
Abstract
Colon cancer in patients with situs inversus totalis is rarely associated with dextrocardia, and chemotherapy is commonly used for treatment. Central venous access devices are used to administer intravenous fluids and chemotherapy in patients with colon cancer. Compared with peripherally inserted central catheters and Hickman-type tunneled catheters, totally implantable vascular access devices (TIVADs) are safer and more effective. However, positioning the catheter tip may be challenging in patients with dextrocardia and situs inversus. We herein describe a novel case involving a patient with dextrocardia and colon cancer who was treated by TIVAD insertion with intracavitary electrocardiography-aided tip localization.
Keywords
Introduction
Dextrocardia, a rare congenital anomaly, is defined as the malpositioning of the heart in the thoracic cavity. Placement of a totally implantable vascular access device (TIVAD) assisted by electrocardiography (ECG)-guided positioning technology in patients with dextrocardia is challenging. We herein present a novel case of ECG-aided tip localization of a TIVAD in a patient with colon cancer, dextrocardia, and situs inversus. The patient successfully underwent TIVAD placement in the left chest wall. Under ultrasound guidance, a central catheter connected to the infusion port was also inserted into the left internal jugular vein beneath the skin. In this report, we discuss the clinical features, ECG characteristics, and location of the catheter tip in this patient. The catheter tip was placed in the superior vena cava, and chest radiographs showed that it was located at the lower border of the T7 vertebra. The distance from the tracheal carina to the catheter tip was 3.01 cm, suggesting that the TIVAD catheter tip was positioned appropriately. 1 The patient developed no surgery-related complications.
Case report
A nearly 60-year-old woman was admitted to the hospital because of a 1-month history of repeated left lower abdominal quadrant pain. She had a history of hypertension and regularly took 2.5-mg levamlodipine once daily to control her blood pressure. A thoracoabdominal computed tomography (CT) scan revealed dextrocardia with situs inversus (Figure 1(a)–(c)), and echocardiography revealed dextrocardia with no atrial septal defect, no ventricular septal defect, and a normal left ventricular ejection fraction. We connected the ECG leads using the conventional method, and the I and aVL limb leads showed negative P-QRS-T waves and ST-T segment changes. Lead reversal ECG (limb and chest leads placed in a mirror location) showed normal sinus rhythm, ST-T segment changes, and positive P-QRS-T waves. Pathological examination revealed colon adenocarcinoma with hepatic metastasis. Laboratory test results were normal, including a complete blood count and measurement of serum electrolytes, myocardial enzymes, the creatinine concentration, liver function, and coagulation function. The patient’s vital signs were as follows: body temperature, 36.2°C; pulse, 67 beats/minute; blood pressure, 145/100 mmHg; respiratory rate, 20 breaths/minute; and oxygen saturation, 97% on room air.

Thoracic/abdominal CT examination suggested dextrocardia with situs inversus. (a) Chest CT showed a right-sided heart. (b) Chest CT revealed a left-sided superior vena cava (red arrow) and (c) Abdominal CT showed a right-sided spleen and a left-sided liver.
The patient was assessed before chemotherapy, and no contraindications to chemotherapy were identified. According to the tumor characteristics and disease stage, the patient received a biweekly schedule of fluorouracil, leucovorin, and oxaliplatin (FOLFOX) chemotherapy. A long-term central venous access device was placed during systemic anticancer treatment to protect the blood vessels, decrease the risk of infection, and reduce drug extravasation. TIVADs are safer and more effective than peripherally inserted central catheters and Hickman-type tunneled catheters.2,3 After providing written informed consent for TIVAD implantation (Smiths Medical ASD, Minneapolis, MN, USA), the patient was placed in the supine position. The ECG monitor was connected using limb lead II to provide long-term, continuous, and real-time ECG information. The limb leads were then placed in the mirror location, and the P-wave morphology appeared identical whereas the QRS complex presented an Rs shape. After routine disinfection and draping of towels, a local anesthetic (2% lidocaine, 2 mL) was administered for local infiltration anesthesia. The operator punctured the left internal jugular vein under ultrasonographic guidance and inserted a guide wire. The ultrasound confirmed that the guide wire was located in the internal jugular vein. A small skin incision (0.5 cm) was then made around the guide. The catheter was placed in the punctured vein after dilatation of the access site and connected to a needle on a syringe filled with heparinized saline (50 U/mL). Then, one end of a sterile metal clip was connected to a needle on a syringe, and the other end of the metal clip was connected to an intracavitary ECG lead wire. Body surface and intracavitary ECG signals were recorded simultaneously using the ECG monitor (Figure 2). The P-wave is at its highest point when the catheter tip approaches the cavoatrial junction. 4 The ideal tip position was pulled back by 1 cm from the catheter when the P-wave in the II-lead ECG was at its highest point. After establishment of anesthesia with lidocaine, the left chest wall was surgically opened, and a pocket of subcutaneous tissue for the port chamber was created. The catheter was then tunneled from the puncture point and attached to a port device. The skin was closed with 4-0 absorbable suture (continuous pattern) after placing the port device in the pocket. Chest radiography was performed 4 hours after the procedure, confirming that the catheter tip was located inside the superior vena cava and lower margin of the seventh thoracic vertebra and that the distance from the tracheal carina was 3.01 cm (Figure 3). The reporting of this study conforms to the CARE guidelines. 5

Real-time lead II signals of body surface ECG and intracavitary ECG. Intracavitary ECG indicated that the P-wave reached its highest point when the catheter tip approached the cavoatrial junction.
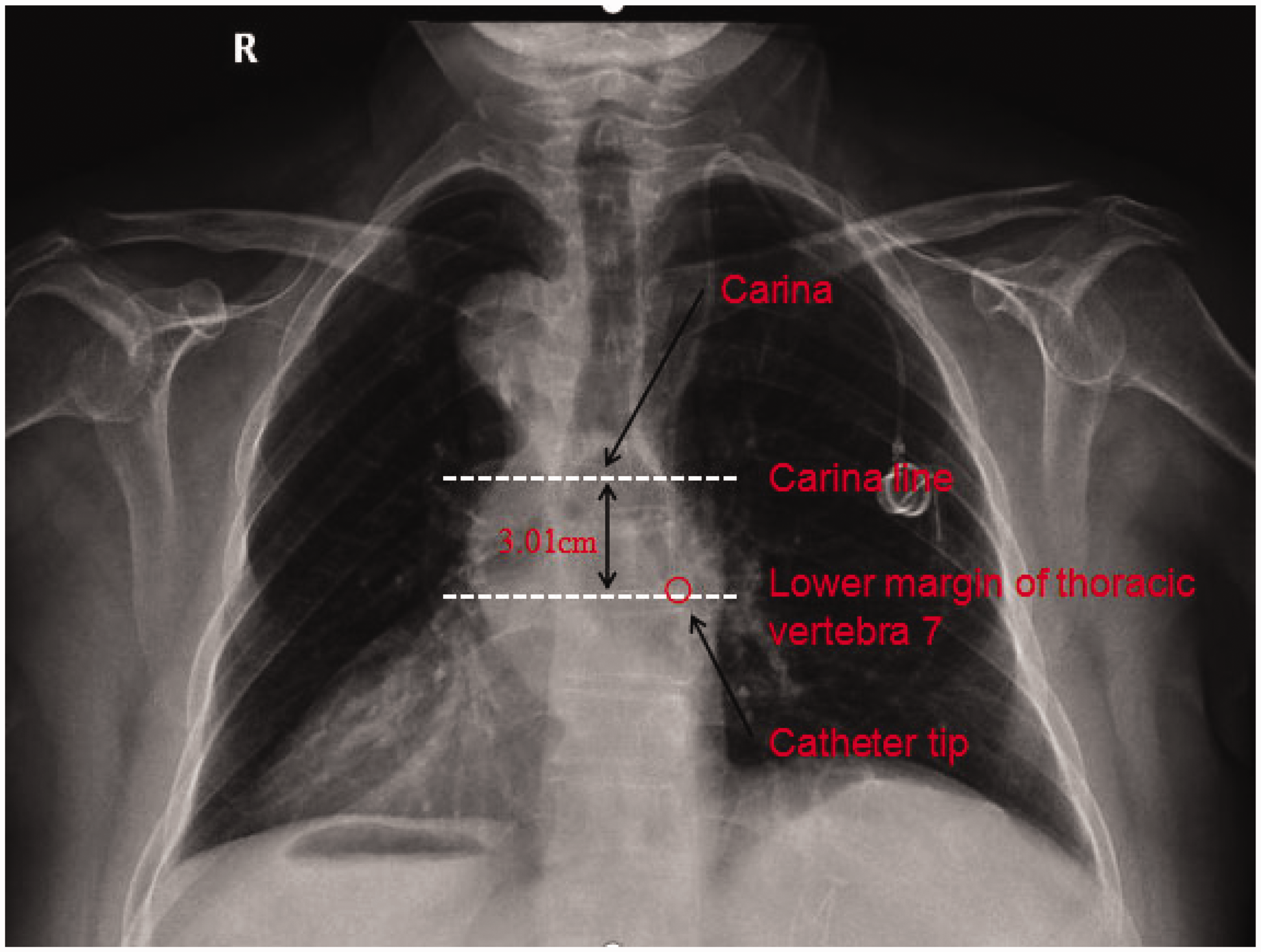
The catheter tip was observed at the ideal location in the chest radiograph (the lower margin of the seventh thoracic vertebra and 3.01 cm below the tracheal carina).
Discussion
Dextrocardia with situs inversus is a rare congenital anomaly, and previous studies have demonstrated that the incidence rate of dextrocardia is approximately 1 in 10,000. 6 The pathogenesis of dextrocardia remains largely unknown. Some scholars believe that dextrocardia is an inherited disorder caused by autosomal recessive mutations, 7 whereas others believe that dextrocardia is caused by malrotation during embryological development. 8 Congenital dextrocardia may be roughly classified into a right-sided heart with complete situs inversus and dextrocardia with situs solitus. 9 We have herein reported a rare case of complete mirror-image transposition of the thoracic and abdominal viscera. The patient presented with situs inversus totalis, which is a mirror-image transposition of the abdominal and thoracic viscera.
Intracavitary ECG has been extensively used for venous infusion port tip positioning in the clinical setting. 10 ECG-guided catheter tip placement for TIVAD implantation is more convenient, safer, and more accurate than the standard fluoroscopy method.10,11 However, little information is available regarding the use of ECG for TIVAD placement in patients with mirror dextrocardia. Implantation of pacemakers or peripherally inserted central catheters in such patients remains challenging because of the complex spatial orientation of the atrium and vascular accesses.12,13
In this clinical case, preoperative chest CT showed that the superior vena cava lay to the left of the mid-vertebral line with dextrocardia, and echocardiography revealed mirror dextrocardia without other congenital heart defects or structural cardiac abnormalities. The left internal jugular vein was selected for catheterization based on the presence of mirror dextrocardia and the morphology of the left superior vena cava. Currently, the most common catheter tip positioning technologies include ultrasound-based intraoperative radiography and intracavitary ECG localization. ECG localization is a convenient, accurate, and safe technique that has recently been widely explored. 11 Leads placed in a mirror location may provide reliable ECG data for patients with dextrocardia. 14 In the present case, the ideal position of the catheter tip was discovered by reversing lead II of the intracavitary ECG. Post-procedure chest radiography revealed that the tip of the catheter was positioned in the inferior vena cava and located 3.01 cm below the tracheal carina. A small amount of blood was withdrawn to verify catheter patency. After surgery, the patient’s vital signs were stable, and she developed no complications.
Conclusion
Patients with dextrocardia and colon cancer are not commonly encountered in the clinical setting, and cases of TIVAD implantation in these patients are even rarer. In this case, chest CT and echocardiography were performed to evaluate the anatomy of the superior vena cava and cardiac tissue before TIVAD implantation. The choice of the most appropriate puncture site is based on the anatomical morphology of the superior vena cava. The catheter tip was positioned according to the morphology of the P-waves on reverse lead II ECG. Subsequent chest X-ray confirmed the accuracy of the catheter tip position. This case report demonstrates that ECG-guided catheter tip placement for TIVAD implantation in patients with dextrocardia and colon cancer is accurate and safe.
Footnotes
Acknowledgment
We are grateful to the patient for providing detailed information.
Author contributions
All authors contributed to the writing and revision of the manuscript. Writing of the original draft: Mingyan Dong. Writing, review, and editing: Mingyan Dong, Lihui Huang, Qiaohong Zhang, Yicui Piao, Zijie Liu, Shuchen Zhu, and Haiguan Luo.
Consent
The patient provided written informed consent before TIVAD insertion. The detailed information of the patient has been de-identified; therefore, the patient’s written consent for publication was not required.
Declaration of conflicting interests
The authors have no conflicts of interest to disclose.
Data availability statement
Data from this report are available on request from the corresponding author.
Ethics approval
The requirement for informed consent was waived because of the nature of this study (case report).
Funding
The publication of this article was supported by Shenzhen High-level Hospital Construction Fund.