
Abstract
Background
Migration of tissue clips into the common bile duct and formation of common bile duct stones after laparoscopic biliary surgery are extremely rare complications, and their etiologies remain elusive. We herein report four cases of migrated clips complicated by stones after laparoscopic biliary surgery.
Case presentation
Two patients (72- and 62-year-old women) were admitted because of varying degrees of epigastric pain, and two patients (88- and 69-year-old men) were admitted because of epigastric pain with chills and fever. They had previously undergone laparoscopic cholecystectomy (LC) plus laparoscopic common bile duct exploration (LCBDE) in our hospital. In Cases 1, 2, and 4, surgery revealed gallbladder triangle adhesion, inflamed dilated bile ducts, and fragile tissues. Blood tests showed elevated liver enzymes and bilirubin. Imaging indicated common bile duct stones. All patients underwent successful surgery with Hem-o-lok clips. No postoperative pain recurred.
Conclusion
Clip migration after laparoscopic biliary surgery may be associated with preoperative biliary duct inflammation, improper use of tissue clips, and postoperative biliary leak-induced inflammation. The clinical presentation is similar to that of calculous cholangitis. Once symptoms of cholangitis appear in patients with a history of LC or LCBDE, the possibility of clip migration and stone formation should be considered.
Keywords
Introduction
Laparoscopic common bile duct exploration (LCBDE) is the gold standard for the treatment of gallbladder stones and common bile duct stones. 1 Among other factors, tissue clips that migrate into the common bile duct may cause biliary obstruction, leading to stone formation and cholangitis. This report describes four cases of clip migration and stone formation after laparoscopic biliary surgery. The purpose of reporting these cases is to explore the causes, diagnostic methods, and management approaches for postoperative clip migration in LCBDE in an effort to prevent the formation of secondary stones due to bile duct clip migration.
Case presentation
Case 1: A 72-year-old woman was admitted to our hospital because of a 3-day history of epigastric pain. Post-admission magnetic resonance cholangiopancreatography (MRCP) examination suggested common bile duct stones and gallbladder stones with chronic cholecystitis (Figure 1), and she underwent laparoscopic cholecystectomy (LC) + LCBDE in December 2019. Intraoperative examination revealed dilated bile ducts with severe inflammatory edema, and Hem-o-lok clips were used to close the appendicular stumps. The patient recovered well after surgery and was discharged from our hospital. In December 2021, she was readmitted to our hospital because of a 3-day history of right upper abdominal pain, and magnetic resonance imaging + MRCP of the upper abdomen suggested bile duct filling defects (Figure 2). Adhesions were removed intraoperatively and the common bile duct was incised for choledochoscopy, which showed two yellow stones of 10-mm diameter and three tissue clips as the core of the stones (Figure 3). The patient was successfully discharged from our hospital after surgery.

Inflammatory edema of the gallbladder triangle, dilation of the cystic duct, and compression of the common hepatic duct with stenosis.

A foreign body in the form of a stripe (external shape resembles a Hem-o-lok clip) is visible in the common bile duct.

Stones with tissue clips as the core.
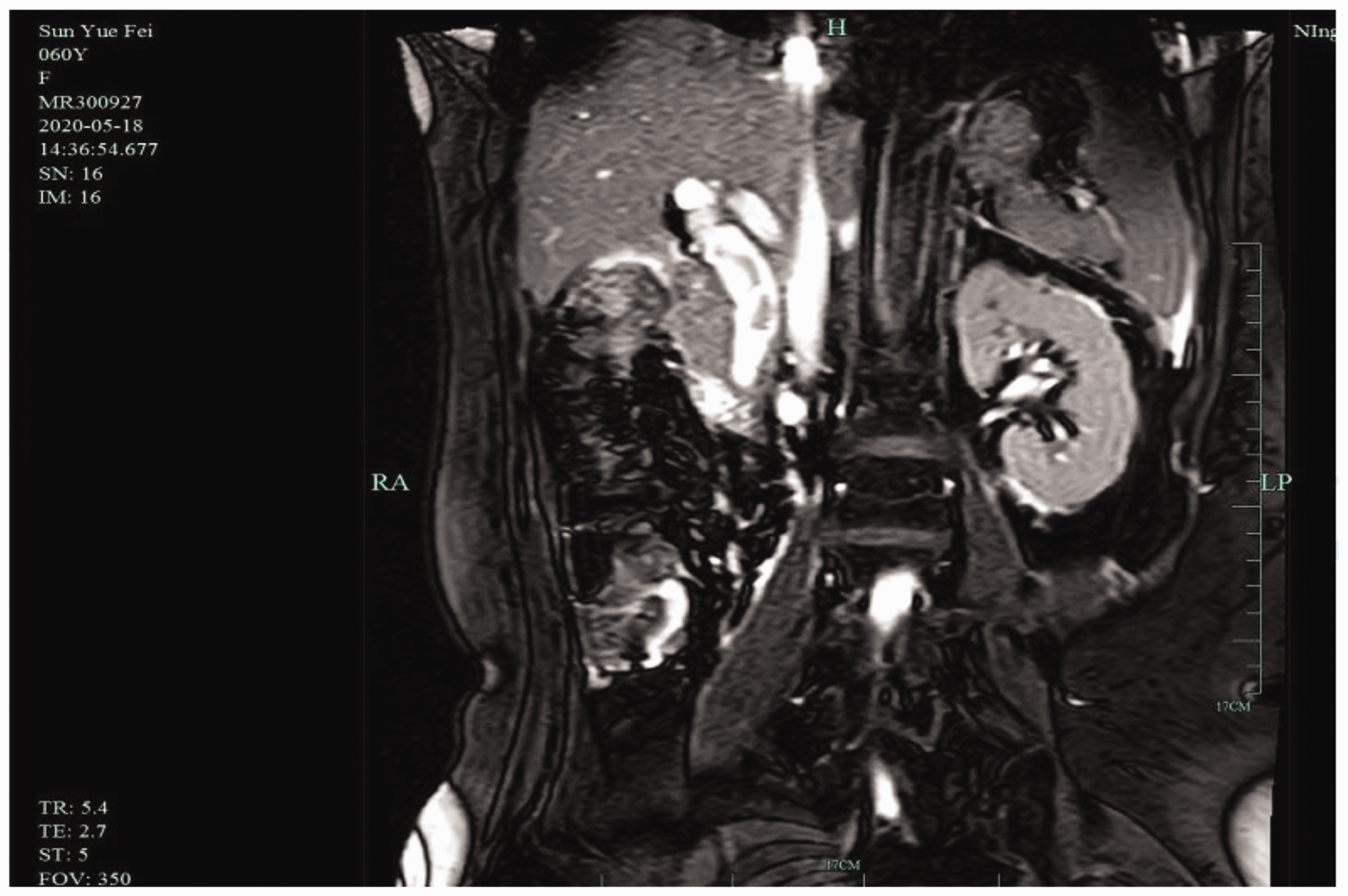
Case 2: A 62-year-old woman was admitted to our hospital because of a 2-day history of epigastric pain. MRCP suggested common bile duct stones and cholecystitis with gallbladder stones (Figure 4). In October 2018, she underwent surgery in our hospital. Gallbladder edema was obvious, and gallbladder stones were considered to be draining into the common bile duct through the cystic duct. LC + LCBDE was performed, and two tissue clips remained in the stump of the cystic duct. The patient was discharged after successful recovery. She was subsequently admitted to our hospital in May 2020 because of a 13-hour history of severe epigastric pain accompanied by nausea and vomiting and yellow sclera. MRCP suggested dilated intrahepatic and extrahepatic bile ducts, and the common bile duct had a diameter of about 1.9 cm with multiple winding cord-like stones inside (Figure 5). The patient was treated surgically. The adhesion in the gallbladder triangle was removed, the common bile duct was incised, and choledochoscopy was carried out (Figure 6). Two tissue clips and several stones were removed. She was discharged from our hospital after successful postoperative recovery.

Stone impaction at the cystic duct, with marked dilatation of the cystic duct and multiple stones in the common bile duct.
Striated stones are visible in the common bile duct (external shape resembles a Hem-o-lok clip).

Migration of tissue clips into the common bile duct.
Case 3: An 88-year-old man was admitted to our hospital because of a 3-day history of recurrent epigastric pain with chills and fever. MRCP suggested cholecystitis with gallbladder stones and multiple stones in the common bile duct (Figure 7). He underwent surgery in September 2020. Intraoperatively, there was no significant dilatation or edema in the bile duct; the multiple stones in the common bile duct were considered the primary stones, and the patient was discharged after surgery with no postoperative complications. In April 2022, he was admitted to our hospital because of a 2-day history of epigastric pain, and computed tomography of the upper abdomen revealed a high-density shadow in the common bile duct (Figure 8). Two Hem-o-lok clips and several stones were removed by choledochotomy. The patient was discharged from our hospital after successful postoperative recovery.

Cholecystitis with gallbladder stones and common bile duct stones.

Dense tissue entrapment is observable in the common bile duct.
Case 4: A 69-year-old man was admitted to our hospital because of a 3-day history of epigastric pain. MRCP suggested cholecystitis with gallbladder stones and multiple stones in the common bile duct (Figure 9), and surgery was performed in March 2021. Intraoperatively, there was no significant dilatation or edema of the bile cyst duct; the multiple stones in the common bile duct were considered the primary stones, and the patient was discharged after an uneventful postoperative recovery. He was admitted to our hospital in August 2022 because of a 3-day history of epigastric distension with fever and yellow urine. MRCP showed multiple stones in the common bile duct with bile duct dilatation (Figure 10). He was treated by laparoscopic surgery, and two Hem-o-lok clips and several stones were removed intraoperatively by common bile duct incision.

Cholecystitis with gallbladder stones and multiple stones in the common bile duct.

Multiple nodular filling defects are observed in the common bile duct.
Discussion
Despite the large number of LCBDE procedures performed worldwide, postoperative migration of tissue clips into the common bile duct with secondary choledocholithiasis is extremely rare. Few relevant reports have described this complication, and only a single case has been reported. 2 The present report describes four cases of migrated clips with stone formation after laparoscopic biliary surgery from October 2018 to September 2022 among 168 LCBDE procedures during this period (incidence of 2.38%).
Three of the four patients were considered to have gallbladder stones secondary to discharge of stones into the common bile duct. All of these patients were found to have adhesion in the gallbladder triangle, dilated bile ducts with inflammatory edema, and brittle tissues intraoperatively. One patient was elderly and had a poor nutritional status. All four patients underwent preoperative magnetic resonance imaging or computed tomography, which showed a morphology similar to that of a tissue-clamped foreign body in the common bile duct. Subsequent intraoperative examination confirmed that the tissue was clamped within the common bile duct, and the clamping of the tissue was the core of the stone formation. The duration of postoperative clamp migration ranged from 1.4 to 2.0 years, with an average of 1.64 years.
The mechanism of clip migration after laparoscopic biliary surgery has not been fully clarified. Three important aspects of the cases in this report are as follows. First, brittle tissues developed secondary to inflammation, edema, malnutrition, and other factors, and the tissue clip on the stump of the cut cystic duct migrated to the common bile duct. 3 Second, the tissue was clamped within the common bile duct to avoid residual gallbladder duct stones. After relaxing the gallbladder traction, the head end of the tissue clip placed pressure on the lateral wall of the common bile duct, resulting in a biliary fistula and clip migration. Third, in addition to the above-mentioned factors, some scholars have also reported that postoperative biliary leakage may cause adhesion in the gallbladder triangle, inflammation in the surrounding tissues, and increased brittleness, leading to detachment and migration of clips from the cystic duct or arterial stump. 4 No postoperative biliary leakage occurred in any of the four patients in the present study. With respect to the mechanism underlying migration of tissue clips into the common bile duct after performing LCBDE, the local inflammatory reaction caused the tissue clips to become wrapped during formation of the T-tube sinus tract, and when the T-tube was removed, the tissue clips fell into the common bile duct along the sinus tract. 5 All four patients in the present study underwent choledochoscopy after T-tube removal, and no tissue clip was found in the sinus tract or common bile duct. Regarding the management of tissue clips, most scholars believe that endoscopic retrograde cholangiopancreatography (ERCP) is the preferred treatment because it is considered to have the advantages of less trauma and faster recovery. However, we used LCBDE in our four patients, mainly with consideration of the following two key points. First, the patients were treated with nutritional support such as fasting and anti-inflammatory therapy after admission, and the symptoms of abdominal pain and fever were relieved. Second, in some patients, the time from biliary surgery to tissue clip displacement was short, the sinus tract between the tissue clip and the common bile duct was not fully formed, and the tissue clip had not entered the common bile duct.
ERCP and LCBDE should be considered as companions rather than competitors when choosing the treatment modality for tissue clip migration. LCBDE provides a large operative space and good visual field, and the success rate of surgical clip removal is higher for patients with more severe tissue clip adhesion. However, for patients with unstable vital signs or acute infection, LCBDE takes a long time to perform, is difficult, and has high surgical risk. ERCP facilitates rapid recovery, induces less trauma, and allows for more effective emergency decompression treatment. Moreover, it may facilitate the removal of stones missed in laparoscopy, and its diagnostic and therapeutic value for biliary tract diseases should not be underestimated. However, there is a possibility of treatment failure in patients with dense tissue clips and surrounding tissue adhesions, and it is technically demanding for physicians.
Conclusions
Although postoperative clip migration after LCBDE rarely occurs, it is a recognized phenomenon and should not be ignored. To reduce the occurrence of clip migration after biliary surgery, surgeons are advised to use the tissue clamp correctly, close the cystic duct completely, relax the gallbladder traction before clamping the tissue to avoid positioning the head end of the tissue clamp very close to the common bile duct, and use absorbable tissue clamps or absorbable sutures to close the stump of the cystic duct when obvious inflammation and edema of the cystic duct are present and the tissue is brittle.
Footnotes
Acknowledgements
We thank the patients for permitting us to use their data to complete this article.
Author contributions
XW and HY reviewed the literature and contributed to the manuscript drafting. XZ and SZ were responsible for revision of the manuscript for important intellectual content. KZ issued final approval for the version to be submitted. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declare no competing interests.
Ethics statement
The patients provided written informed consent for participation in this study and for publication of their clinical information and photographic material. The signed informed consent forms are available upon request. This study was approved by the Medical Ethics Committee Member of the People’s Hospital Affiliated to Ningbo University (approval number MR-33-21-014116).
Funding
This study was supported by the Zhejiang Medical Science and Technology Projects (2020370595). The funders had no role in the study design; collection, analysis, or reporting of data; preparation of the manuscript; or decision to submit for publication.