
Abstract
Extramedullary hematopoiesis (EMH) is a rare condition characterized by proliferation of hematopoietic stem cells outside the bone marrow, usually as a compensatory response to hematological disease. Although EMH primarily occurs in the liver and spleen, it can manifest in atypical locations, such as the mediastinum. We herein describe an asymptomatic 66-year-old man with incidentally discovered posterior mediastinal EMH. A 28- × 32-mm mass was detected during a routine examination. Laboratory findings were within normal limits. Computed tomography revealed a well-defined enhancing mass with a density of 60 Hounsfield units, suggestive of a neurogenic tumor. Surgical resection confirmed EMH, characterized by megakaryocytes and hematopoietic precursors. The patient recovered smoothly and was discharged 5 days postoperatively. Accurate preoperative diagnosis of EMH is challenging, as illustrated by this case. Although typically associated with anemia or hematological abnormalities, EMH can present without such signs. Surgical resection and histopathological examination are essential for diagnosis. This case emphasizes the diagnostic complexity of posterior mediastinal EMH, even in patients without overt hematological disorders. Posterior mediastinal EMH is exceedingly rare and diagnostically demanding. A high index of suspicion and histological tissue analysis are crucial for optimal management. Video-assisted thoracoscopic surgery enables both diagnosis and treatment through mass excision.
Keywords
Introduction
Extramedullary hematopoiesis (EMH) is a compensatory response to severe anemia and is often secondary to chronic hemolytic anemia or ineffective hematopoiesis. Although the spleen and liver are the most common sites for the occurrence of EMH,1,2 isolated cases in the posterior mediastinum are also rarely encountered. Because of the lack of specificity in clinical manifestations and imaging characteristics, EMH is often misdiagnosed as a neurogenic tumor. Video-assisted thoracoscopic surgery (VATS) can be beneficial in differentiating these tumors.
This case report fills an important knowledge gap regarding the clinical presentation and management of EMH in mediastinal tumors. This unique case is difficult to differentiate from other mediastinal tumors and thus enhances physicians’ understanding that mediastinal tumors can also involve EMH. The insights gained from this case will assist physicians in making informed decisions and formulating tailored treatment strategies for similar cases in the future.
Case presentation
We herein describe a 66-year-old man who sought medical evaluation because of the incidental discovery of a posterior mediastinal mass during a routine physical examination 2 years previously. When the mass was discovered, the patient had been entirely asymptomatic with no complaints of pain, dyspnea, or systemic symptoms. Importantly, he had no history of chronic illnesses or hematological disorders.
Upon the initial discovery, the patient’s primary care physician ordered a series of laboratory investigations to assess the patient’s overall health and investigate the nature of the mass. A complete blood count showed a slightly elevated red blood cell count and hemoglobin level followed by a slight decrease, with the majority of values within the normal range (Figure 1). This absence of hematological abnormalities presented a significant diagnostic challenge because EMH is typically associated with underlying hematological conditions characterized by compromised hematopoiesis.

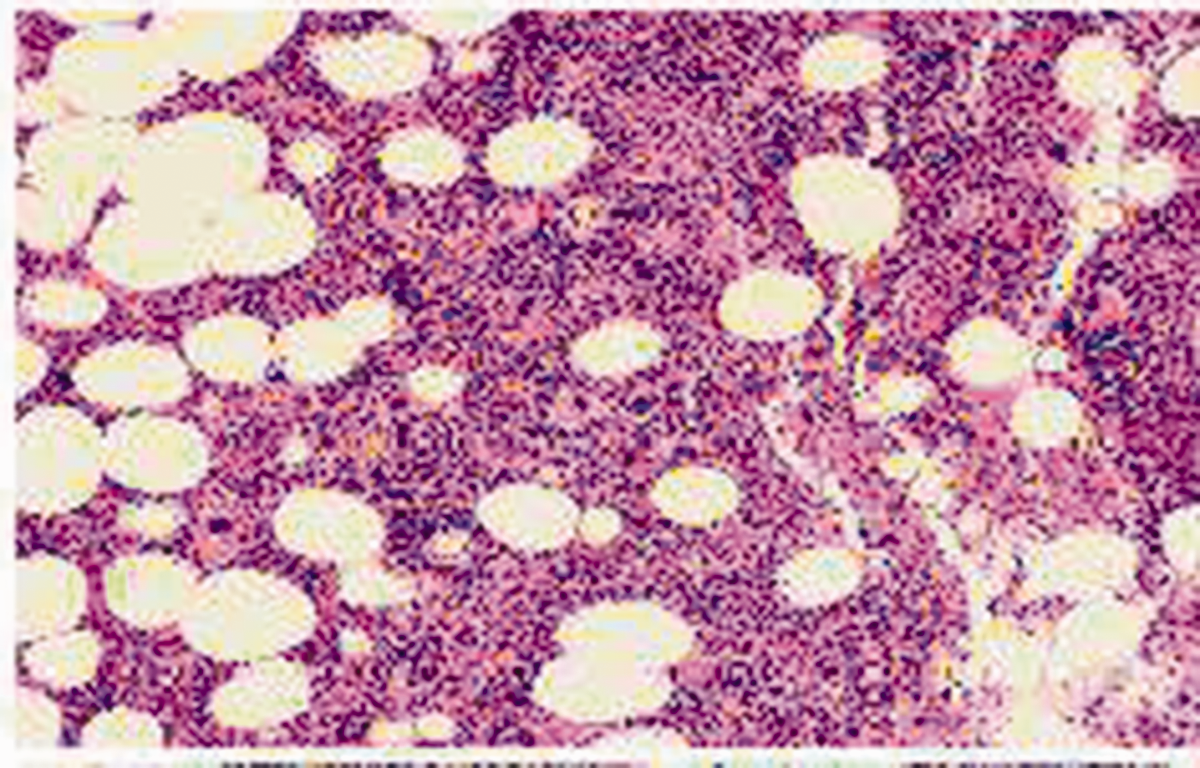
Histopathological studies showed that the tumor tissue consisted of hematopoietic cells including megakaryocytes, erythroid precursors, and myeloid precursors.
The patient’s uneventful medical history added to the complexity of the clinical presentation. He had experienced no recent illnesses, infections, or significant life events that might have triggered hematopoietic responses. He had no history of blood transfusions, which are often associated with iron overload and the subsequent development of EMH as a compensatory mechanism. Moreover, he had no known familial hematological disorders, adding to the diagnostic challenge of the posterior mediastinal mass.
Intriguingly, the patient had remained asymptomatic throughout the 2-year interval since the initial discovery of the mass. He reported no symptoms such as chest pain, dysphagia, or cough and no constitutional symptoms such as fever, night sweats, or weight loss. The absence of these clinical manifestations further obscured the diagnosis because such symptoms often develop in patients with posterior mediastinal masses, especially when the mass exerts pressure on surrounding structures or invades nearby tissues.
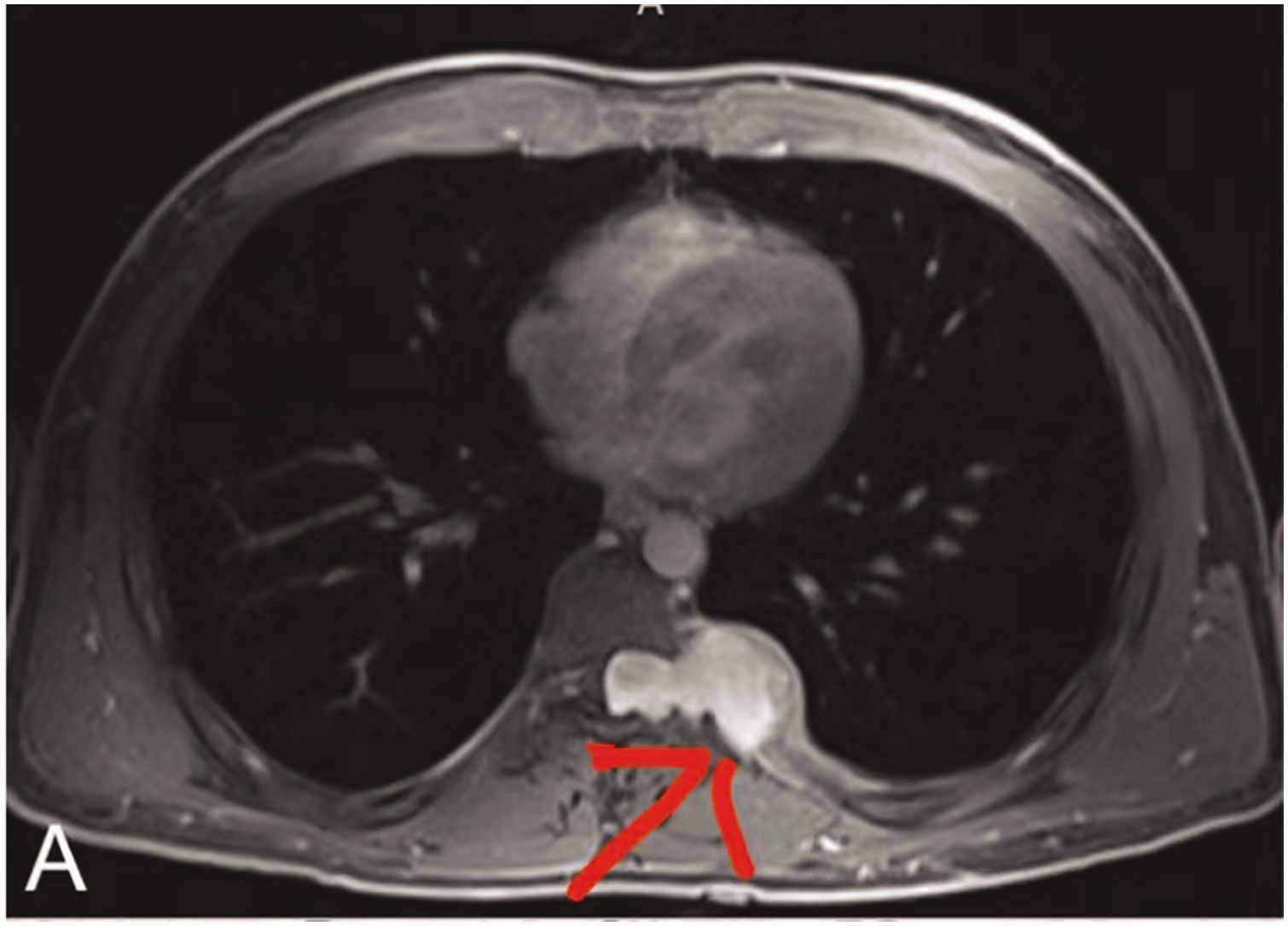
The physical examination findings were similarly unremarkable. Palpation of the chest wall revealed no palpable masses, tenderness, or crepitus indicative of subcutaneous emphysema. The patient’s breath sounds were clear, and there were no audible murmurs or bruits on auscultation. Additionally, no lymphadenopathy was appreciated on examination of the cervical, axillary, or supraclavicular lymph nodes. Given the patient’s asymptomatic state and absence of hematological aberrations, we initially decided to monitor the progression of the posterior mediastinal mass. Subsequent imaging was deemed necessary to further investigate the nature and location of the mass. Radiological investigations were conducted to provide insight into the characteristics of the mass. Contrast-enhanced computed tomography (CT) of the chest was performed to delineate the size, location, and radiological features of the mass. The CT scan revealed a well-defined, homogenously enhancing mass of soft tissue density measuring 28 × 32 mm. This mass was situated in the right paravertebral region, closely adjacent to the 10th thoracic vertebra. The density of the mass on CT imaging was approximately 60 Hounsfield units, indicating that it had a solid composition (Figure 2).

Slightly elevated red blood cell count and hemoglobin level followed by a slight decrease, with the majority of values within the normal range.
The radiological findings were intriguing but lacked specificity. Although the mass was clearly delineated, its appearance was not pathognomonic, making it difficult to ascertain the underlying pathology based solely on imaging. Consequently, given the location and radiological characteristics of the mass, the initial differential diagnoses primarily included benign neurogenic tumors such as schwannomas or neurofibromas.
The patient’s medical history, clinical presentation, and radiological findings posed a significant diagnostic challenge. The absence of symptoms, hematological abnormalities, or a clear etiological factor for the posterior mediastinal mass complicated the diagnostic process. In light of these uncertainties, the medical team decided to pursue the more definitive approach of resecting the mass by single-port VATS under general anesthesia. This decision was driven by the dual objectives of achieving a definitive diagnosis and, if warranted, providing therapeutic intervention.
The surgical procedure was conducted without complications. Intraoperative examination revealed that the mass was encapsulated and highly vascular, which are unexpected characteristics in the context of a benign neurogenic tumor. On gross examination, the excised mass was red in color.
We next performed a comprehensive histopathological analysis, including immunohistochemical staining. This analysis was indispensable for achieving an accurate diagnosis and understanding the nature of the mass. We expected that the results of these histological investigations would provide critical insights into whether the mass represented EMH, which, despite its rarity, could not be ruled out given the enigmatic clinical presentation.
Microscopic examination of the tissue specimen revealed a complex landscape of hematopoietic elements within the mass. Megakaryocytes and hematopoietic cell precursors were readily identifiable, consistent with the presence of EMH. These initial histological findings provided valuable diagnostic clarity, and the immunohistochemical analysis further corroborated the diagnosis. The results of the immunohistochemical staining reinforced the identification of the mass as a site of EMH. Specific markers for hematopoietic cell populations, including megakaryocytes, erythroid precursors, and myeloid precursors, were expressed within the mass. These findings collectively established the diagnosis of posterior mediastinal EMH (Figure 3).
Contrast-enhanced computed tomography examination of the chest revealed a lateral mass (60 HU) measuring 28 × 32 mm on the right side of the 10th thoracic vertebra of the posterior mediastinum.
The patient was discharged from the hospital 5 days postoperatively and had fully recovered 1 week later. For 2 years, he did not return to the hospital for further treatment. The reporting of this study conforms to the CARE guidelines. 3 Ethics committee approval was not required because of the nature of this study (case report). Written informed consent for publication of this case report was obtained from the patient. Prior to the study, patient consent for treatment was obtained.
Discussion
EMH refers to the hematopoietic process that occurs outside the bone marrow and serves as a compensatory mechanism for insufficient red blood cell production. It is most common in patients with chronic hemolytic anemia, 4 especially those with transfusion-independent thalassemia intermedia.5,6 Ineffective erythropoiesis from the bone marrow forces extramedullary hematopoietic tissue to expand, leading to compensatory hematopoiesis in other areas of the body, often in the form of masses. 7 EMH is commonly observed in the liver, spleen, and lymph nodes; however, cases involving the mediastinum are rare. Studies have shown that 11% to 15% of patients with EMH have involvement of the hematopoietic tissue adjacent to the spine, with the thoracic and lumbar regions being the most frequently affected sites. 8 The reason for this predominance is uncertain, but these regions are thought to be actively involved in fetal hematopoiesis during pregnancy. Although this pathway typically ceases after birth, extramedullary hematopoietic vascular connective tissue retains the ability to produce red blood cells in cases of prolonged ineffective erythropoiesis. 8
Accurate diagnosis of EMH can be challenging, particularly when patients have no relevant history of hematological disorders. The paraspinal region is a common site of EMH, with most paravertebral masses being asymptomatic. Imaging techniques such as chest CT and magnetic resonance imaging can assist in diagnosis, with the latter being the preferred diagnostic modality. Paraspinal EMH presents as multiple lobulated or well-defined masses with intermediate signal intensity on T1-weighted images and low signal intensity on T2-weighted images.9,10 CT features include heterogeneous masses of soft tissue density. Two previous reports described the imaging characteristics of EMH.11,12 Although EMH has no specific imaging findings in most imaging examinations, the involvement of multiple sites or the presence of visible fat on gross or microscopic examination can be helpful, especially in patients with known risk factors such as myelofibrosis. Neurogenic tumors reportedly exhibit the following two characteristics: First, they form a dumbbell-shaped mass within the neural foramina, which can be distinguished radiologically. Second, neurofibromas are histologically characterized by strong, uniform expression of the S100 protein, which is a useful diagnostic feature 13 (Figure 4). Diagnosis of nonspecific soft tissue masses usually requires biopsy. The most common presentation of EMH as a mass lesion is multiple fat-containing lesions localized to the axial skeleton. Although more commonly found in the posterior mediastinum, EMH can also involve the nervous system. EMH mass lesions are typical vascular tumors, and bleeding complications should be considered during biopsy. The diagnosis of EMH should be strongly considered when these features are present during surgery or imaging.
Dumbbell-shaped structure.
There is no unified evidence-based medical standard for the treatment of EMH. Research has suggested that low-dose radiotherapy can be used as a treatment option for patients with EMH; sclerosing agents are not recommended.14–17 The treatment of EMH outside the mediastinum depends on the presence of symptoms, and modalities include transfusion, radiotherapy, hydroxyurea therapy, or selective surgical excision. Before evaluating the effectiveness and safety of existing treatment options in large-scale prospective trials, a personalized approach should be designed for both single and combination therapies. Surgical excision of the mass is required for confirmation through pathological examination. 18 Given the rarity of EMH, there are no standardized treatment approaches for symptomatic patients and no evidence-based guidelines for managing EMH. Treatment typically depends on the severity of symptoms, size of the mass, patient’s clinical condition, and previous treatments. Various treatment options have been described, including transfusion therapy, laminectomy, radiation therapy, and the use of hydroxyurea as a hematopoietic suppressive agent. However, the ideal management strategy remains controversial, and an individualized approach should be designed until large-scale prospective trials can be performed to assess the effectiveness and safety of existing treatment regimens. 19
In summary, the clinical and radiographic features of EMH lack specificity, making preoperative diagnosis challenging. It is often misdiagnosed as a neurogenic tumor, lung cancer, or spinal tuberculosis. Definitive diagnosis relies on postoperative pathological examination. This case highlights the importance of considering EMH in patients with posterior mediastinal masses with similar CT findings.
Footnotes
Acknowledgements
We thank the patient for his cooperation in the publication of this case report. We also appreciate the instructions by the clinical teachers.
We acknowledge that we have not previously published in this specific area. However, we have extensive expertise in related fields, including esophageal cancer, mediastinal diseases, and lung cancer. Our research and experience have provided us with a strong foundation to contribute to this area.
Data availability statement
Data are available only upon request because of privacy/ethical restrictions.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This study was not funded by any company, non-profit, or governmental agency.