt targeted prevention and control strategies based on the epidemiological survey results of snakebites in different regions. Community education on snakebites and training in first aid skills should also be strengthened so that people know when emergency hospitalization is needed and unnecessary interventions can be avoided.
Limitations
Our study has several limitations. First, this was a retrospective study, and some data were incompletely recorded, such as the exact timing of limb binding. Second, the tourniquets described in this paper were not all the same type of tourniquet, and the tying pressure of the tourniquet was difficult to estimate, resulting in the inability to unify the criteria. Third, the content of snake venom could not be detected. Radioimmunoassay, agglutination assay, enzyme-linked immunosorbent assay, and fluoroimmunoassay have been used to detect the content of snake venom. 37 In subsequent studies, we will determine the content of venom, refine the exact timing of binding, and stratify patients.
Conclusion
The independent risk factors affecting the severity of snakebite in Chongqing are age, tourniquet use, and CK concentration. Early identification of these risk factors and active treatment measures may help to improve the prognosis of patients with snakebites. The overall severity of snakebites is mild and the prognosis is good. Using a tourniquet during self-rescue at the scene after a snakebite may aggravate the severity of the bite, increase the risk of moderate to severe snakebite, and even increase the risk of serious complications. Therefore, to prevent unnecessary injury caused by tourniquet use, we do not recommend tourniquet use after snakebites in Chongqing.
Footnotes
Author contributions
Study design: Qian Yang. Data collection: Qian Yang, Yunhan Gao, Weijie Fu, and Shaying Ma. Data analysis: Qian Yang, Yunhan Gao, and Weijie Fu. Manuscript preparation: Qian Yang. Critical revision: Qian Yang, Yunhan Gao, and Weijie Fu.
Data availability statement
All data are available on request from the corresponding author.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.