
Abstract
Objective
To evaluate the efficacy of methylene blue in preventing recurrent symptomatic postoperative adhesions.
Methods
Patients with a history of >2 surgeries for intra-abdominal adhesion-related complications were selected for this study. Adhesiolysis surgery was subsequently performed using administration of 1% methylene blue. The follow-up period was 28.5 ± 11.1 months.
Results
Data were available from 20 patients (seven men and 13 women) whose mean ± SD age was 51.2 ± 11.4 years. Adhesions took longer to become symptomatic after the first abdominal surgery when the initial pathology was malignant compared with benign. However, the recurrence of adhesions after a previous adhesiolysis surgery had a similar time onset regardless of the initial disease. Following adhesiolysis surgery with methylene blue, the majority of patients did not present with symptoms associated with adhesion complications (i.e., chronic abdominal pain, bowel obstruction) for the length of the follow-up period.
Conclusions
The use of methylene blue during adhesiolysis surgery appears to reduce the recurrence of adhesion-related symptoms, suggesting a beneficial effect in the prevention of adhesion formation.
Introduction
Peritoneal adhesions are one of the most common postoperative complications following classical or laparoscopic abdominal and pelvic surgery. The rate of postoperative adhesion formation is high and studies indicate that they occur in 50–100% of cases1,2 and have even higher recurrence rates (85–93%).3,4Complications generated by postoperative adhesions can result in significant health problems. For example, 40% of all bowel obstructions and 65–75% of small bowel obstructions are caused by postoperative peritoneal adhesions. 5 Additionally, 40% of cases of chronic postoperative abdominal pain occur solely as a result of peritoneal adhesions with another 25% having peritoneal adhesions as one of the causative factors.6,7,8 One study suggested that peritoneal adhesions are responsible for secondary infertility in women in 15–20% of cases 9 whereas other reports suggest that they are causative in 40–50% of cases.10,11
Several strategies have been suggested as methods of reducing the rate of post-operative peritoneal adhesion formation. They include: use of minimally invasive surgical procedures; minimal operation time; reduction of light exposure and thermal peritoneal procedures; reduction of peritoneal bleeding; evacuation of haematic fluid collection and lavage of the abdominal cavity; avoidance of peritoneal trauma by coagulation or dehydration; prevention of septic contamination; minimal use of alloplastic materials inside the peritoneal cavity (i.e., mesh, sutures, drainage tubes, talc from surgical gloves); use of various anti-adhesive substances.12,13 For recurrent adhesions, especially in cases where high-grade adhesions are present, some of the aforementioned recommendations cannot be applied. For these patients, the use of adhesion-reducing adjuvants may be considered and various substances have been used, including saline, dextran, heparin, hyaluronic acid. 1 Data from several studies suggest that icodextrin or hyaluronic acid-carboxymethylcellulose (HA–CMC) are effective adhesion-inhibiting substances. 14 However, these agents are expensive and so the present study was designed to investigate the effectiveness of methylene blue as an anti-adhesive agent.
Methods
This was a retrospective analysis of data collected from patients that presented with bowel obstruction or chronic abdominal pain syndrome, secondary to grade IV generalized abdominal adhesions (according to the Bhatia classification) 15 between January 2011 and December 2015 at the Emergency City Hospital of Timisoara, Romania. Inclusion criteria were: intra-abdominal adhesions (grade IV according to the Bhatia classification) 15 following surgical treatment for either a non-malignant or malignant pathology; at least two open adhesiolysis surgeries without the use of methylene blue; recurrent symptoms. Patients excluded from the study included those with positive cytology and/or peritoneal biopsy for malignancy, abdominal mesh or other alloplastic material repairs, and/or septic contamination of the peritoneal cavity after the opening of an intestinal loop during adhesiolysis during the previous surgery.
Eligible patients had subsequently undergone adhesiolysis surgery using methylene blue. Following open surgery through blunt or sharp dissection, 50 ml methylene blue (1%) had been instilled into the abdominal cavity and the abdominal wound had been closed. After 12 h, a drainage tube was unclamped for 48 h. The patients’ vital signs (i.e., blood pressure, body temperature, oxygen saturation and urine output), postoperative wound and the aspect and quantity of drained fluid were monitored until the first post-operative bowel movement had occurred. Postoperative pain was quantified using an audio-visual scale 16 and haemoglobin, white blood cell count, and hepatic and renal parameters were recorded. Short- and long-term complications suggestive of a recurrence of intra-abdominal adhesions (e.g., chronic abdominal pain, complete or incomplete bowel obstruction) were also monitored. Patients’ medical records were retrospectively reviewed by an investigator (M.I.) for baseline demographic characteristics and operative data after the procedure.
Patient written informed consent was obtained and approval for the study was obtained from the Ethics Committee of Emergency City Hospital, Timisoara, Romania.
Statistical analyses
Statistical analyses were performed using SPSS software (version 21.0 for Windows®; (IBM SPSS, Armonk, NY: IBM Corp, USA) and a P-value < 0.05 was considered to indicate statistical significance.
Continuous variables were expressed as mean ± standard deviation (SD) and range. Student’s t-test, χ2 analysis, Fischer’s exact test and Wilcoxon signed-rank test were used for establishing statistical significance between variables.
Results
Data were available from 20 patients (seven men and 13 women) whose mean ± SD age was 51.2 ± 11.4 years. Initial pathology that required surgical intervention was classified according to the malignant or non-malignant (i.e., benign) characteristics of the disease. For malignant disease, the origin was described as either gastrointestinal (GI) or gynaecological, while benign disorders included abdominal wall defects or sepsis of the reproductive or GI tracts. Patient characteristics according to initial diagnosis are shown in Table 1. Of the 20 patients, 11 had malignant disease and nine had benign disease.
Distribution of patients with intra-abdominal adhesions following surgical treatment for either a non-malignant or malignant pathology
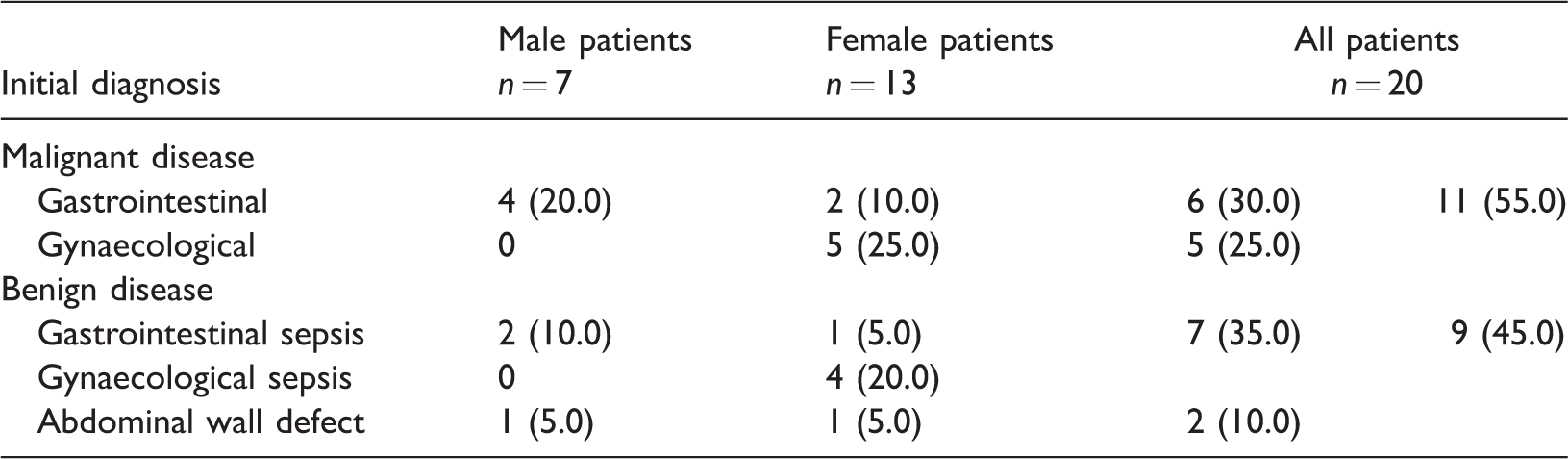
Values are shown as n (%)
During the postoperative period after the initial surgery, all patients developed abdominal adhesions that required a further operation. Across all patients, the number of adhesiolysis surgeries required after the initial surgery was 2.6 ± 0.6 (range, 2–4); 11 (55%) patients underwent two surgeries, 8 (40%) patients had three surgical interventions and one patient had four surgeries. On admission, 16 (80%) patients had presented with bowel obstruction (six complete, 10 incomplete). In addition, four (20%) patients reported chronic pain following surgery that had not responded to standard treatment options. All patients had been examined to exclude other pathologies that may have been responsible for their clinical manifestations.
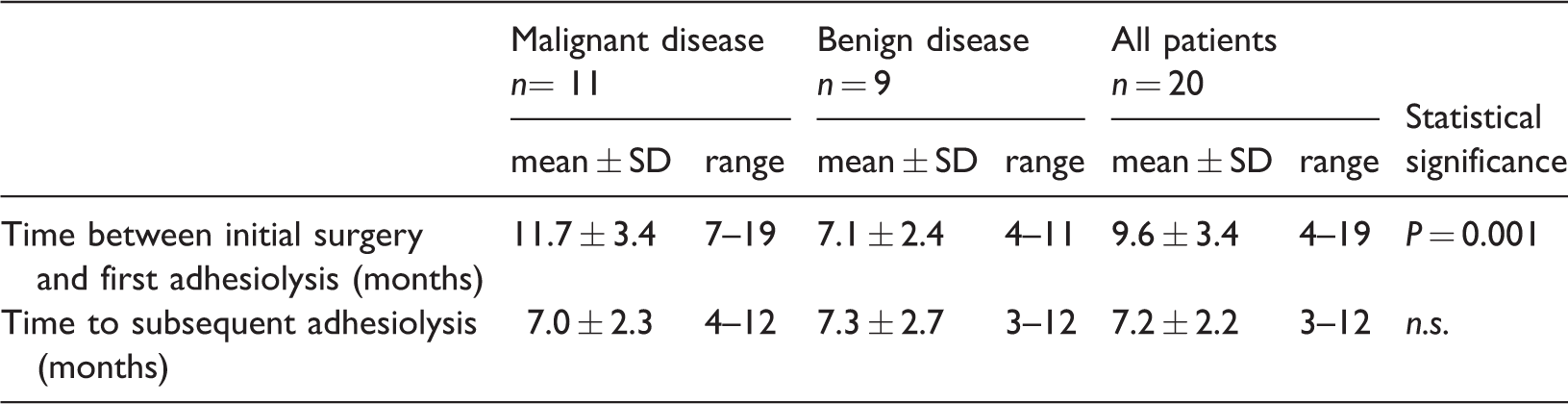
The time interval between initial surgery and first adhesiolysis surgery was significantly longer for the sub-group with malignant abdominal disease compared with the sub-group who had benign disease (11.7 ± 3.4 and 7.1 ± 2.4 months, respectively) (Table 2). The time to subsequent adhesiolysis surgery was similar in both groups (7.0 ± 2.3 and 7.3 ± 2.7 months, respectively).
Time intervals between adhesiolysis surgeries following surgical treatment for either a non-malignant or malignant pathology
During the postoperative period following adhesiolysis surgery with methylene blue, abdominal drainage was maintained for 48 h. On the first postoperative day, the drainage volume for all patients was approximately 200 ± 55 ml per day (range 100–350 ml). By the second day, average drainage volume had decreased to <100 ml which permitted removal of the drainage tubes.
Patients were monitored for 28.5 ± 11.1 months (range 9–57 months) following adhesiolysis surgery with methylene blue. Four (20%) patients reported chronic abdominal pain that was managed by minimal analgesic therapy (three of these patients had reported pain in the pre-adhesiolysis period. For three (15%) other patients, surgical treatment was required for pathologies independent of the initial disease and abdominal adhesions; in these cases, patients showed low grade adhesions with a limited extent in the peritoneal cavity (Bhatia grade II). 15
For all patients, the time between initial surgery and first adhesiolysis surgery was longer than the time to subsequent adhesiolysis surgery (9.6 ± 3.4 and 7.2 ± 2.2 months, respectively), but the difference was not statistically significant (Table 2). However, analysis showed that these time intervals were statistically significantly (P=0.002) shorter than the symptom-free, follow- up period following adhesiolysis surgery with methylene blue (i.e., 28.5 ± 11.1 months)
No significant differences were observed in oxygen saturation or time interval until first flatus when values from previous adhesiolysis surgeries and adhesiolysis surgery with methylene blue were compared (Table 3). However, the level of post-operative pain and supplementary analgesic use was significantly elevated when previous adhesiolysis surgeries were compared with the adhesiolysis surgery with methylene blue (Table 3).
Postoperative parameters from patients undergoing adhesiolysis surgery

scale ranged 1 (no pain) to 5 (unbearable pain) 16
Discussion
Complications caused by the formation of postoperative peritoneal adhesions, whether following open or laparoscopic procedures, are of great importance not only because of their high incidence (50-100% of cases) but also because of the high rate of their recurrence (85-93% of cases).1–5,9–11 Numerous studies have investigated various methods or strategies to minimize the risk of peritoneal adhesion formation; these studies have included optimization of surgical procedures and use of adhesion-reducing adjuvants.12,13,17–21 Several substances that may affect the pathogenesis of the peritoneal adhesions have been investigated, with HA-CMC and icodextrin being the most extensively studied, but as yet there is no consensus on the preferred treatment. 14
The use of methylene blue as an anti-adhesive agent has been investigated in several experimental models 20–25 and clinical studies. 26 Its mechanism of action was thought be via the non-selective inhibitory effect of nitric oxide (NO)-synthetase,27,28 which reduces vasodilatation, capillary permeability, angiogenesis and collagen synthesis.29,30 However, other NO-synthetase inhibitors, such as NG-nitro-L-arginine methyl ester, do not have the same anti-adhesive effect.29,30 Moreover, NO donors, such as L-arginine and spermine NONOate, have also been shown to reduce adhesion formation.31–33 Furthermore, its mechanism of action cannot be related to a reduction in free radicals since other antioxidant substances (e.g., allopurinol, super oxide dismutase, vitamin E) are not as effective as methylene blue.34,35 Other studies suggest that methylene blue reduces intraabdominal adhesion formation by enhancing peritoneal fibrinolytic activity. 23 Notably, its anti-adhesive effect was not observable within the first 24 hours but was significant after seven days. 22 In summary, the prevention of peritoneal adhesion formation by methylene blue is probably a complex process involving acute inflammatory reaction, intermediate proliferative phase of fibrinolysis and eventually collagen formation and angiogenesis. 23
By contrast with previous studies that have evaluated the short-term (8-12 weeks) anti-adhesive proprieties of methylene blue, 26 our study cannot confirm that the agent prevents peritoneal adhesion formation. However, it did show that methylene blue was not associated with adhesion complications in a majority of patients for approximately 28.5 months.This period was significantly greater than previous recurrence periods when methylene blue was not used. The increase in postoperative pain and use of analgesics after surgery with methylene blue may be explained by the irritant effect of the agent on nerve endings in the peritoneal serosa.36,37
The appearance of postoperative adhesions after initial surgery occurred significantly earlier in patients with benign pathologies compared with those with malignant disease. We suggest that this difference may have been due to a slower adhesion maturation process as a result of local metabolic changes caused by adjuvant anti-cancer treatment. The time between subsequent adhesiolysis surgeries was similar in malignant or benign disease groups. We believe this may be explained by a similarity in the adhesion formation process in all patients who were no longer suffering from septic peritoneal disease or undergoing oncological treatment.
The study had several limitations including its retrospective design, small sample size, lack of control group and possible selection bias. Nevertheless, the study highlights the need for further research on the anti-adhesive properties of methylene blue in randomized controlled trials involving large numbers of patients.
Footnotes
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.