
Abstract
Objective
To investigate the association between seasonality and intentional drug overdose (IDO), a commonly seen method of self-harm in daily emergency medicine practice.
Methods
Cases of IDO were retrospectively selected using the International Classification of Diseases (ICD)-10 coding system (codes T36–T50), in patients who attended the Emergency Department of MacKay Memorial Hospital between January 2018 and August 2019. Data regarding age, sex, arrival time, marital status, vital signs, comorbidities, psychiatric history, social conflicts, substance of overdose, and length of hospital stay by season, were analysed using Student’s t-test and χ2-test.
Results
Of all included cases (n = 196), IDO occurred most frequently in spring (32.1%), particularly in male patients (28/49 male cases). First-time IDO occurred most frequently in spring (51/133 first-time cases) and most spring cases were first-time IDO (51/63 spring cases). Repeat IDO occurred most frequently in autumn (20/63 repeat cases). Female conflict with father and/or boyfriend, and personality disorder in patients who overdosed, showed seasonality with a spring peak. Hospital admission rate was highest in winter (10/45 winter cases [22.2%]).
Conclusion
Episodes of IDO exhibited seasonality, with a spring peak, particularly for male patients, female patients in conflict with father and/or boyfriend, and those with personality disorder. Clinicians should pay close attention to the abovementioned patient groups.
Introduction
Suicide behaviour is a complex issue involving environmental, biological, psychological and social factors, and is one of the most common issues encountered in daily emergency practice. 1 Drug overdose is a type of non-violent suicide method that does not involve the direct infliction of bodily harm. Intentional drug overdose (IDO) is by far the most common method of self-harm involved in suicide behaviour, accounting for between 65 and 85% of all hospital-based self-harm presentations. 2 Seasonality of suicidal behaviour has been widely studied previously, with a well-replicated suicide peak in spring,3–5 however, one study in Finland found an autumn peak in poisoning among females. 6 In previous studies, no uniform pattern for seasonality in IDO has been found. One study in Italy showed suicides committed by poisoning methods peaked in the spring and late autumn. 7 A Swiss study revealed that seasonality of suicide differed largely by suicide method, and there was no significant seasonality in drug overdose. 8 A study in Singapore found that suicides tended to peak in the spring months, particularly in April and May, but no detailed data on overdosage or poisoning were available. 9 In a study conducted in Taiwan, seasonality was concluded to exist in violent suicides, and trends showed an obvious peak during March for nonviolent suicides. 10 The aim of the present study was to clarify the association between seasonality and IDO. Seasonality of IDO and associated risk factors were investigated via a retrospective review of records between January 2018 and August 2019 at a tertiary teaching medical centre in northern Taiwan.
Patients and methods
Study population
Mackay Memorial Hospital, Taipei, is a tertiary care medical centre with 196 570 Emergency Department visits reported annually. In this retrospective observational cohort study, data were collected by searching the hospital database for all patients who had attended the Emergency Department of Mackay Memorial Hospital, with International Statistical Classification of Diseases and Related Health Problem 10th Revision (ICD-10) coding specific for drug overdose, including T36–T50 (Table 1), between January 2018 and August 2019. Patients with a diagnosis of overdose (defined as exceeding a normal drug treatment dose) and poisoning were selected according to the inclusion criteria. Following chart review, patients who were diagnosed with unintentional overdose, including mis-swallowing and accidental adverse drug reaction, were excluded from the study.
International Classification of Diseases (ICD)-10 coding system for poisoning (codes T36–T50) used for participant selection in the present study.

The study was approved by the Institutional Review Board of MacKay Memorial Hospital: 22MMHIS168e, and the requirement for informed patient consent was waived due to the retrospective study design. All patient details were de-identified and the reporting of this study conforms to STROBE guidelines. 11
Study variables
Data regarding age, sex, time of presentation to the emergency department, season of presentation to the emergency department, repeated act history, marital status, concurrent ethanol use, vital signs on arrival, Glasgow coma scale score, related comorbidities, psychiatric history, interpersonal conflicts, categories of overdose, presence of insomnia, length of hospital stay, and hospitalization status, were extracted. Data were analysed according to seasons, where spring was defined as March, April, and May; summer as June, July, and August; autumn as September, October, and November; and winter as December, January and February.
Statistical analyses
Data are presented as n (%) prevalence or mean ± SD, and were analysed using IBM SPSS Statistics software for Windows, version 25.0 (IBM Corp., Armonk, NY, USA). Student’s t-test or χ2-test were used in statistical analyses, and a P value < 0.05 was considered to indicate a statistically significant difference.
Results
Hospital records from a total of 299 patients were retrieved from the hospital database. Following chart review, 103 patients were excluded due to unintentional overdose, including mis-swallowing and accidental adverse drug reaction. Thus, a total of 196 patients who presented at Mackay Memorial Hospital Emergency Department with IDO between January 2018 and August 2019 were enrolled into the study. The age of the study population ranged from 14 to 92 years (mean ± SD, 39.2 ± 18.3 years) and the male to female ratio was 1:3 (male, n = 49; female, n = 147).
Intentional drug overdose was found to occur most frequently in spring (63/196 patients [32.1%]). Analysis of male and female subgroups revealed a spring peak in IDO for male patients (28/49 male patients [57.1%]; P < 0.001 between seasons), but no statistically significant differences in IDO rates between seasons for female patients (Figure 1 and Table 2), similar to a previously reported study. 12 A total of 63/196 patients (32.1%) had a previous history of IDO. First IDO occurred most frequently in spring (51/133 patients with first IDO [38.3%]). Repeat acts of IDO occurred most frequently in autumn (20 out of 63 repeat IDO cases [31.7%], P = 0.024; Figure 2 and Table 2), however, only 44.4% of autumn cases were repeat acts of IDO, with most autumn cases involved first-time IDO (25/45 cases [55.6%]). The involvement of alcohol in IDO presentations was significantly higher in spring (24 out of 54 cases involving alcohol [P = 0.046], and 24/63 overall spring cases [38.1%]). Among patients with psychiatric disorders committing IDO, those with personality disorder showed seasonality, with a statistically significant peak in spring (32 of 75 IDO cases with personality disorder [42.7%] and 32 of 63 spring IDO cases [50.8%]; P = 0.002). In terms of interpersonal conflict, conflict with father showed seasonality with a peak in spring (eight out of 10 cases in conflict with father [80%] and 8 out of 63 spring cases [12.7%]; P = 0.01), as did conflict with boyfriend (four out of four cases in conflict with boyfriend [100%] and 4 out of 63 spring cases [6.3%]; P < 0.05) (Table 2). Admission rate was highest in winter (10 out of 22 ward admissions [45.5%] between January 2018 and August 2019, and 10/45 winter cases [22%]; P = 0.009).
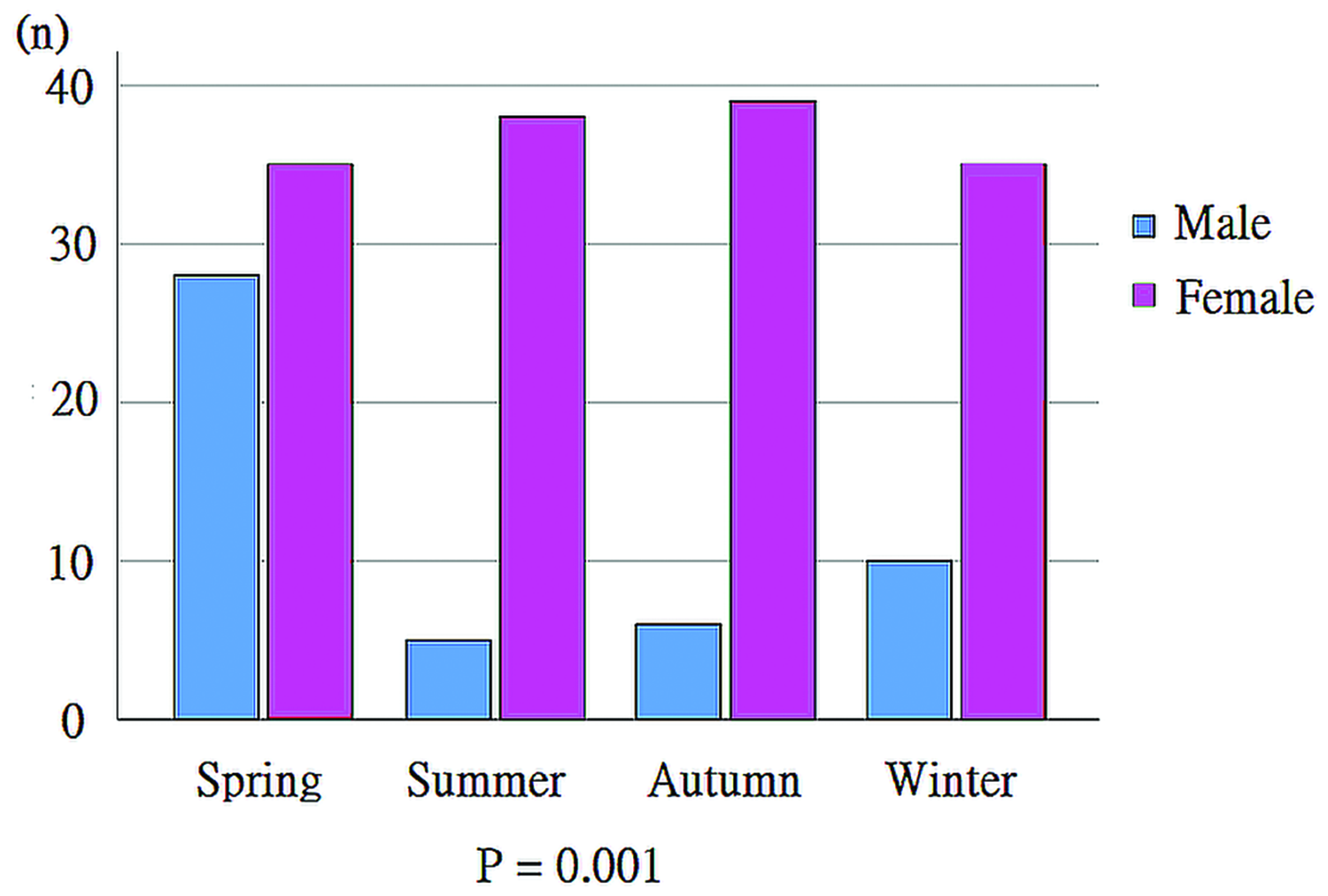
Gender differences by season in 196 intentional drug overdose cases.
Comparison of 196 intentional overdose cases according to season.

Data presented as n (%) prevalence or mean ± SD.
Bp, blood pressure; bpm, beats per min; ICU, intensive care unit.
NS, no statistically significant between-group difference (P ≥ 0.05, Student’s t-test or χ2-test).
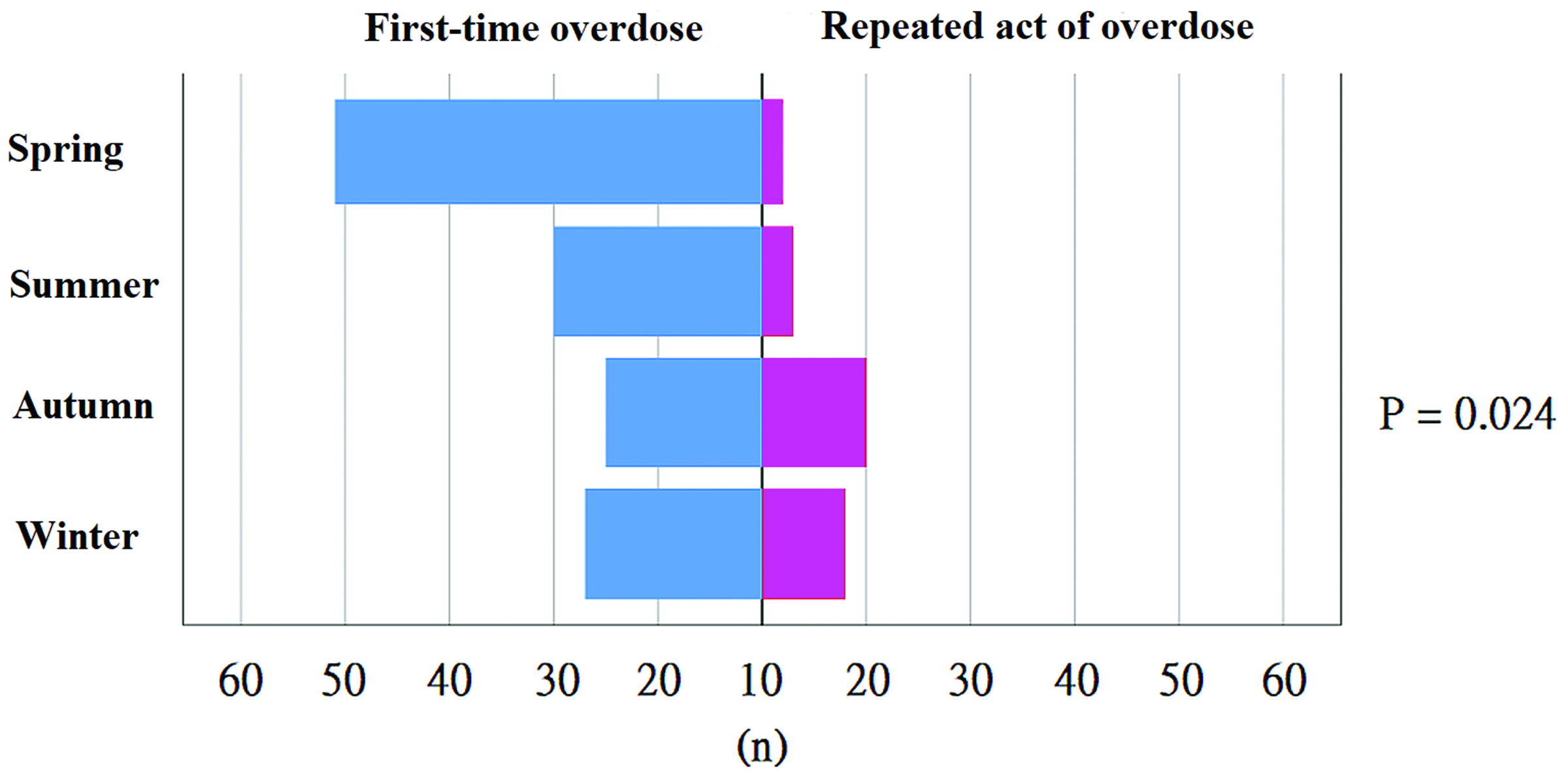
First-time (blue bars) and repeat acts (pink bars) of intentional drug overdose by season in 196 cases, showing an autumn peak in repeat intentional drug overdose.
No statistically significant differences between seasons were found in emergency department arrival time, marital status, comorbidities, vital signs, Glasgow coma scale score, bipolar affective disorder, depression, schizophrenia, presence of insomnia, or length of hospital stay. Winter was associated with a numerically longer mean time in hospital (3 ± 5.1 days), however, this difference was not statistically significant versus other seasons (P = 0.064). Among substances associated with IDO, benzodiazepine was used most frequently (62 cases [31.6%]). No statistically significant seasonal differences were found in substances used in cases of IDO (Table 3).
Substances associated with 196 cases of intentional drug overdose.

Data presented as n (%) prevalence.
Mixed medications indicates pills that were missing their wrappers or had been opened, and could not be discriminated based on medical records.
No statistically significant difference in substances between seasons (P = 0.250; χ2-test).
Discussion
Seasonality of IDO with sex differences
The present study showed seasonality of IDO in male patients only, with a peak in spring (57.1%), which was consistent with previously published studies from Iran and Italy that illustrated a peak in the spring season for medication intake as an attempted suicide method.13,14 A study conducted in Finland found significant differences between the sexes in choice of suicide methods, with males tending to choose a more violent method compared with females. 6 In their study, drug overdose accounted for about 60% of non-violent suicides among males and over 90% of female non-violent suicides. 6 Suicide behaviour is complex, involving multiple factors, and the definite cause of this gender difference remains unclear. A possible mechanism to explain the seasonality of suicide behaviour is lower plasma tryptophan levels measured in spring. 15 Tryptophan is the main precursor of serotonin, and serotonin deficits are implicated in the pathogenesis of depression, aggression, impulsivity, suicidal ideations, and suicide attempts. 16
There is evidence for differences between the sexes in variants of genes related to serotonergic transmission and gene–environment interactions, which may contribute to the risk of depression. 17 Also, suicidal behaviours seem to be associated with hyperactivity of the hypothalamic–pituitary–adrenal (HPA) axis. 18 In a study by Uhart et al., 19 healthy male subjects were demonstrated to have greater HPA axis responses to a psychological stressor than healthy female subjects. Cortisol levels exhibit seasonal rhythmicity, with peak levels occurring during winter and reduced levels occurring in summer. 20 Seasonal changes in cortisol secretion and the different HPA axis response between the sexes may also partially contribute to sex differences in suicide behaviour. Another hypothesis for the sex difference in seasonality of suicide behaviours is the involvement of socioeconomic factors. For example, males tend to perform more outdoor work compared with females, and increased exposure to the outdoor environment may result in physiobiological factors, including day length, light, temperature, pollution, pathogens or allergens, contributing to a more seasonal effect. 21
Seasonality of repeat IDO peaked in autumn
Drug overdose has been identified as the most commonly used method in repeated suicidal attempts. 22 Compared with other methods of self-harm, drug overdose is shown to be far less likely than other methods to lead on to switching methods. 23 The present study revealed that repeat acts of IDO showed significant seasonality with an autumn peak (31.7% of repeat IDO cases), representing 44.4% of autumn IDO cases. A repeat act of suicide is influenced by multiple factors. For example, a study in Spain showed that alcohol use, personality disorders and younger age are risk factors for re-attempting suicide. 24 In a cohort study conducted in Spain by Finkelstein et al., 25 17.0% of patients were reported to commit a repeat overdose, which was lower than that found in the present study (32.1%), and associated risk factors included psychiatric care in the preceding year, alcohol dependence, and documented depression. Female sex, rural residence, lower socioeconomic status, ingestion of psychoactive drugs, and younger age have also been weakly associated with repeat overdose. 22 The mechanism behind the seasonality of repeat IDO remains poorly understood, and it may be influenced by many confounding factors.
Seasonality of IDO with concurrent alcohol use peaked in spring
A UK study showed an increase in the concurrent use of alcohol with suicide, despite a decline in drinking among the general population, and drug overdose with concurrent alcohol use may increase the lethality. 26 In the present study, the involvement of alcohol in IDO presentations was found to be significantly higher in spring (44.4% of all IDO cases involving alcohol, and 38% of all spring cases), which was similar to a study conducted in Poland that showed a significant relationship between alcohol misuse and suicide during spring, and concluded that the older the victims, the higher the alcohol concentration. 27 A study conducted in Sweden also showed a spring peak in alcohol-related suicide, 28 and as with seasonality of suicide behaviour, the seasonality of alcoholism is also hypothesised to be through the brain serotonergic system. 29
Seasonality of IDO with personality disorder peaked in spring
The impact of psychiatric disorders on the likelihood of suicidal behaviour has long been a subject of interest and discussion. Kim et al. 30 reported that depressed suicides without comorbid cluster B personality disorders committed suicide in the spring/summer, and suicides involving schizophrenia occurred in the autumn/winter. Their study showed significant seasonal variation in suicide between patients with different psychopathologies, however, the study population was limited to male suicide completers, regardless of suicide method. 30 Doganay et al. 31 reported no significant seasonality of suicide attempt in patients with personality disorder, but in those with depression, results showed significant seasonality of suicide attempt, with a peak in spring and summer. A study conducted in Sweden showed that a history of inpatient-treated psychiatric disorder was associated with an increase in suicide seasonality. 32 However, the study population was limited to patients with psychiatric disorders severe enough to require hospital admission, and the results showed significant seasonality mainly in violent methods of suicide involving infliction of bodily harm. 32 The present results showed significant seasonality for IDO in patients with personality disorder, with a peak in spring (42.7% of IDO cases with personality disorder), and 50.8% of spring IDO cases had personality disorder. Personality disorders, and their co-morbidity with other psychiatric, are shown to be risk factors for suicidal behaviors. 33 However, the mechanism behind different seasonal patterns of suicide attempts between specific psychiatric disorders remains unclear. One possible mechanism of seasonality in suicide attempt is through the brain serotonergic system, and several psychiatric disorders involve central serotonergic dysfunction. 34 Given that different diseases might result from one or more different processes, such as defective synthesis, release, re-uptake, catabolism, or metabolism of serotonin, 35 the impact of seasonal change may differ between different diseases. The present results should be interpreted with caution due to the possibility of underestimation, as some patients may have had a psychiatric disorder that was undiagnosed at the point of emergency department visit.
Seasonality of IDO without significant correlation to comorbidities
Many chronic diseases are known to be associated with elevated risk of suicide, including haemodialysis for renal failure, epilepsy, asthma, HIV infection, and cancers. 35 However, the present study showed no specific seasonal pattern in IDO with comorbidities (hypertension, diabetes mellitus, or uraemia). One physical illness described in the literature to present with suicide seasonality is atopic disease, which may intensify the seasonal variation of suicide. 36 However, atopic disease was not included as a comorbidity in the present study, and it remains unclear whether a seasonal pattern would be replicated in cases of drug overdose.
Seasonality of IDO with interpersonal conflict
Psychosocial factors are known to be associated with increased risk of suicidal self-poisoning attempts, particularly interpersonal conflict. 37 In the present study, conflict with father or boyfriend showed seasonality with peaks in spring (P = 0.010 and P = 0.035). This phenomenon is also consistent with differences between the sexes in response to serotonergic system regulation in seasonal change, which involves aggression and impulsivity, and thus leads to conflict.
Seasonality of hospitalization in IDO peaked in winter
The present study showed significant seasonality in admission rate, with a winter peak (10 out of 22 ward admissions [45.5%], and 10 out of 45 winter IDO cases [22.2%], P = 0.009). The higher admission rate in winter may indicate a higher severity of overdose or higher risk of re-attempting suicide, and this seasonal effect may be influenced by several factors, including the climate. Climatic factors in winter may involve cooler temperature, higher humidity, and more raining days, and a study conducted in Finland demonstrated that winter with low solar radiation may be associated with increased risk of suicide. 38 In terms of temperature, current evidence indicates that higher temperatures increase suicide rates, 39 however, humidity and rainfall appear to have no significant effect on suicide frequencies.10,38,40 Of note, the most common substance used in IDO in the present study population was found to be benzodiazepine, which would not usually lead to admission. Therefore, it may be hypothesized that people would be admitted due to the use of more dangerous substances, such as cardiovascular medication or antidepressants. Further subgroup analysis may be warranted to clarify such relationships.
The present study described IDO in terms of seasons and gender, and, to the best of the authors’ knowledge, is the first to describe analyses of interpersonal conflict as a predisposing factor for suicide. The results may be limited by several factors, such as the single-centre study setting, and data collection via medical records, which may easily have resulted in loss of information due to the retrospective study method. Future IDO studies should involve a prospective study design, or a study population enrolled from a national registry database.
Conclusion
Although IDO is commonly observed in female patients, the present study identified a seasonal pattern in episodes of IDO with a peak in spring (32.1%) that was driven by IDO seasonality in male patients (57.1%), personality disorder (50.8% of spring cases), and conflict with father or boyfriend. Repeat acts of IDO peaked in the autumn (44.4% of autumn IDO cases), and hospitalization due to IDO peaked in winter (22.2%). No statistically significant seasonal differences were found in arrival time, marital status, comorbidities, vital signs, Glasgow coma scale, or substance overdosed. Clinicians should pay close attention to the patient factors described in the present study to help prevent IDO episodes in different seasons.
Footnotes
Acknowledgements
We thank the Emergency Department of MacKay Memorial Hospital, Taiwan.
Author contributions
Chih-Hung Lo, Chen-Hao Liao, and Sheng-Teck Tan: data collection and writing.
Yu-Jang Su: study design, statistical analysis, data collection, writing, manuscript revision and correspondence.
Data availability statement
De-identified data are available upon request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.