
Abstract
Objective
To test agreement and interchangeability between distal (dRA) and forearm radial arterial (RA) pressures (AP) during general anesthesia (GA) for prone spinal surgery.
Methods
This prospective observational study involved 40 patients scheduled for GA spinal surgery. The right dRA and left forearm RA were cannulated in all patients to continuously measure invasive blood pressures (IBP). We compared the agreement and trending ability of systolic AP (SAP), diastolic AP (DAP), and mean AP (MAP) at each site 15 minutes after tracheal intubation, start of surgery, 30 and 60 minutes after the start of surgery, and after skin suturing.
Results
Paired BP values (n = 184) (37 cases) were analyzed. The bias (standard deviation), limits of agreement, and percentage error were: SAP: 0.19 (3.03), −5.75 to 6.12, and 5.04%; DAP: −0.06 (1.75), −3.50 to 3.38, and 5.10%; and MAP: 0.08 (1.52), −2.90 to 3.05, and 3.54%, respectively. The linear regression coefficients of determination were 0.981, 0.982, and 0.988 for SAPs, DAPs, and MAPs, respectively; four-quadrant plot concordance rates were 95.11%, 92.03%, and 92.66%, respectively.
Conclusion
All arterial BPs showed good agreement and trending capabilities for both the dRA and RA. The dRA may be substituted for the RA in IBP monitoring.
Keywords
Introduction
Blood pressure (BP) is the key hemodynamic parameter for anesthesia management. 1 BP management in spinal surgery requires interdisciplinary cooperation between anesthetists and surgeons. 2 Appropriate arterial blood pressure maintains good spinal perfusion 3 and also reduces intraoperative bleeding. 4 Invasive blood pressure (IBP) monitoring is considered the “gold standard” for BP monitoring. 5
The forearm radial artery (RA) is the classic cannulation access in patients receiving general anesthesia (GA). 6 However, in prone spinal surgery, the patient’s upper arms are usually placed on an armrest, which may cause problems maintaining wrist extension. The use of the distal radial artery (dRA) is a rational alternative for patients with disorders of the elbow joint or who maintain their arms in nonergonomic positions for prolonged periods. 7
Poor agreement between arterial BP measurements at different measurement sites has been proven in awake people8,9 or in vasodilatory states during cardiac surgery.10,11 To date, the clinical differences between systolic arterial pressure (SAP), diastolic AP (DAP), and mean AP (MAP) from the dRA and RA approaches during prone spinal surgery under GA are not definitively known. The purpose of this study was to compare IBPs obtained at the two sites.
Methods
Ethical Considerations
This was a prospective, self-controlled, observational study performed at the Jinling Hospital, Nanjing, Jiangsu, China. The protocol was approved by the Ethics Committee of Jinling Hospital (approval number: 2021NZKY–013-02; approval date: 29 April 2021) and registered in the Chinese Clinical Trials Registry (registration number: ChiCTR2100043714; registration date: 27 February 2021). All participating patients provided written informed consent and the patients’ data were de-identified automatically. 12 The reporting of this study conforms to the STROBE guidelines. 13
Study population
Patients aged 30 to 70 years, with American Society of Anesthesiologists (ASA) class I to III, who were scheduled for more than 1 hour of elective prone spinal surgery under GA between March 2022 and July 2022 were enrolled consecutively. Patients were excluded if their arteries were nonpalpable or they had peripheral vascular disease, difficulty communicating, infected puncture site, blood coagulation disorders, negative modified Allen tests, body mass index (BMI) > 30 kg/m2, or systolic BP difference >10 mmHg between the upper limbs in either the supine or semirecumbent posture measured by noninvasive oscillometry.
Anesthesia and perioperative management
Before anesthesia and after initiating standard monitoring, the patients underwent left RA cannulation under local anesthesia (LA) to monitor IBP. Following preoxygenation, GA was induced with intravenous midazolam 0.02 to 0.03 mg/kg, propofol 1 to 3 mg/kg, sufentanil 0.2 to 0.3 µg/kg, and rocuronium bromide 0.6 to 0.8 mg/kg to facilitate tracheal intubation. Propofol was used for anesthesia maintenance, with continuous infusion of remifentanil, in accordance with the anesthetist’s judgment, and bispectral indices of 40 to 60. Lung ventilation was performed with volume-control mode and a tidal volume between 7 and 8 mL/kg to maintain blood oxygen saturation (SpO2) > 95% and end-tidal carbon dioxide (CO2) between 30 and 40 mmHg. An experienced operator performed the right dRA cannulation immediately after anesthesia induction. The patient was then moved to the prone “superman” position 14 with the upper arms resting on an armrest parallel to the patient’s longitudinal axis above the shoulders with the elbows flexed at < 90°.
The dRA and RA were identified by anatomical landmarks (the anatomical snuffbox and styloid process of the radius for the dRA and RA, respectively), and cannulated with identical 22-gauge, 25-mm-long arterial cannulation sets (B. Braun, Melsungen, Germany) using real-time ultrasound-guidance. The cannulation protocol was published previously. 7 Each catheter was attached to a pressure transducer (B. Braun) with standard 3-m-long connector tubing. The transducer system had one tap and one connector. The continuous flushing rate was 3 mL/hour, while the fast flushing rate was 1 mL/s. Both transducers were zeroed to atmospheric pressure and placed at the patient’s midaxillary line. Arterial pressure waveforms and SAP, DAP, and MAP were displayed simultaneously on patient monitors (Mindray, Shenzhen, China). MAP equals the area under the pressure wave averaged over the cardiac cycle, which depends on pressure wave contour. 15 The transducer system was checked for damping coefficients and natural frequencies using a fast flush test immediately before each measurement,1,16 and, if necessary, abnormal damping was corrected. The RA BP measurements were used as the basis for all therapeutic decisions.
Clinical and perioperative variables
The patients’ demographic information was obtained from hospital records and comprised age, sex, height, weight, body mass index (BMI), comorbidities, and current medication. Intraoperative data comprised anesthesia and surgery durations, as well as hemodynamic data, namely, SAP, DAP, and MAP.
SAP, DAP, and MAP readings from the dRA and RA were automatically recorded on a computer by an anesthesia information acquisition system (DoCare Co., Ltd., Beijing, China). SAP, DAP, and MAP measurements were obtained at five time points (Figure 1):
T1 (baseline), 15 minutes after tracheal intubation T2, at the start of surgery T3, 30 minutes after the start of surgery T4, 1 hour after the start of surgery T5, at the completion of skin suturing.

Diagram illustrating the study design. dRA, distal radial artery; RA, forearm radial artery; BP, blood pressure.
Ten readings were recorded from both the dRA and RA at 1-minute intervals at each time point. The mean BP value over five consecutive beats was recorded to reduce the effects of respiration. 17
The primary outcome was the assessment of the agreement of SAP, DAP and MAP values between the dRA and RA approaches using Bland–Altman analysis. The secondary outcome was the tracking ability of each hemodynamic variable compared between the two approaches.
Sample size
The Bland–Altman method does not specify sample size as it is not a conventional statistical test, 18 and there are no requirements regarding patient or measurement numbers for studies in which repeated measurements are compared. 19 Therefore, we used the methods reported in previous studies17,20 and analyzed over 150 paired measurements, which was considered sufficient for adequate interpretation of the study findings.
Statistical analysis
Continuous data are presented as means ± standard deviations (SD) and categorical data as numbers and percentages. The Bland–Altman method was used to assess agreement between paired BP values, representing the primary outcome.
21
Bias, representing systematic error, was determined as the mean difference between the two BP measurement approaches. Precision, representing variability or random error between the approaches, was determined as the SD of the bias. In accordance with the guidelines of the Association for the Advancement of Medical Instrumentation,
22
a bias value of <5 mmHg was considered acceptable. The limits of agreement (LOA) represented the bias ±1.96 SD and defined the expected range of 95% of the difference between the approaches. The percentage error was used as an interchangeability criterion.
22
percentage error =
For the measurement of the secondary outcome, the tracking ability of the two measurements was evaluated using four-quadrant plots, with presentation of the results as the concordance rate. 23 The concordance between the two deltas was analyzed, 24 representing the dRA and RA, respectively, with each delta indicating changes between two consecutive readings. The concordance rate was determined as the ratio of data within the upper right or lower left quadrants on the four-quadrant plot, 23 with an exclusion zone of 5 mmHg. 24 The exclusion zone excluded the very small AP changes driven by noise and improved the signal/noise ratio.
All statistical analyses were performed using Microsoft Excel 2007 (Microsoft Inc., Redmond, WA, USA), GraphPad Prism 7 (GraphPad Software, Inc., La Jolla, CA, USA), and R version 4.2.1 (www.r-project.org). P < 0.05 was considered statistically significant.
Results
Patients
Forty patients who were scheduled to undergo elective spinal surgery under GA were initially recruited. Of these, one patient withdrew from the study, and two others were withdrawn owing to technical difficulties with arterial catheter insertion. Table 1 contains the demographic and intraoperative data of the remaining 37 patients. In all, 185 paired measurements using the dRA and RA approaches were obtained from the 37 patients, of which 184 were used in the final analysis, excluding measurement errors (Figure 2).
Demographic and intraoperative data.

SD, standard deviation; BMI, body mass index; ASA, American Society of Anesthesiologists.
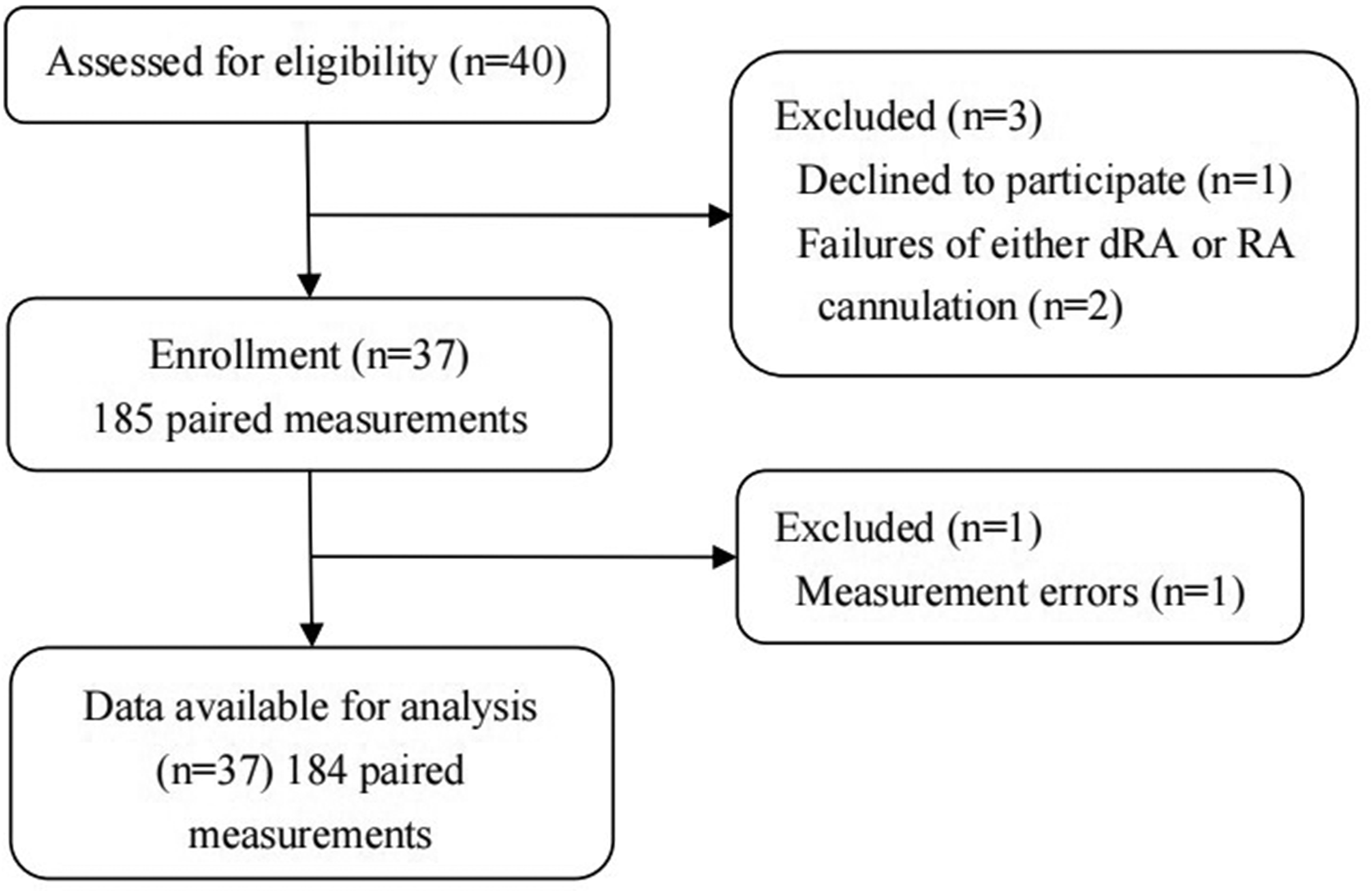
Study flow chart. dRA, distal radial artery; RA, forearm radial artery.
Analysis of agreement
Supplemental Table 1 shows the distribution of BP measurements. In the Bland–Altman analysis, the bias (SD) and LOA were 0.19 (3.03) and −5.75 to 6.12 for SAP; −0.06 (1.75) and −3.50 to 3.38 for DAP; and 0.08 (1.52) and −2.90 to 3.05 for MAP, respectively. The percentage errors were 5.04%, 5.10%, and 3.54% for SAP, DAP, and MAP, respectively (Table 2, Figure 3). Linear regression analysis showed a high coefficient of determination between SAPs (R 2 = 0.981; P<0.001), DAPs (R 2 = 0.982; P<0.001), and MAPs (R 2 = 0.988; P<0.001).
Agreement in blood pressure readings between the dRA and RA approaches.

Data are presented as means ± SD unless otherwise stated.
dRA, distal radial artery; RA, radial artery; SD, standard deviation; LOA, limits of agreement; BP, blood pressure.
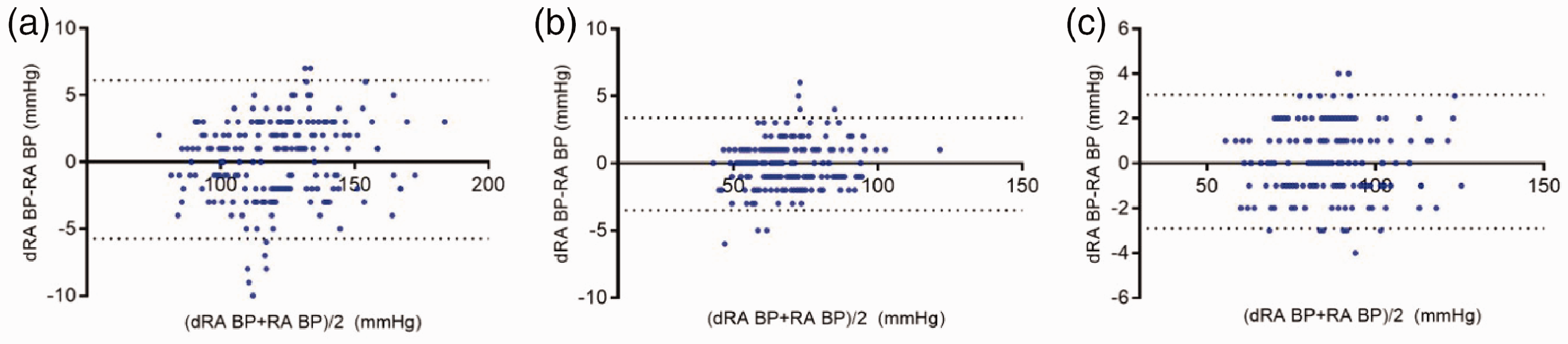
Bland–Altman plot for repeated measures, with 95% limits of agreement (dotted lines). The horizontal and vertical axes indicate the means and differences in BP values obtained using the dRA and RA approaches, respectively. (a) SAP, (b) DAP, and (c) MAP. BP, blood pressure; dRA, distal radial artery; RA, forearm radial artery; SAP, systolic arterial pressure; DAP, diastolic arterial pressure; MAP, mean arterial pressure.
Analysis of trending ability
The trending abilities of the hemodynamic variables were analyzed by four-quadrant plots. The concordance rates for SAP, DAP, and MAP were 95.11%, 92.03%, and 92.66%, respectively (Figure 4).
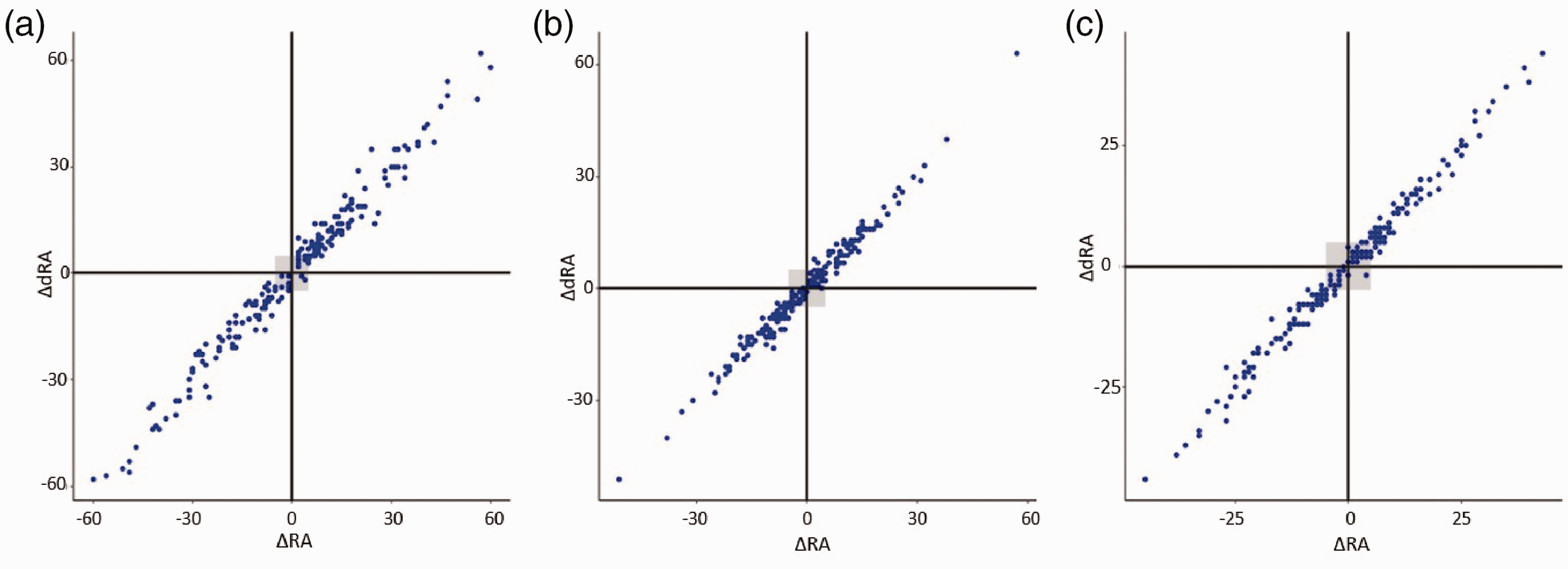
Four-quadrant plots showing trending agreements between the dRA and RA measurements. Exclusion zones were 5 mmHg. The horizontal and vertical axes indicate the changes in blood pressure between two consecutive readings using the dRA and RA approaches, respectively. (a) SAP, (b) DAP, and (c) MAP. dRA, distal radial artery; RA, forearm radial artery; SAP, systolic arterial pressure; DAP, diastolic arterial pressure; MAP, mean arterial pressure.
Discussion
BP is a complex physiological variable. After ventricular ejection, a pressure wave propagates from the large elastic central arteries to smaller muscular arteries in the periphery. This has important implications for anesthetic practice, as measured AP is a primary determinant of fluid and vasopressor administration. Anesthetists and intensivists recognize peripheral BP, usually forearm RA BP, as the clinical reference for central BP.
The novel dRA approach builds on the advantages of the RA approach. The use of the dRA also maintains and preserves the integrity of the RA for future cannulation.25,26 A further advantage is that wrist flexion in the prone and lateral decubitus positions has less influence on arterial waveforms in the dRA compared with the RA, 27 as cannulation of the dRA at the anatomical snuffbox allows pronation of the patient’s forearm. 28
Scientists have proposed various statistical methods to assess the equivalence29,30 between new measures and a gold standard. The Bland–Altman analysis is based on the accuracy of the new method, difference compared with the gold standard, and the average of the two methods. Recently, Bland–Altman analysis has been extended to clinical studies in repeated measures analyses. 31 For example, Asamoto et al 32 used this method to evaluate the accuracy and equivalence of minimally invasive continuous cardiac displacement monitoring in two different procedures. However, the Bland–Altman analysis does not consider the order of the observed data. The four-quadrant plot mainly focuses on the trend of the difference in two values between the new method and the gold standard.
In the present study, we evaluated the accuracy and trending ability of dRA compared with RA measurements in adult patients during prone spinal surgery under GA. Our main finding was that SAP, DAP, and MAP showed statistically significant agreement between the two approaches, with small mean ± SD differences between the dRA and RA measurements. Furthermore, SAP, DAP, and MAP all showed good trending, with very few discordant measurements and high concordance rates. These results may indicate that the dRA BP values were accurate for routine clinical use.
The guidelines for the noninvasive measurement of AP provided by the Association for the Advancement of Medical Instrumentation recommend an agreement of 5 mmHg (± 8 mmHg) in comparisons between a test and a reference method. 33 A large observational study 34 that compared noninvasive oscillometric measurements with invasive arterial BP readings reported differences as high as 10 mmHg in MAP values. However, our study compared two invasive BPs and revealed that the bias and SD between dRA and RA approaches were much lower than 5 mmHg. Additionally, good precision with small SD values were found for dRA. We also verified that the dRA approach was reliable for tracking BP changes. All R2 coefficients of the dRA and RA values were high, and regression relationships did not change with either low or high BP readings. These results indicate good consistency between dRA and RA measurements.
The effect of cannula site on the accuracy of AP measurements has been studied in numerous settings. In patients that have not been anesthetized, there can be significant amplification of SBP from central to peripheral arteries.8,9 Higher SAP and pulse pressures have been reported in the dorsalis pedis artery (DPA) compared with the RA; however, DAP and MAP remain relatively constant.35,36 We assumed that the dRA would also exhibit this amplification phenomenon compared with the RA, considering that the dRA is the distal part of the RA. However, the SAP, DAP, and MAP readings did not differ significantly between the two sites (P = 0.462, 0.705, and 0.638, respectively). A possible explanation is that the dRA is a somewhat smaller downstream extension of the RA and has abundant collateral circulation. Moreover, patients in our study were under GA, which may have resulted in fewer unstable factors compared with sedated or awake patients. Furthermore, the systemic vascular dilation effect of anesthetic drugs should not be ignored.
There are several limitations in this study. First, this was an observational and self-controlled study. We originally planned to perform all BP measurements using the same arm to avoid confounding by interarm BP differences. However, it was difficult to determine the presence and potential impact of partial blood flow obstruction in the dRA from the upstream RA cannulation. Eventually, we decided to reduce bias associated with blood flow in both upper limbs by excluding patients with oscillometric BP differences >10 mmHg. Second, this study involved a cohort of patients who underwent a particular surgical type at a single center, and the small sample size could have affected analysis of the agreement between the two BP sites. Therefore, the generalizability and bias of these findings remain debatable. Large-sample and multi-center studies in different clinical situations are needed. Third, the clinical standards for spinal surgery mandate that BP values be maintained within a narrow range, preventing the use of an error grid analysis, as suggested by Saugel et al. 37 Fourth, intraoperative blood loss, volumes of administered blood products, and precise use of vasopressors were not documented. However, precise correlations between BP readings and actual fluid balance are frequently not determined, clinically. 38 Fifth, we did not determine the catheter frequency response, in accordance with the ARTERY Society guidelines, 39 which is needed to assure data quality control. Finally, agreements between the approaches were evaluated using Bland–Altman analysis and four-quadrant plots. These methods’ criteria for precision (such as bias within 5 mmHg or 20% percentage error)21,23 have been developed largely for the measurement of cardiac output and noninvasive BP assessments. Thus, there is no standardized method for determining agreement between IBP measurements.
Conclusion
SAP, DAP, and MAP all showed good agreements and trending abilities with dRA BP measurements compared with RA BP measurements in prone spinal surgeries under GA. Thus, if RA monitoring is unavailable, the dRA may be a suitable and reliable substitute.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231188285 - Supplemental material for Agreement between distal and forearm radial arterial pressures in patients undergoing prone spinal surgery: a prospective, self-controlled, observational study
Supplemental material, sj-pdf-1-imr-10.1177_03000605231188285 for Agreement between distal and forearm radial arterial pressures in patients undergoing prone spinal surgery: a prospective, self-controlled, observational study by Jingwei Xiong, Miaomiao Xu, Kangli Hui, Jiejie Zhou, Jie Zhang, Manlin Duan and Lidong Zhang in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605231188285 - Supplemental material for Agreement between distal and forearm radial arterial pressures in patients undergoing prone spinal surgery: a prospective, self-controlled, observational study
Supplemental material, sj-pdf-2-imr-10.1177_03000605231188285 for Agreement between distal and forearm radial arterial pressures in patients undergoing prone spinal surgery: a prospective, self-controlled, observational study by Jingwei Xiong, Miaomiao Xu, Kangli Hui, Jiejie Zhou, Jie Zhang, Manlin Duan and Lidong Zhang in Journal of International Medical Research
Supplemental Material
sj-pdf-3-imr-10.1177_03000605231188285 - Supplemental material for Agreement between distal and forearm radial arterial pressures in patients undergoing prone spinal surgery: a prospective, self-controlled, observational study
Supplemental material, sj-pdf-3-imr-10.1177_03000605231188285 for Agreement between distal and forearm radial arterial pressures in patients undergoing prone spinal surgery: a prospective, self-controlled, observational study by Jingwei Xiong, Miaomiao Xu, Kangli Hui, Jiejie Zhou, Jie Zhang, Manlin Duan and Lidong Zhang in Journal of International Medical Research
Footnotes
Acknowledgements
The authors would like to thank all participants involved in this research.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author Contributions
Jingwei Xiong analyzed the data and wrote the manuscript. Miaomiao Xu, Kangli Hui, and Jiejie Zhou collected the data. Jie Zhang assisted in the performance of the study. Manlin Duan was the principal investigator and supervised the study. Lidong Zhang helped revise the manuscript. All authors read and approved the final manuscript.
Data availability
Data are available from the authors on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.