
Abstract
Objectives
The clinical course of coronavirus disease 2019 (COVID-19) infection is often aggressive, with unfavorable outcomes for those with comorbidities such as type 2 diabetes mellitus (T2DM). We aimed to assess the prevalence and risk factors of COVID-19 infection, mortality, and post-infection lung fibrosis in patients with COVID-19 infection who had T2DM.
Methods
In this cross-sectional study, we included adult patients with T2DM who attended an endocrinology clinic and underwent testing for COVID-19 infection.
Results
Among 1039 included patients, the mean age was 59.5 ± 11.0 years and 429 (41.3%) were men. Overall, 87.1% of patients had received COVID-19 vaccination and 32.3% had confirmed COVID-19 infection. The COVID-19-related mortality was 3.0% and rate of post-COVID-19 lung fibrosis was 19.1%. Vaccination was associated with lower COVID-19-related mortality (odds ratio [OR]: 0.03, 95% confidence interval [CI]: 0.0–0.3) and post-COVID-19 lung fibrosis risk (OR: 0.3, 95% CI: 0.1–0.9).
Conclusion
Patients with T2DM exhibited a high prevalence of COVID-19 infection and associated mortality. However, COVID-19 vaccines were beneficial in reducing the risks of COVID-19-related mortality and post-infection lung fibrosis in these patients. COVID-19 vaccines and boosters are recommended for patients with T2DM. Further studies involving larger study populations are necessary to validate these findings.
Keywords
Introduction
Coronavirus disease 2019 (COVID-19) is an infectious illness caused by a novel coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). To date, over 100 million people globally have been infected with the virus, with over 6 million deaths. 1 The disease often demonstrates an aggressive clinical course, with unfavorable outcomes observed in the presence of comorbidities, including type 1 and type 2 diabetes mellitus (DM), hypertension (HTN), and cardiovascular diseases.2,3 Given the high prevalence of type 2 DM (T2DM) and evidence showing that patients with diabetes are more vulnerable to severe illness and mortality, T2DM has emerged as an independent risk factor for COVID-19, even after adjusting for age, race and ethnicity, sex, obesity, and HTN.4,5 Underlying mechanisms that contribute to the increased risk of COVID-19 infection in patients with T2DM include a chronic proinflammatory state, extensive tissue damage, and variations in blood glucose levels. 6
The development and distribution of the first COVID-19 vaccines in 2020 are commonly believed to have helped to slow the spread of the disease worldwide and help to reduce the severity of infection and risk of mortality in infected individuals. 7 In Jordan, the first confirmed case of COVID-19 infection was reported on 3 March 2020. Since then, over 1.5 million people have been diagnosed with COVID-19, with more than 14,000 cumulative deaths reported as of the beginning of 2022. However, as of September 2022, only 44.5% of the population in Jordan were fully vaccinated, indicating low uptake of COVID-19 vaccines in comparison with global rates.8,9
Despite the considerable number of published studies on COVID-19 emerging from the Middle East, there is still limited information regarding the effect of COVID-19 infection in patients with diabetes. Whereas COVID-19 infection and diabetes have been extensively studied in higher-income countries (HICs), little is known about the infection among patients with T2DM in low- and middle-income countries (LMICs). The characteristics and outcomes of COVID-19 in LMICs may differ from those in HICs owing to the distinctive factors present in these regions.
Given the high prevalence of T2DM and high rate of COVID-19 infection, alongside low vaccination uptake, there is an urgent need for additional research assessing the prevalence of COVID-19-related morbidity and mortality in this patient population. In the present study, we aimed to evaluate the prevalence of COVID-19 infection among patients with T2DM and associated factors. Our secondary aim was to evaluate COVID-19-related mortality and post-COVID-19 lung fibrosis and mortality in these patients.
Methods
In this cross-sectional study, we reviewed the available database records of patients with T2DM who visited the endocrine clinic at a university hospital between January and September 2019.
Study population
We included all patients aged ≥18 years who were diagnosed with T2DM according to American Diabetes Association (ADA) criteria, 10 visited the endocrine clinic between January and September 2019, and who underwent reverse transcription polymerase chain reaction (RT-PCR) testing for COVID-19 infection. The ADA criteria for the diagnosis of diabetes include glycated hemoglobin (HbA1c) level of 6.5% or higher, fasting plasma glucose level of 126 mg/dL or higher, an oral glucose tolerance test result of 200 mg/dL or higher after a 75-gram glucose challenge or a random plasma glucose level of 200 mg/dL or higher with accompanying hyperglycemia symptoms. We excluded patients with missing laboratory or clinical data, those with end-stage renal disease on dialysis, and those who did not undergo RT-PCR testing.
Informed verbal consent was obtained from all patients or their families by telephone. This study received ethical approval from the University of Jordan Institutional Review Board (IRB # 10/2022/5672, approval date 1/3/2022) and was conducted in line with the ethical principles of the World Medical Association’s Declaration of Helsinki. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 11
Data collection
COVID-19 infection-related data were collected in a review of patients’ electronic medical records as well as in telephone interviews with patients and/or their family members at the end of September 2022 to collect missing data. The following data were collected: basic sociodemographic characteristics, anthropometric measurements (including waist circumference [WC] and body mass index [BMI]), past medical history (including HTN and smoking history), diabetes duration, presence of microvascular complications such as diabetic nephropathy and diabetic neuropathy, macrovascular complications such as cardiovascular diseases and stroke, and current medications. Patients’ most recent laboratory data were also collected, including each patient’s estimated glomerular filtration rate (eGFR) and serum creatinine, serum albumin, HbA1c, and 25-hydroxy (OH) vitamin D levels.
COVID-19-related data included COVID-19 infection status based on a documented positive RT-PCR test result, and COVID-19 vaccination status according to official Ministry of Health vaccination documentation that included the vaccination date and type of vaccine. Vaccination status was determined for the time of COVID-19 infection; positive vaccination status meant that the patient had received any number of vaccine doses prior to COVID-19 infection and negative vaccination status meant the patient had received a vaccine dose after COVID-19 infection or never received a vaccine. The most recent chest computed tomography (CT) scans in patients with confirmed COVID-19 infection were reviewed by a pulmonary physician to assess post-COVID-19 lung fibrotic abnormalities.
For the purposes of this study, COVID-19-related mortality was defined as any death occurring in patients with positive RT-PCR results who died without full recovery from COVID-19 and with no alternative cause of death identified. 9
Statistical analysis
All statistical analyses were performed using Stata statistical software, version 16 (Stata Corp. LLC, College Station, TX, USA). Categorical variables are presented as number and percentage, and continuous variables are presented as mean and standard deviation. Differences between infected and non-infected patients were assessed using the chi-squared test for categorical variables and Student t-test for continuous variables. A multivariable logistic regression model was constructed to identify variables associated with an increased risk of COVID-19-related mortality and binary logistic regression models were constructed to identify variables associated with the development of post-infection lung fibrosis. Potential factors affecting COVID-19 infection and mortality rates were assessed using unit–variable regression analysis. Only significant variables were subsequently included in the final multivariable regression model. The estat vif command in Stata was used to exclude variables with a high variance inflation factor to minimize multicollinearity. The confidence interval (CI) was set at 95% and p values of ≤0.05 were considered to indicate statistical significance.
Results
Of 1652 eligible patients, 1039 (62.9%) met the inclusion criteria (Figure 1). Of these, 429 (41.3%) were men. The mean patient age was 59.5 ± 11.0 years. Among the total patients, the mean duration of T2DM was 10.2 (standard deviation 7.8) years, with mean HbA1c level 7.7% ± 1.5%. In terms of anthropometric characteristics, the mean WC of the cohort was 109.2 ± 14.4 cm, and the mean BMI was 32.9 ± 6.5 kg/m2. Overall, 715 patients (68.8%) had HTN and 450 (43.3%) had albuminuria. In terms of complications, the prevalence of diabetic nephropathy and diabetic retinopathy was 46.2% and 56.6%, respectively. Only 131 patients (12.6%) were current smokers. Most patients were being treated with metformin (n = 821; 79.0%) and angiotensin-converting enzyme inhibitors/angiotensin receptor blockers (n = 561; 54.0%) (Table 1).

Flow chart of patient selection in this study.
Associations between baseline characteristics and COVID-19 infection status among patients with type 2 diabetes mellitus.

ACEIs, angiotensin-converting enzyme inhibitors; ARBs, angiotensin receptor blockers; BMI, body mass index; CAD, coronary artery disease; eGFR, estimated glomerular filtration rate; HbA1c, glycated hemoglobin; HTN, hypertension; SD, standard deviation; T2DM, type 2 diabetes mellitus; WC, waist circumference.
Significant at p ≤ 0.05.
Most patients (n = 905; 87.1%) had received at least one COVID-19 vaccine dose at the time of follow-up. The first-dose vaccine included one of the following: BNT162b2 (Pfizer/BioNTech, 50.9%), BBIBP-CorV (Sinopharm, 32.5%), and ChAdOx1-SARS-COV-2 (Oxford/AstraZeneca, 16.6%). Additionally, 863 patients (83.1%) had received two vaccine doses; the second dose included the BNT162b2 (50.9%), BBIBP-CorV (32.5%), and ChAdOx1-SARS-COV-2 (16.6%) vaccines. Only 183 patients (17.6%) had received a third dose, among which 96.2% had received the BNT162b2 (Pfizer/BioNTech) vaccine and 3.8% had received the BBIBP-CorV (Sinopharm) vaccine; data not shown.
Overall, 336 patients had been infected with COVID-19 at least once as confirmed in PCR testing, resulting in a prevalence of 32.3%. Compared with non-infected patients, those with COVID-19 infection were significantly younger (p < 0.01) and had a significantly higher mean BMI (p = 0.05) and WC (p = 0.03) (Table 1). However, there was no statistically significant difference in vaccination status between infected and non-infected patients. Overall, 22% of patients with COVID-19 infection were admitted to the hospital and 6.8% were admitted to the intensive care unit (ICU); data not shown.
Of the 336 patients with COVID-19 infection, 16 (4.8%) died; however, death was related to COVID-19 infection in only 3% of cases (n = 10). There was no significant difference in all-cause mortality between infected and non-infected patients (4.8% vs. 4.0%). Univariate analysis showed that COVID-19-related mortality was significantly associated with older age, the presence of retinopathy, lower mean serum albumin levels, higher mean BMI and WC, vaccination status (all p < 0.01), and lower eGFR (0.02). Vaccination prior to the time of infection and younger age and were found to be significantly associated with a decrease in the risk of COVID-19-related mortality (odds ratio [OR]: 0.03, 95% CI: 0.0–0.3; p = 0.01 and OR 1.2, 95% CI: 1.04–1.3; p < 0.01, respectively (Table 2).
Risk factors for COVID-19-related mortality among COVID-19-infected patients with type 2 diabetes mellitus (N = 336).
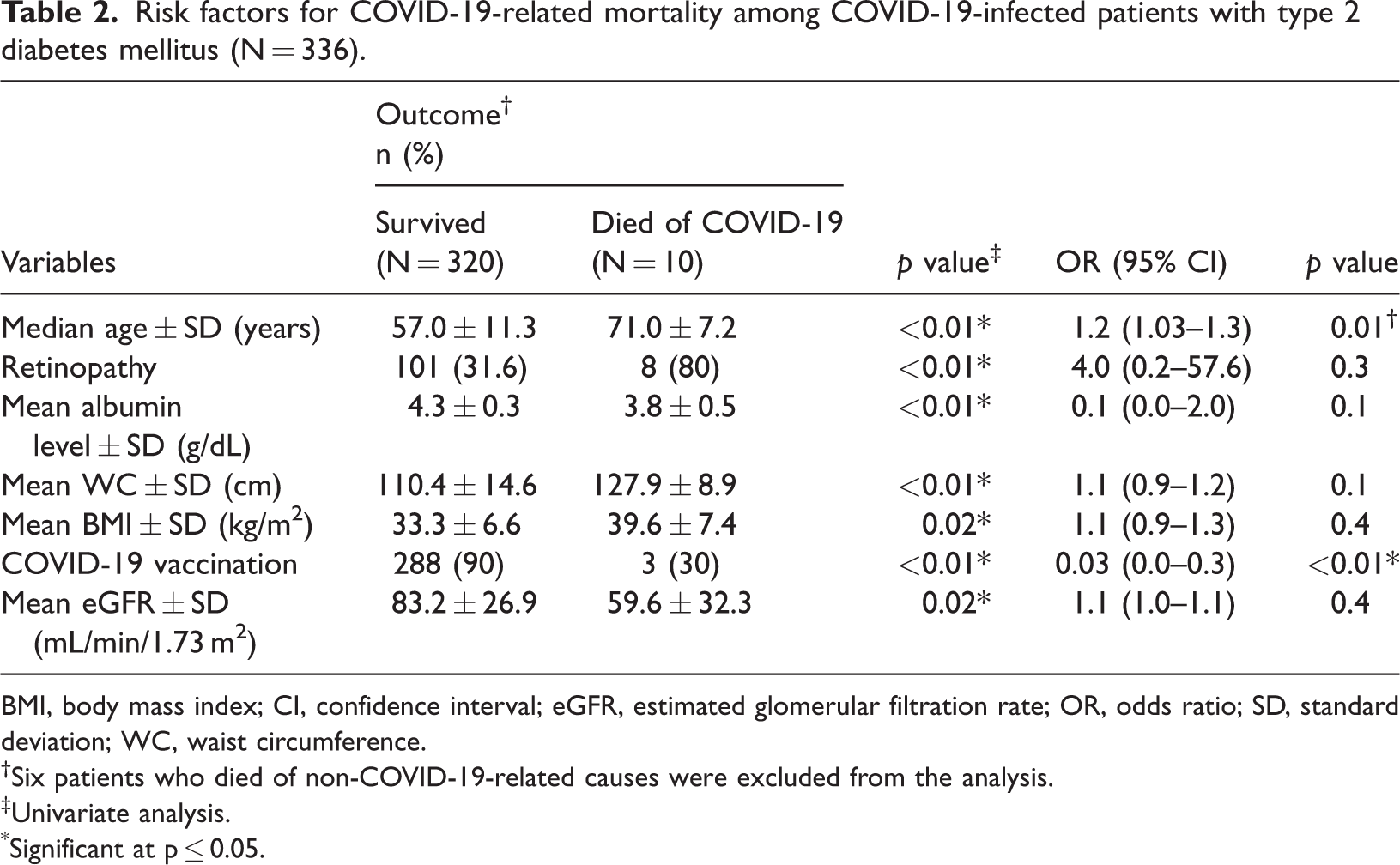
BMI, body mass index; CI, confidence interval; eGFR, estimated glomerular filtration rate; OR, odds ratio; SD, standard deviation; WC, waist circumference.
Six patients who died of non-COVID-19-related causes were excluded from the analysis.
Univariate analysis.
Significant at p ≤ 0.05.
Among 309 surviving patients with past COVID-19-infection who had a chest CT scan during follow up, 19.1% had evidence of post-infection lung fibrotic abnormalities. In univariate analysis, COVID-19-related lung fibrosis was associated with HTN (p = 0.03), coronary artery disease (p = 0.004), increased mean T2DM duration (p < 0.01), lower mean serum albumin levels (p = 0.04), and lower mean eGFR (p = 0.05). In the multivariable model, vaccination status remained the only factor significantly associated with a decrease in COVID-19-related lung fibrosis risk (OR: 0.3, 95% CI: 0.1–0.9; p = 0.03) (Table 3).
Risk factors for post-COVID-19 infection lung fibrosis among surviving COVID-19-infected patients with type 2 diabetes mellitus (N = 309).
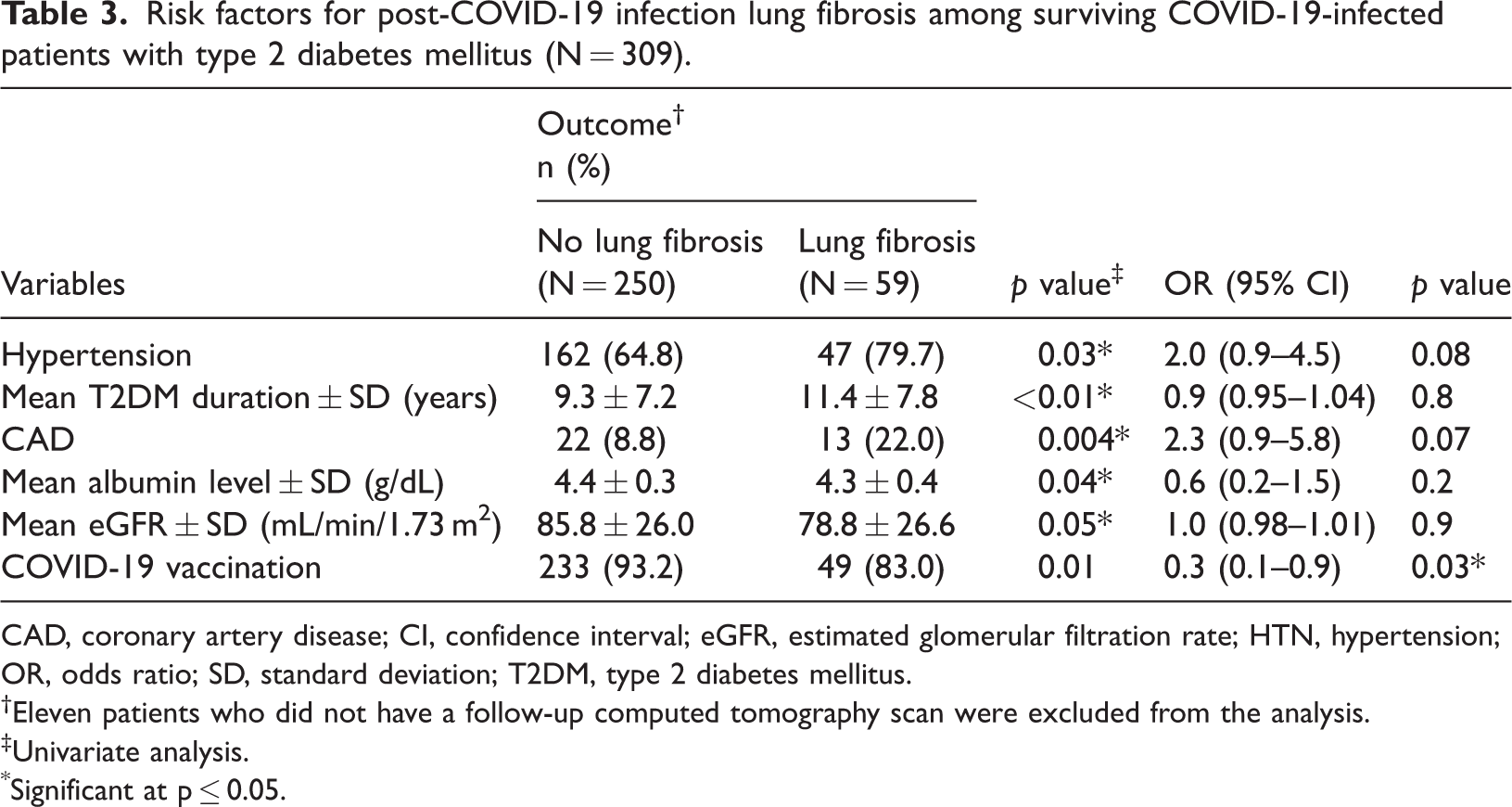
CAD, coronary artery disease; CI, confidence interval; eGFR, estimated glomerular filtration rate; HTN, hypertension; OR, odds ratio; SD, standard deviation; T2DM, type 2 diabetes mellitus.
Eleven patients who did not have a follow-up computed tomography scan were excluded from the analysis.
Univariate analysis.
Significant at p ≤ 0.05.
Discussion
Diabetes is one of the most common comorbidities worldwide and carries a high risk of complications. A recent case series found that between 30% and 40% of patients had diabetes among those who were admitted to the hospital or intensive care or who died as a result of COVID-19 infection. 12 There is a large body of evidence regarding COVID-19 and T2DM in HICs. However, these results cannot necessarily be extrapolated to LMICs. The World Bank has classified Jordan as a LMIC. To the best of the authors’ knowledge, ours is the first study of its kind to be conducted in the Middle Eastern region in which COVID-19 infection among patients with T2DM is investigated. In the current study, we aimed to assess the prevalence of COVID-19 infection among patients with T2DM, as well as the impact of infection on morbidity and mortality in this population. Approximately, one-third of patients with RT-PCR-confirmed COVID-19 had diabetes, a rate much higher than that reported in the general population (17.0%). 13 According to a recent review of 18 publications, Abdi et al. concluded that the cumulative prevalence of diabetes in COVID-19-infected individuals is 14.5%. 14 Similarly, Faghir-Gangi et al. reported that the pooled prevalence of diabetes in individuals with COVID-19 was 14% based on an analysis of 23 articles. 15
In the present study, significantly higher mean BMI and WC values were reported in patients with COVID-19 infection versus in those without infection. Comparable findings have been reported by other researchers; the relationship between these variables suggests a dose-response effect, with increased adiposity being associated with a greater risk of infection. 16 This association is hypothesized to be owing to the increased expression of angiotensin-converting enzyme 2, the receptor utilized by SARS-CoV-2 to infect cells. 17 In several studies, increased age (>60 years) has been associated with a greater risk of COVID-19 infection and greater severity compared with patients under 40 years of age.18–20 In our study, we did not find a difference in the rate of COVID-19 infection according to age. However, it is important to highlight that the mean age of both the infected and non-infected groups in our study was >50 years old, which may explain this variation in findings. Additionally, older patients are less likely to participate in certain social activities or large gatherings and may therefore have a lower risk of exposure to viral infections. 21 However, we found a significant difference in the COVID-19-related mortality rate according to age, which has also been reported in several studies.18–20
In the current study, we found that vaccination status was not significantly associated with a reduction in the prevalence of COVID-19 infection. This may be because vaccines are not as effective in preventing SARS-CoV-2 transmission among immunocompromised individuals compared with non-immunocompromised individuals. For instance, previous research has shown that the immune antibody response is significantly lower in patients with diabetes, indicating an immunocompromised state. 22 Additionally, patients with breakthrough infections following the administration of COVID-19 vaccines have a very high prevalence of several comorbidities, including diabetes. 23
The prevalence of COVID-19-related mortality in the present study was 3%. This finding supports the overall increase in COVID-19-mortality among patients with diabetes compared with the general population. However, other studies have reported higher mortality rates in diabetic cohorts. Kumar et al. reported that diabetes was associated with a two-fold increase in COVID-19-related mortality. 24 In an analysis of 76 studies involving 31,067 patients with COVID-19 infection, Shang et al. concluded that patients with diabetes demonstrated higher case-mortality rates than patients who did not have diabetes (28.5% vs. 13.3%). 25 Other studies have also reported varying COVID-19-related mortality rates, ranging from 9% to 10.6%.26,27 The lower mortality rate seen in our study can be explained by the lower mean age of the cohort, particularly considering that age is a well-established risk factor for COVID-19-related mortality and ICU admission,17–20 as well as a higher vaccination rate at the time of infection. Additionally, the low mortality rate and low rates of hospital (22%) and ICU admission (6.8%) noted in our study may be owing to the high vaccination rate, with 83.1% of patients having received at least two vaccine doses. Studies have shown that COVID-19 vaccines are very effective in decreasing mortality and morbidity, thereby reducing rates of hospital and ICU admission for COVID-19. 28
In this study, a multivariable model revealed that the risk COVID-19-related mortality was not associated with any patient sociodemographic or clinical characteristics or laboratory variables, apart from age and vaccination status. Other studies have reported associations with several variables; for instance, age, the presence of cardiovascular diseases, and BMI have been associated with higher mortality among patients with diabetes. 19 The CORONADO study (Coronavirus SARS-CoV-2 and Diabetes Outcomes) also found that HbA1c levels and microvascular complications were associated with increased mortality among COVID-19-infected patients with diabetes. 26 However, it is important to mention that our analysis showed that vaccinations were significantly protective against COVID-19-related mortality. Several population cohort studies have similarly found that vaccines were effective in populations with a high prevalence of diabetes.27,29
In terms of the development of post-COVID-19 lung fibrosis, we found that 19.1% of COVID-19-infected patients with diabetes developed lung fibrosis. Harding et al. reported that diabetes increased the risk of post-acute COVID-19 syndrome (PACS) by four times. 30 Raveendran et al. suggested that successful glycemic control together with physical activity and rehabilitation were helpful in the management of patients with PACS, indicating that these factors may play a role in the development of PACS. 31 Moreover, in our cohort, vaccinations were significantly protective against the development of lung fibrosis. Other studies have demonstrated that vaccinated patients with breakthrough infections were at lower risk of developing PACS. 32
Strengths and limitations
To the best of the authors’ knowledge, the present study is the first to demonstrate that vaccination may reduce the risk of post-COVID-19 lung fibrosis in patients with T2DM. This might be the result of reduced COVID-19 severity among vaccinated patients because disease severity is a risk factor for PACS. 33 The current study is also the first to describe the impact of COVID-19 infection in patients with T2DM in Jordan over 2 years during the pandemic. Moreover, ours is the only study to report clinically significant evidence linking vaccine status and the development of lung fibrosis as a post-COVID-19 complication. This study also has several limitations. First, the single-center setting of the study and small number of patients limit the generalizability of our findings. Second, the retrospective study design permits inference of the associations between the variables of interest but causation cannot be proven. Furthermore, although we used regression models to adjust for confounding variables, the risk of confounding bias cannot be completely eliminated alongside other unmeasured confounders. Finally, we were unable to determine associations between the type of vaccine or number of vaccine doses and the risk of COVID-19-related mortality and post-infection lung fibrosis.
Conclusion
Patients with T2DM showed a higher prevalence of COVID-19 infection and COVID-19-related mortality in comparison with the general population. COVID-19 vaccines may be associated with lower COVID-19-related mortality and post-infection lung fibrosis in patients with diabetes. COVID-19 vaccines and boosters should be recommended to patients with T2DM. Further studies with a larger study population are needed to confirm our findings.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231198413 - Supplemental material for Prevalence and risk factors of COVID-19 infection, mortality, and post-infection lung fibrosis in patients with type 2 diabetes: a cross-sectional study
Supplemental material, sj-pdf-1-imr-10.1177_03000605231198413 for Prevalence and risk factors of COVID-19 infection, mortality, and post-infection lung fibrosis in patients with type 2 diabetes: a cross-sectional study by Randa Farah, Hussam Al-Hawari, Asma Albtoush, Amani Nofal, Tala Basheer Hyasat, Raghed Abdel Hay Abu Jabeh, Lojayn Tareq Suboh, Ahmad A. Toubasi, Tareq Fatah Eqrai and Mohammad Abufaraj in Journal of International Medical Research
Footnotes
Acknowledgements
The authors cordially thank the participants in this study for their time and valuable contribution to this research. We also extend our gratitude to the Deanship of Academic Research at the University of Jordan for their assistance in this study.
Authors’ contributions
Randa I. Farah contributed to study conceptualization; formal analysis; methodology; supervision; and original writing, drafting, review, and editing of the manuscript. Hussam Al-Hawari contributed to study supervision and editing, and reviewing the final manuscript. Asma Albtoush' contributed to the study methodology and supervision, and reviewing the final manuscript. Amani Nofal, Tala Hyasat, Raghad Abu Jebbeh, and Lojayn Salah contributed to data curation and coding, study methodology, programming and software development, and writing the original draft of the manuscript. Ahmad Altobasi contributed to the collecting missing data and writing of the original draft of the manuscript. Mohammad Abufaraj contributed to formal analysis, study supervision, and editing of the final manuscript. All authors gave their final approval and agreed to be accountable for all aspects of the work, ensuring its integrity and accuracy.
Data availability
All data generated or analyzed during this study have been included in the manuscript. The raw datasets used and/or analyzed in the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.