
Abstract
Objective
Methylene blue (MB) and spring microcoils are used for the preoperative localization of small pulmonary nodules (SPNs). We aimed to compare the efficacy and safety of these methods using published data.
Methods
We identified randomized controlled trials and observational studies that assessed preoperative SPN localization using MB or spring microcoil and compared these using a meta-analysis.
Results
Seven studies of 933 patients were identified, in whom 1081 SPNs were located. Four hundred twenty-four SPNs were located using MB (n = 359 participants), and 657 SPNs were located using the spring microcoil method (n = 574 participants). The prevalence of technical success of SPN localization was higher using MB (mean deviation [MD]: 0.43; 95% confidence interval [CI]: 0.20, 0.93); the incidence of postoperative complications was lower (MD: 1.70; 95% CI: 1.09, 2.65); and the time taken for removal was longer (MD: −12.37; 95% CI: −22.60, −2.13). There were no differences with respect to the successful wedge resection rate, the time taken for localization, the duration of the procedure, or the mean hospital stay.
Conclusions
Both methods can detect SPNs; however, MB is associated with a higher success rate and fewer postoperative complications, while spring microcoil localization is associated with more rapid removal.
Keywords
Introduction
Early screening can reduce the risk of mortality in patients with lung cancer. Advancements in imaging technology and the popularization of high-resolution computed tomography (CT) for the physical examination of masses has resulted in the detection of many asymptomatic small pulmonary nodules (SPNs). SPNs are revealed on CT as high-density shadows in the lung parenchyma of ≤30 mm that are not associated with pathologies, such as atelectasis, lymphadenopathy, and pleural effusion.1,2 Pathological diagnosis is the gold-standard method for the diagnosis of SPNs; therefore, after CT screening, SPNs are removed using video-assisted thoracoscopic surgery (VATS) and tissue samples are examined to facilitate early diagnosis and treatment.3,4 SPNs can be detected using preoperative CT scans, visual observation, or palpation during surgery, but are often inaccessible, which makes the surgery more difficult and conversion to open chest surgery may be necessary if the SPNs cannot be examined pathologically. Therefore, a good localization method is necessary to facilitate the thoracoscopic treatment of such nodules.
Intraoperative ultrasonography, tactile sensor localization, preoperative CT-guided methylene blue (MB) staining, hook wire, spring microcoil, and crochet are commonly used localization methods,5–8 and each has specific advantages and disadvantages. To date, the optimal localization method has not been identified, but the most commonly used methods are the microcoil, hook wire, and MB localization. Previous studies have shown that all three methods have a high success rate (>90%),9–11 but the prevalence of adverse events in patients with SPNs who undergo hook wire localization can be as high as 90%. In contrast, the MB and spring microcoil methods are associated with significantly lower incidences of complications, including pneumothorax, pleural bleeding, and pleural fluid leakage, during SPN resection (13%–55%).12,13 Of these, pneumothorax is the most common, and the overall prevalence of pneumothorax in the present study was 38.4% 14 . Nevertheless, the efficacy and safety of MB and spring microcoil localization have not been systematically evaluated. Therefore, we aimed to evaluate the published data regarding the use of these methods and to systematically compare their efficacy and safety. We followed the relevant guidelines available at www.bmj.com/content/372/bmj.n160.
Materials and Methods
Search strategy
We searched the following databases for articles published between the establishment of the database and 15 October 2022: Medline via PubMed, Embase, Cochrane, CENTRAL, CINAHL, Web of Science, China Biomedical Literature (CNKI), the Chinese Science and Technology Periodical Database (VIP), and Wanfang. The following search terms were used, connected with OR/AND: “pulmonary nodules,” “small pulmonary nodules,” “solitary pulmonary nodules,” “multiple pulmonary nodules,” “pulmonary nodulectomy,” “CT-guided,” “methylene blue localization,” “methylene blue,” “coil localization,” “coil,” “spring micro coil,” and “micro coil”. For example, in Medline via PubMed, the search strategy was: (Pulmonary nodules OR small pulmonary nodules OR solitary pulmonary nodules OR multiple pulmonary nodules OR pulmonary nodulectomy) AND (CT-guided OR methylene blue localization OR methylene blue); (Pulmonary nodules OR small pulmonary nodules OR solitary pulmonary nodules OR multiple pulmonary nodules OR coil OR spring micro coil OR micro coil) AND (CT-guided OR coil localization OR methylene blue). All the relevant studies were retrieved and their full texts were downloaded.
Inclusion criteria
Research articles were included if the studies described were clinical controlled trials, retrospective cohort studies, or case–control studies; if there was a diagnosis of pulmonary sarcoidosis (excluding lung cancer with a definitive diagnosis; and if the full text was available in Chinese or English.
Exclusion criteria
Articles were excluded if the study groups were not clearly defined; if they featured other study designs, such as data analysis studies and case reports; if they were duplicates or animal experiments; if metastatic pulmonary nodules were included; and if conservative or non-invasive treatment was used.
Risk of bias assessment
Two researchers independently examined the included articles using the RevMan 5.4 software risk of bias assessment tool (The Cochrane Collaboration, Copenhagen, Denmark). The assessment included seven items: random allocation method, allocation scheme concealment, blinding method for the research objective and investigator, blinding method for the outcomes, integrity of the data, selectivity of reporting, and other biases. Each item was rated as “low risk,” “high risk,” or “unclear”.
Clinical outcomes
The following clinical outcomes were extracted: prevalence of the technical success of localization, prevalence of successful wedge resection, time taken for localization, time taken to remove the nodule during surgery, mean hospital stay, and the incidence of postoperative complications (including pneumothorax, pleural effusion, continuous hemoptysis, and pleural reaction).
Statistical analysis
RevMan 5.4 software was used for the meta-analysis. The mean difference (MD) was used as the combined outcome index for continuous variables. We used the Q test for qualitative analyses and the I2 test for quantitative analyses to determine the heterogeneity of the data. If P > 0.1 and I2 ≤ 50%, the data were considered to be homogeneous, and a fixed effects model was used for the meta-analysis. P ≤ 0.1 and I2 > 50% was regarded as indicating high heterogeneity among the studies, and in these instances a random effects model was used for the meta-analysis. For all variables for which the data were highly heterogeneous, subgroup or sensitivity analyses were used to explore the source of the heterogeneity. When comparing datasets, P < 0.05 was considered to represent statistical significance.
Results
Included studies
Eight hundred twenty-five papers were initially retrieved, and duplicates (n = 248) were removed using EndNote (Clarivate, London, UK) and NoteExpress (http://www.inoteexpress.com/index.htm#Home). The titles and abstracts of the included studies were screened against the inclusion and exclusion criteria, and 545 articles were excluded. Full-text reviews of the remaining 32 articles were then performed, from among which seven studies were selected for inclusion in the meta-analysis. The included studies consisted of two retrospective case–control studies and five retrospective cohort studies.14–20 Of the participants, 359 were in the MB group (424 SPNs) and 574 were in the spring microcoil group (657 SPNs). The screening process is shown in Figure 1 and the characteristics of the included studies are shown in Table 1. The results of the risk of bias assessments are shown in Figure 2. The overall risk was controllable, and a meta-analysis was conducted.

Flow chart of the literature screening.
Basic characteristics of the included studies.
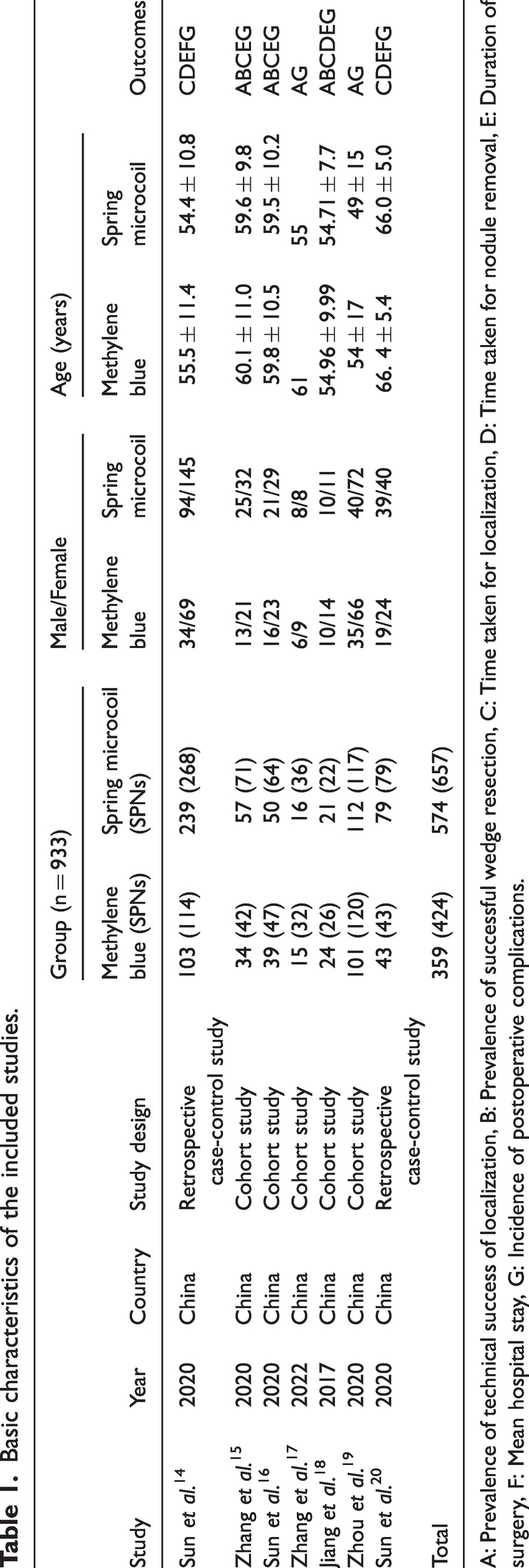
A: Prevalence of technical success of localization, B: Prevalence of successful wedge resection, C: Time taken for localization, D: Time taken for nodule removal, E: Duration of surgery, F: Mean hospital stay, G: Incidence of postoperative complications.
Complications during the included studies.


Results of the risk of bias assessment for the included studies.
Technical success of localization rate
In five studies, a detailed comparison of the technical success of the localization of SPNs was performed, as shown in Figure 3. There was a low level of heterogeneity among these studies, and therefore a fixed effects model was used for the meta-analysis. The prevalence of technical success of the localization of SPNs using the spring microcoil method was lower than that using the MB method (MD: 0.43; 95% confidence interval [CI]: 0.20, 0.93; z = 2.13; P = 0.03).
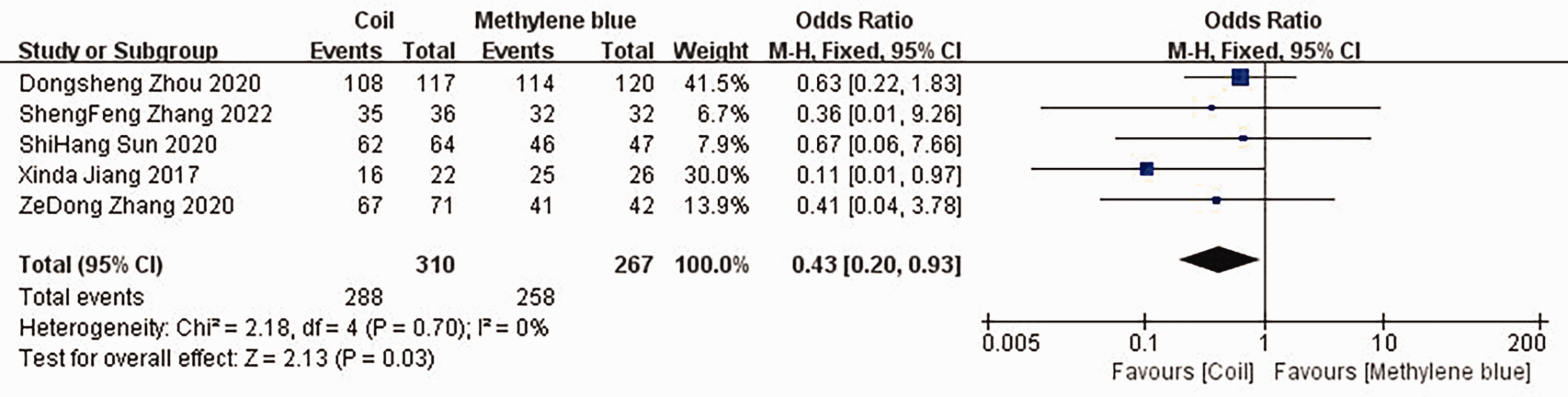
Forest plot showing the prevalence of technical success of localization for the two groups
Prevalence of successful wedge resection
In three studies, the prevalence of successful wedge resection for the treatment of SPNs associated with the two methods was compared, as shown in Figure 4. There was low heterogeneity among the studies, and therefore a fixed effects model was used for the meta-analysis. There was no significant difference in the prevalence of successful wedge resection between the coil group and the MB group (MD: 0.30; 95% CI: 0.08, 1.18; z = 1.73; P = 0.08).
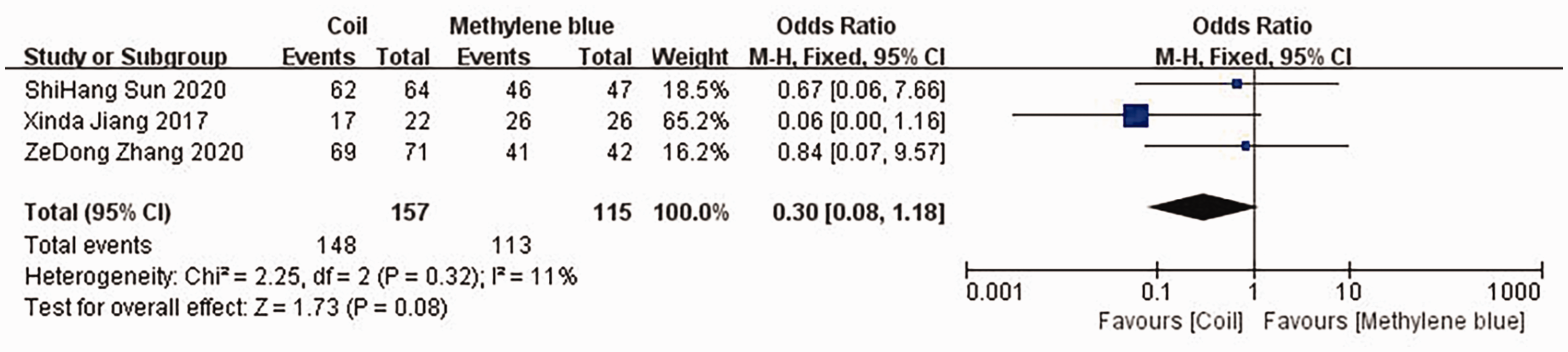
Forest plot showing the prevalence of successful wedge resection for the two groups.
Time taken for the localization
In five studies, the time taken for the localization of the SPNs was compared, as shown in Figure 5. There was high heterogeneity among the studies, and therefore, a random effects model was used for the meta-analysis. There was no significant difference in the time taken for localization between the microcoil and MB groups (MD: 1.01; 95% CI: −0.20, 2.22; z = 1.63; P = 0.10).

Forest plot of the time taken for localization (in minutes) for the two groups.
Time taken to remove the SPNs during surgery
In three studies, the time taken for nodule removal during surgery was compared, as shown in Figure 6. A low level of heterogeneity was found among the studies, and therefore, a fixed effects model was used for the meta-analysis. The time taken for pulmonary nodule removal in the coil group was shorter than that in the MB group (MD: −12.37; 95% CI: −22.60, −2.13; z = 2.37; P = 0.02).

Forest plot of the duration of nodule resection (in minutes) during surgery for the two groups.
Duration of surgery
In five studies, a comparison of the duration of surgery was made between the two groups (see Figure 7). The studies were highly heterogeneous, and therefore a random effects model was used for the meta-analysis. The difference in the duration of surgery between the microcoil and MB groups was not significant (MD: −1.81; 95% CI: −24.24, 20.61; z = 0.16; P = 0.87).
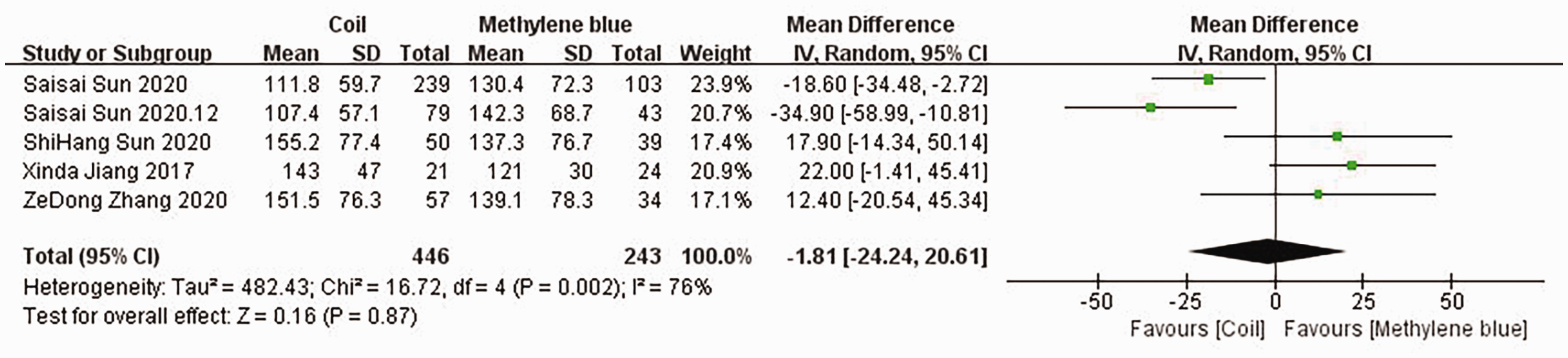
Forest plot of the duration of surgery (in minutes) for the two groups.
Mean hospital stay
In two studies, the mean hospital stay was compared between the two groups, as shown in Figure 8. The level of heterogeneity between the studies was low, and therefore a fixed effects model was used for the meta-analysis. The mean hospital stay did not differ between the microcoil and MB groups (MD: −0.09; 95% CI: −0.80, 0.62; z = 0.25; P = 0.80).

Forest plot of the mean hospital stay (in days) for the two groups.
Incidence of postoperative complications
In seven studies, a detailed comparison of the incidence of postoperative complications was made (see Figure 9). There was a low level of heterogeneity among the studies, and therefore a fixed effects model was used for the meta-analysis. The incidence of postoperative complications in the coil group was higher than that in the MB group (MD: 1.70; 95% CI: 1.09, 2.65; z = 2.36; P = 0.02).
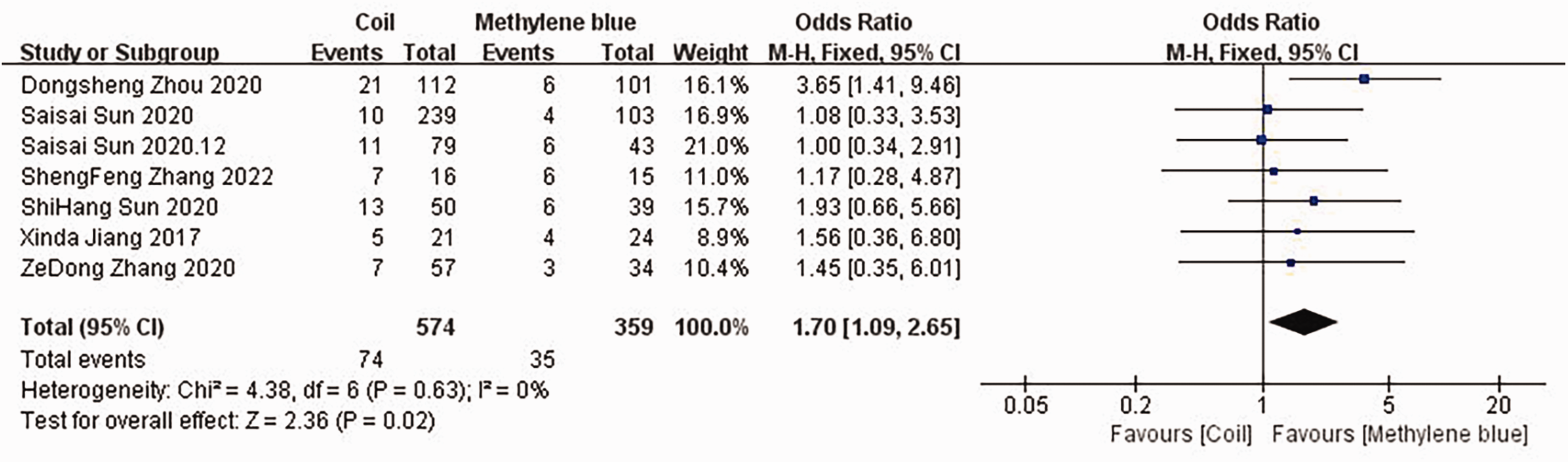
Forest plot of the incidence of postoperative complications for the two groups.
Discussion
Preoperative CT-guided localization is often used to guide the resection of peripheral SPNs using VATS lobectomy, and the use of these localization methods can reduce the likelihood of a thoracotomy being necessary. Compared with the conventional SPN localization methods, such as the hook method, the MB and microcoil methods are more reliable, are technically simpler, and are safer.21,22 MB is commonly used to treat methemoglobinemia, and after absorption, it is discharged in the urine without being metabolized; therefore, it is safe to use at low doses. MB is a blue aqueous solution that is often used in the diagnosis of anastomotic leakage during thoracic surgery. The MB method is also much cheaper than the hook wire, spring microcoil, and other localization methods. Prior to surgery, MB is injected into the abnormal lung tissue to dye it blue and thereby distinguish it from the surrounding normal lung tissue.23,24 After this process, the MB diffuses into the lung tissue, which means that size of the wedge resection is larger than the nodules. Typically, the resection margin is not positive; however, the use of MB might result in excessive resection of normal lung tissue. To prevent this, surgery should be performed as soon as possible after localization. According to the results of previous studies, the time elapsed between MB injection and the start of surgery should not exceed 3 hours, which prevents localization failures caused by MB diffusion and absorption.23,25–27 Yu et al. 28 proposed that the use of a combination of MB and a hook wire would reduce localization failure caused by the diffusion and fading of the MB secondary to a long period of time between injection and surgery. Furthermore, some patients have dark lung surfaces because of long-term smoking, which results in poor differentiation between the MB-stained area and surrounding lung tissue following MB injection, thereby increasing the difficulty of the surgery.
Spring microcoils are embolic spring coils that are used for the treatment of vascular embolism and can be retained in the human body for a long time after surgery. 29 Prior to surgery, the spring microcoil is positioned under CT guidance: one end of the coil is placed around the pulmonary nodule and the other end is placed in the pleural cavity. Because these coils are elastic, the head ends on both sides can be opened and rotated into a dumbbell shape, or they can both be placed in the lung and opened to form a circle. Because the coil is harder than the lung tissue, the pulmonary nodule can be localized through visual inspection, palpation, and other methods during surgery.1,11,30 The spring microcoil localization method is similar to the MB method and other preoperative localization methods, in that it can cause pneumothorax, pulmonary hemorrhage, pleural reaction, and other complications. Compared with MB staining, the spring microcoil is more stable after positioning and the time elapsed between positioning and the start of surgery can be longer; for example, the coil can be placed in the evening prior to the day of the surgery.31–33 This may avoid the problems of conflicting schedules among thoracic surgeons and radiologists, and the scheduling of operating rooms, and facilitate the activities of a multi-disciplinary team. Liu et al. proposed that a combination of CT and digital subtraction angiography (DSA) should be used to guide the localization of SPNs using the spring microcoil method and that fluoroscopy should be used to assist with the location of the coil during surgery. 34 Positive margins and foreign bodies caused by wire cutting have been reported following preoperative CT-guided hook wire localization, 35 and spring microcoil localization is associated with the same risks.
In the present study, through comprehensive analyses of published studies in which the MB and spring microcoil methods were compared, we found no significant differences in the prevalence of successful wedge resection, the time taken for intraoperative positioning, the duration of surgery, or the mean hospital stay (P < 0.05) between these two methods. The MB method was associated with a higher prevalence of successful localization of pulmonary nodules, a lower incidence of postoperative complications, and a longer duration of resection (P < 0.05) than the spring microcoil method. Thus, both methods have advantages and disadvantages, and clinicians and radiologists should select the appropriate method according to the specific situation of the patient.
The present study had a few limitations. First, most of the included studies were retrospective studies, and therefore were more vulnerable to potential bias. Second, the included studies were small, and therefore more clinical trials should be performed to improve the statistical power and the reliability of the conclusions. Third, although the baseline data of the two groups were comparable, some of the included studies did not include participants with multiple pulmonary nodules, but rather a single nodule. This could have contributed to selection bias. Further prospective randomized controlled trials are required to verify these findings.
Conclusion
Both the MB and spring microcoil localization methods are effective means of localizing SPNs during surgery. However, MB localization is associated with a higher success rate and fewer postoperative complications. The spring microcoil localization method is associated with the rapid removal of SPNs during surgery. The two localization methods have specific advantages that clinicians should consider to select the best approach for each patient.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231187938 - Supplemental material for Use of methylene blue and a spring microcoil in the preoperative localization of small pulmonary nodules under CT guidance: a meta-analysis
Supplemental material, sj-pdf-1-imr-10.1177_03000605231187938 for Use of methylene blue and a spring microcoil in the preoperative localization of small pulmonary nodules under CT guidance: a meta-analysis by Mengchen Wang, Yikang Yu, Lu Li and Chenfeng Qian in Journal of International Medical Research
Footnotes
Author Contributions
MW drafted the manuscript and was responsible for document retrieval and data processing; CQ was responsible for checking the included indicators; LL obtained funding for the research; and YY designed the figures.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was funded by a Science and Technology Project of the Jinhua Science and Technology Bureau (project no.: 2021-3-041).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.