
Abstract
Objective
To investigate the effect of the coronavirus disease (COVID-19) pandemic on lifestyle behaviour and clinical data in a population who underwent an annual health check-up in Tokyo, Japan.
Methods
A self-report questionnaire was completed regarding changes in their physical activities, diet, alcohol intake, smoking and mental stress. For those recommended to undergo further examination or treatment, their intention to do so was also questioned. The clinical results of the check-ups across three different periods (before and during the pandemic and survey period) were statistically compared.
Results
During the survey period, 838 examinees responded. While physical activities decreased due to teleworking, changes in food intake and dietary patterns were varied. Furthermore, changes in mental stress were also diverse. As for the intention to undergo further clinical examination or treatment, 23.5% answered that they thought they would wait until the government lifted the state of emergency or the pandemic subsided. Compared with before the pandemic, diastolic blood pressure, liver function, kidney function and bone density tended to deteriorate.
Conclusions
The COVID-19 pandemic affected the lifestyle of the current study population. To prepare for future outbreaks, real-world information should be collected and shared so that effective measures for health promotion can be developed.
Introduction
The coronavirus disease (COVID-19) is a novel infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus. It was first identified by the World Health Organization (WHO) in December 2019, following an outbreak in Wuhan, China. 1 Subsequently, COVID-19 was declared a public health emergency on 30 January 2020 and further classed as a pandemic in March 2020. As of 26 March 2023, there have been over 760 million confirmed cases of COVID-19 and 6.8 million deaths. 2 To prevent the transmission of COVID-19, many countries took various measures, such as a placing their populations into a lockdown situation. Due to these measures, the lives of people, including their dietary habits, physical activities and mental health, were enormously affected.3–31
From early March 2020, the Japanese government encouraged companies to introduce remote-working systems. Furthermore, the Prime Minister declared a state of emergency for Tokyo, Osaka and other major metropolitan areas on 7 April 2020, which was subsequently extended nationwide on 16 April 2020. Based on the declaration, citizens were instructed to stay at home, refrain from nonessential outings and to limit their use of public transportation and facilities. The first declaration was lifted on 25 May 2020. However, due to the continuation of the pandemic, the Tokyo Metropolitan Government had to repeatedly declare states of emergency, which were related to the timing of the increase in new COVID-19 cases (between April and May 2020, January and March 2021, April and June 2021, July and September 2021). Although the Japanese government did not implement a lockdown, the lifestyle of the Japanese people was strongly impacted and changed due to these declarations.21,32
In Japan, according to the Industrial Safety and Health Act, 33 employers are legally required to have employees undergo an annual health check-up to promote their healthcare awareness, detect abnormalities at an early stage, which can lead to early treatment and prevent working in unhealthy conditions.34,35 Items of the health check-up, procedures and frequency vary depending on individual cases and some employers offer employees comprehensive health check-ups called ‘Ningen-Dock’. These include anthropometric parameters, biochemical tests and some imaging studies together with a doctor’s consultation and lifestyle education, which may prevent the progression of lifestyle-related diseases by reducing modifiable risk factors.36–38
The Akasaka Sanno Medical Centre (ASMC) provides comprehensive health check-ups (hereafter, check-ups) for both workers and non-employment applicants concerned regarding their health. To determine the influence of the COVID-19 pandemic on Japanese workers, this current study conducted a questionnaire survey of the examinees of the check-ups at the ASMC. The answers provided by the examinees to the questionnaire and the results of the check-ups were analysed.
Participants and methods
Study design and population
This current retrospective study undertook a survey of examinees who underwent a check-up at the ASMC, Tokyo, Japan between 1 January 2022 and 30 April 2022. A questionnaire and a brief description of the study and its aim were sent to the individual examinees beforehand. Information regarding the study aim was also posted at the ASMC. Additionally, an opt-out method was provided for examinees who did not wish to participate. The questionnaires were signed by each examinee and their anonymity and confidentiality were guaranteed when the results were analysed. The questionnaire included 11 questions divided into seven categories as follows: commuting, exercise, dietary habit, alcohol consumption, smoking, mental stress and hospital visit (see supplementary materials, Figure 1). No specific inclusion/exclusion in the criteria was pre-determined.
This study was conducted with the approval of the medical Ethics Review Board of Sanno Hospital and ASMC (approval number: 21-S-19). Written informed consent was deemed obtained when the participants submitted/responded to the questionnaire. This study’s report conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 39
Questionnaire items
The check-up items included age, sex, anthropometric data, blood pressure, pulse rate, electrocardiogram, blood and urine tests, faecal occult blood test, ophthalmological examinations, audiometry tests, gastric endoscopy, abdominal ultrasound examination, bone density (calcaneal bone densitometry via ultrasound) and examinations for female-related diseases, such as breast cancer and gynopathy. Among the participants, some had undergone their previous check-ups before (before 31 March 2020) and during the COVID-19 pandemic (between 1 April 2020 and 31 December 2021). The study analysed the data from these time periods.
Statistical analyses
All statistical analyses were performed using the SAS statistical package, version 9.4 (SAS Institute Inc., Cary, NC, USA). The examinees were divided into three groups based on the timing of their check-ups (before and during the COVID-19 pandemic and during the survey period). For variables of the characteristics, summary statistics were constructed using mean ± SD, frequency distributions or proportions. According to the variable type, two-way analysis of variance and generalized linear model analysis were used to determine the significance of the differences between the three groups. Welch’s t-test or Fisher’s exact test was used for comparison between males and females. A P-value <0.05 was considered statistically significant.
Results
During the survey period, 2253 individuals underwent check-ups at the ASMC. Among them, 841 examinees participated in the study (participation rate, 37.3%). The examinees’ check-up results organized by timing (before and during the COVID-19 pandemic and during the survey period) are shown in Table 1. Diastolic blood pressure (DBP), total protein (TP), albumin (Alb), creatinine (Cr), estimated glomerular filtration rate (eGFR), estimated GFR by cystatin C (eGFRcys), aspartate aminotransferase (AST), alanine aminotransferase (ALT), erythrocyte sedimentation rate (ESR), white blood cell (WBC), red blood cell (RBC), haematocrit (Hct), platelet (Plt) and bone density values were significantly different between before the pandemic (T0), during the pandemic (T1) and survey period (T2) (P < 0.05 for all comparisons). Among these characteristics, DBP, AST, ALT, ESR, WBC, RBC, Hct and Plt increased from T0 to T1 to T2. TP and albumin were the same at T0 and T1; however, they increased at T2. eGFR decreased from T0 to T1; however, it increased from T1 to T2. Cr continued to increase while eGFRcys, which is less dependent than eGFR upon the body composition, consistently decreased all through T0 to T1 to T2. These results demonstrated that kidney function deteriorated all through these periods. Bone density also decreased from T0 to T1 to T2.
Demographic and clinical characteristics before/during the coronavirus disease (COVID-19) pandemic and during the survey period in Japanese workers (n = 841) that underwent routine health check-ups at the Akasaka Sanno Medical Centre, Tokyo, Japan.
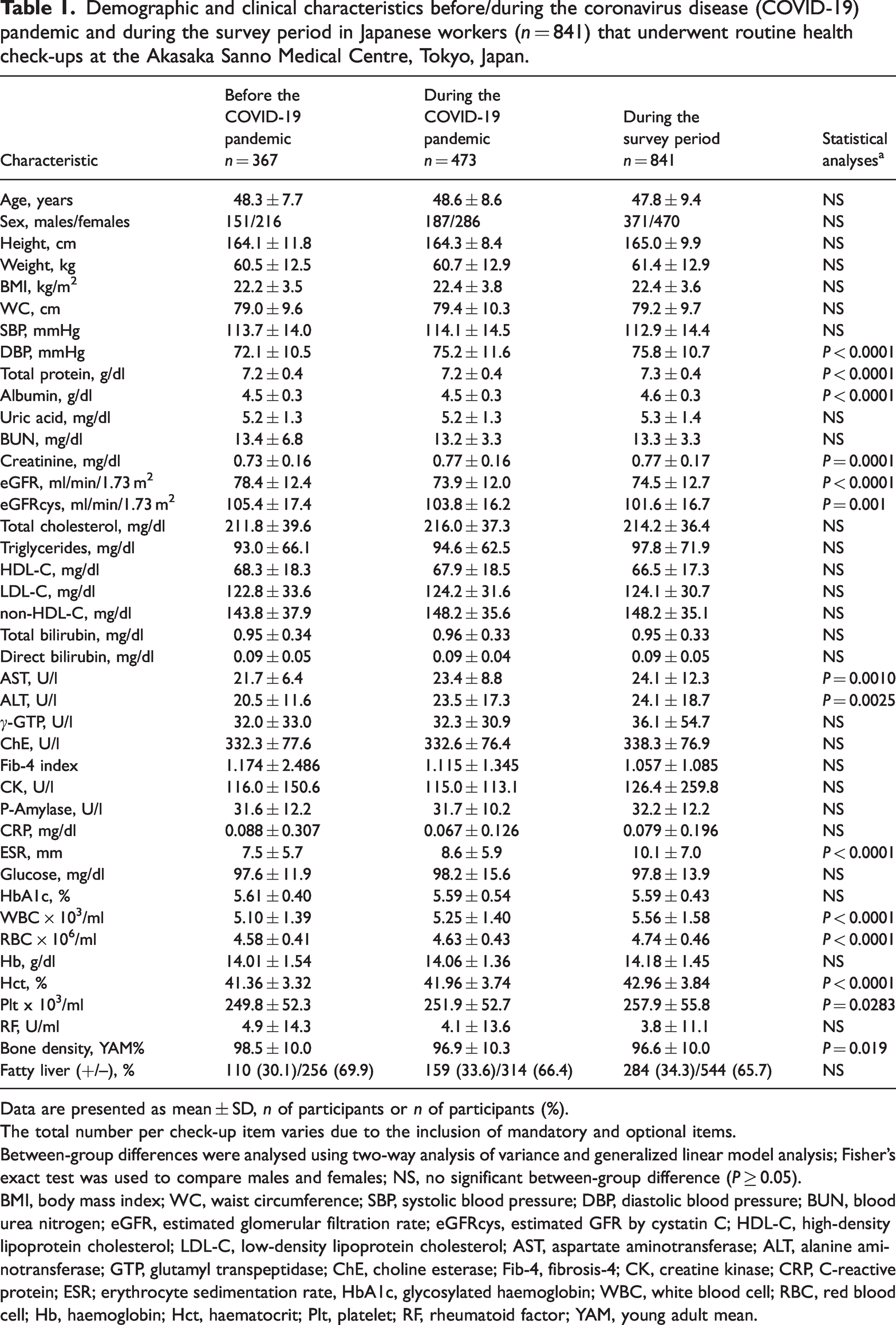
Data are presented as mean ± SD, n of participants or n of participants (%).
The total number per check-up item varies due to the inclusion of mandatory and optional items.
Between-group differences were analysed using two-way analysis of variance and generalized linear model analysis; Fisher’s exact test was used to compare males and females; NS, no significant between-group difference (P ≥ 0.05).
BMI, body mass index; WC, waist circumference; SBP, systolic blood pressure; DBP, diastolic blood pressure; BUN, blood urea nitrogen; eGFR, estimated glomerular filtration rate; eGFRcys, estimated GFR by cystatin C; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; AST, aspartate aminotransferase; ALT, alanine aminotransferase; GTP, glutamyl transpeptidase; ChE, choline esterase; Fib-4, fibrosis-4; CK, creatine kinase; CRP, C-reactive protein; ESR; erythrocyte sedimentation rate, HbA1c, glycosylated haemoglobin; WBC, white blood cell; RBC, red blood cell; Hb, haemoglobin; Hct, haematocrit; Plt, platelet; RF, rheumatoid factor; YAM, young adult mean.
Among the examinees, 838 (368 men and 470 women) answered the questionnaire (hereafter, respondents). Three of the 841 examinees chose not to complete the questionnaire although they had consented to have their data included in the analyses. The results for responses to question 1, excluding 102 respondents (eight men and 94 women) who responded with ‘not applicable’, are summarized in Table 2. As shown in Table 2a, compared with before the pandemic, the commuting frequency during the pandemic was reduced, with statistical significance in both men and women (P < 0.0001 for all comparisons). Before the pandemic, men commuted significantly more frequently than women (P < 0.0001) (Table 2b). However, this sex difference was not observed during the pandemic and the survey periods.
Results of the questionnaire survey undertaken in Japanese workers (n = 838) that underwent routine health check-ups at the Akasaka Sanno Medical Centre, Tokyo, Japan: question 1 – How many days per week did you commute to your place of work?
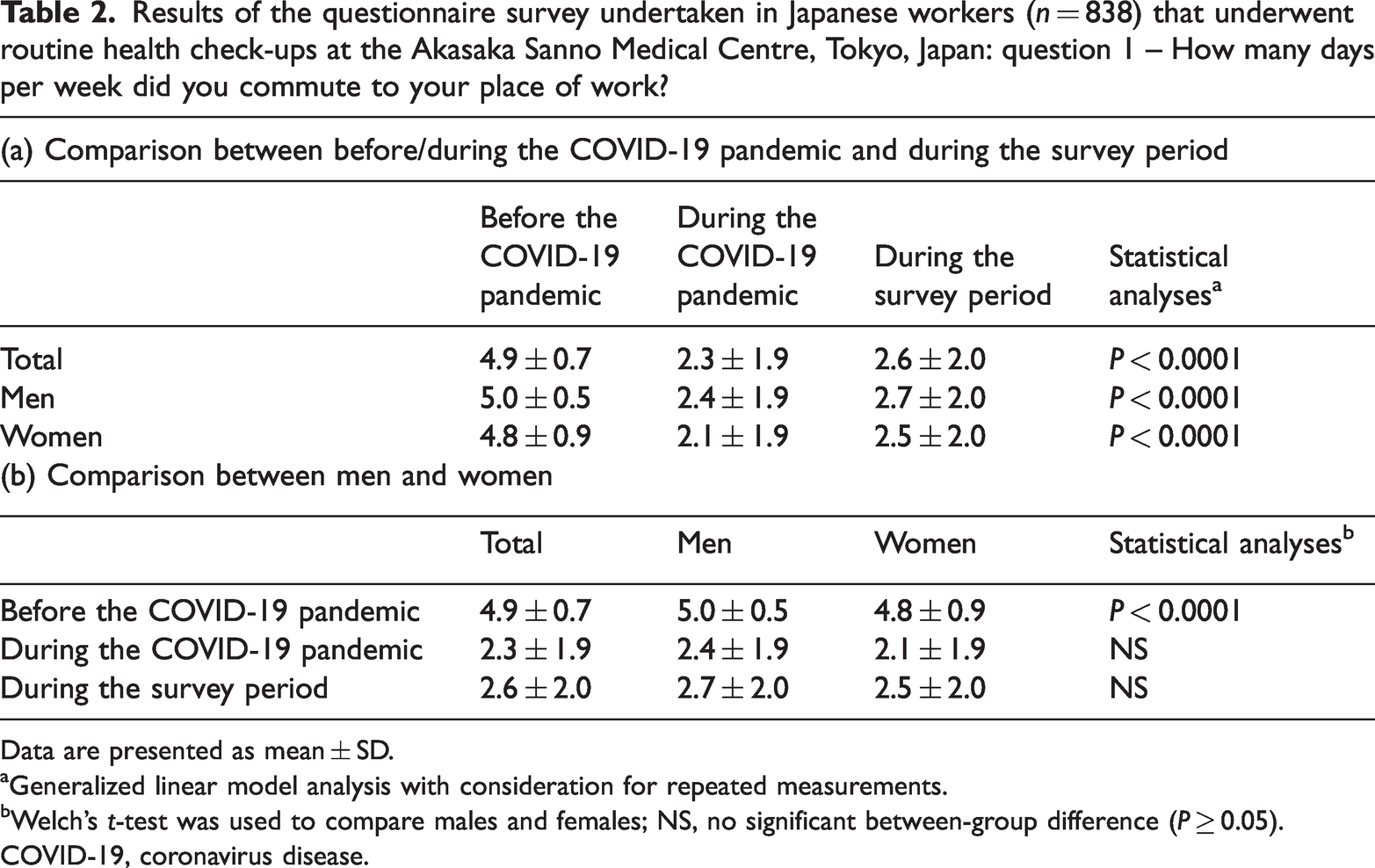
Data are presented as mean ± SD.
Generalized linear model analysis with consideration for repeated measurements.
Welch’s t-test was used to compare males and females; NS, no significant between-group difference (P ≥ 0.05).
COVID-19, coronavirus disease.
The answers to question 2 are summarized in Table 3a. In both men and women, the most selected answer with regard to the change in their level of physical activities (PA) was ‘Decreased’, followed by ‘No change’. Compared with women, significantly more men answered ‘Increased’ (P = 0.0435). Respondents who answered that their level of PA increased during the pandemic were asked to choose the reasons. Their choices are summarized in Table 3b. In both men and women, the most selected reason was ‘opportunity to exercise increased due to more free time’. Furthermore, significantly more men than women selected this reason (P = 0.0048). Representative free comments for ‘others’ included an increase in additional physical activities, such as ‘housework increased’ and ‘more time to play with children’. Respondents who answered that their level of PA decreased during the pandemic were also asked to choose the reasons. Their choices are summarized in Table 3c. In both men and women, the most selected reason was ‘commuting shifted to teleworking’. Furthermore, significantly more men than women selected this reason (P = 0.0003). The second most selected reason was ‘staying indoors’, which was selected significantly more frequently by women than men (P = 0.0443). Representative free comments for ‘others’ included ‘reduced time and/or opportunity for hobby due to closure of facilities or cancellation of lessons’, ‘for going out, I tried to use my own car rather than using the public transportation’, and ‘I had less time to do exercise because my family stays at home all the time’.
Results of the questionnaire survey undertaken in Japanese workers (n = 838) that underwent routine health check-ups at the Akasaka Sanno Medical Centre, Tokyo, Japan: question 2 – How did the levels of physical activities change from before to during the coronavirus disease (COVID-19) pandemic?

Data are presented as n of participants (%).
Fisher’s exact test was used to compare males and females; NS, no significant between-group difference (P ≥ 0.05).
Excluded responses: respondents had to choose one answer; however, they chose multiple answers.
The answers to question 3A are summarized in Table 4a. While more than 40% of the respondents answered that their meal amount had not changed during the pandemic, 144 of 470 (30.6%) women and 91 of 368 (24.7%) men answered that their diet had increased. Respondents who answered that their total amount of food intake had increased were asked to choose the reasons. Their choices are summarized in Table 4b. In both men and women, the most selected reason was ‘intake of sweets or snacks increased’. This reason was selected by significantly more women than men (P = 0.0013). Representative free comments for ‘others’ included ‘I ate more than before to deal with stress’ and ‘the size of dinner increased at home due to teleworking’. Respondents who answered that their total amount of food intake decreased were also asked to choose the reasons. Their choices are summarized in Table 4c. In both men and women, the most selected reason was ‘frequency of dining out or drinking party decreased’. Representative free comments for ‘others’ included ‘My physical activities reduced and I lost my appetite as a result of teleworking’, ‘Because I gained weight, now I am trying to lose weight’, ‘Fewer opportunities to have snacks while working’, ‘Because the staff cafeteria was closed’ and ‘Because my workload increased, I could not have enough time to have meals’. The answers for question 3B are summarized in Table 5. The most selected answer by men was ‘became regular’. While 159 of 368 (43.2%) men selected this answer, only 134 of 470 (28.5%) of women selected it (P < 0.0001). Compared with men, significantly more women selected ‘no change’ (P < 0.0001). The answers for question 3C are summarized in Table 6. In both men and women, more than 72% answered that their frequency of dining out decreased. The answers for question 3D are summarized in Table 7. In both men and women, approximately 48% (175 of 368 men and 231 of 470 women) answered that their frequency of delivered meals/takeout/meals purchased at convenience store did not change. Furthermore, 35.0% (293 of 838 participants) answered that the frequency increased.
Results of the questionnaire survey undertaken in Japanese workers (n = 838) that underwent routine health check-ups at the Akasaka Sanno Medical Centre, Tokyo, Japan: question 3A – How did your total amount of food intake change from before to during the coronavirus disease (COVID-19) pandemic?

Data are presented as n of participants (%).
Fisher’s exact test was used to compare males and females; NS, no significant between-group difference (P ≥ 0.05).
Results of the questionnaire survey undertaken in Japanese workers (n = 838) that underwent routine health check-ups at the Akasaka Sanno Medical Centre, Tokyo, Japan: question 3B – How did your meal schedule change from before to during the coronavirus disease (COVID-19) pandemic?
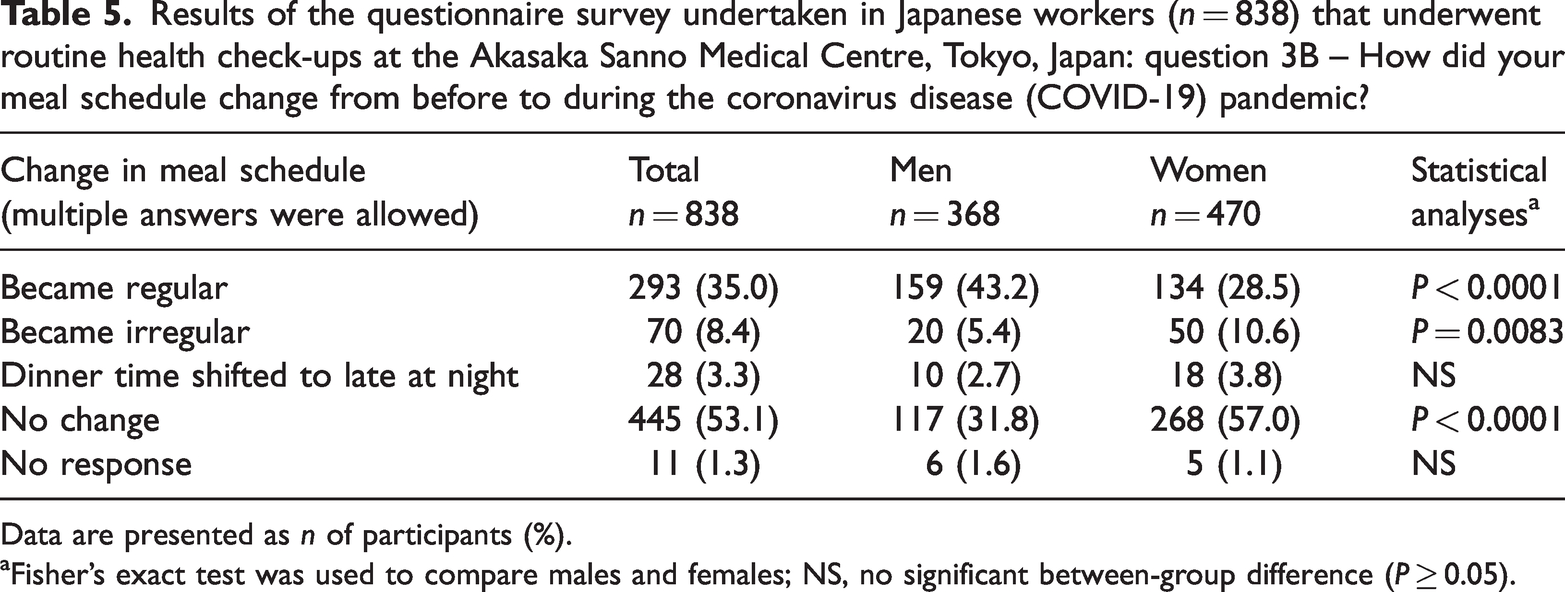
Data are presented as n of participants (%).
Fisher’s exact test was used to compare males and females; NS, no significant between-group difference (P ≥ 0.05).
Results of the questionnaire survey undertaken in Japanese workers (n = 838) that underwent routine health check-ups at the Akasaka Sanno Medical Centre, Tokyo, Japan: question 3C – How did your frequency of dining out change from before to during the coronavirus disease (COVID-19) pandemic?

Data are presented as n of participants (%).
No significant between-group differences (P ≥ 0.05).
Results of the questionnaire survey undertaken in Japanese workers (n = 838) that underwent routine health check-ups at the Akasaka Sanno Medical Centre, Tokyo, Japan: question 3D – How did your frequency of delivered meals/takeout/meals purchased at convenience store change from before to during the coronavirus disease (COVID-19) pandemic?
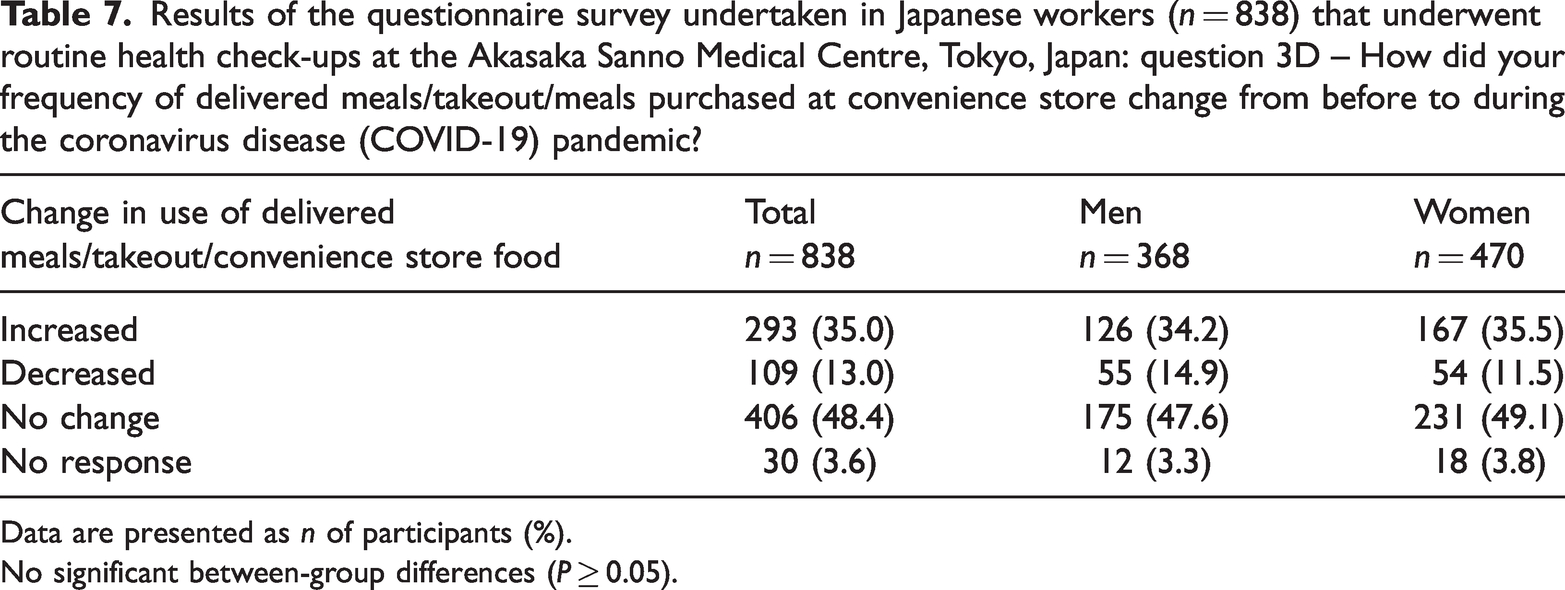
Data are presented as n of participants (%).
No significant between-group differences (P ≥ 0.05).
The answers to question 4 are summarized in Table 8a. The most selected answer by men was ‘decreased’. Regarding sex differences, significantly more men than women selected this answer (P = 0.0028). Respondents who answered that their amount of alcohol intake increased were asked to choose the reasons. The results are summarized in Table 8b. The most selected reason for both men and women was ‘amount and frequency of drinking at home increased’. Respondents who answered that their amount of alcohol intake decreased were also asked to choose the reasons. The results are summarized in Table 8c. In both men and women, the most selected reason was ‘frequency of dining out or drinking party decreased or cancelled’. Representative free comments for ‘others’ included ‘I do not feel like drinking anymore’, ‘I tried to reduce alcohol intake’ and ‘It is troublesome to go outside to buy alcohol’.
Results of the questionnaire survey undertaken in Japanese workers (n = 838) that underwent routine health check-ups at the Akasaka Sanno Medical Centre, Tokyo, Japan: question 4 – How did the amount of alcohol intake change from before to during the coronavirus disease (COVID-19) pandemic?
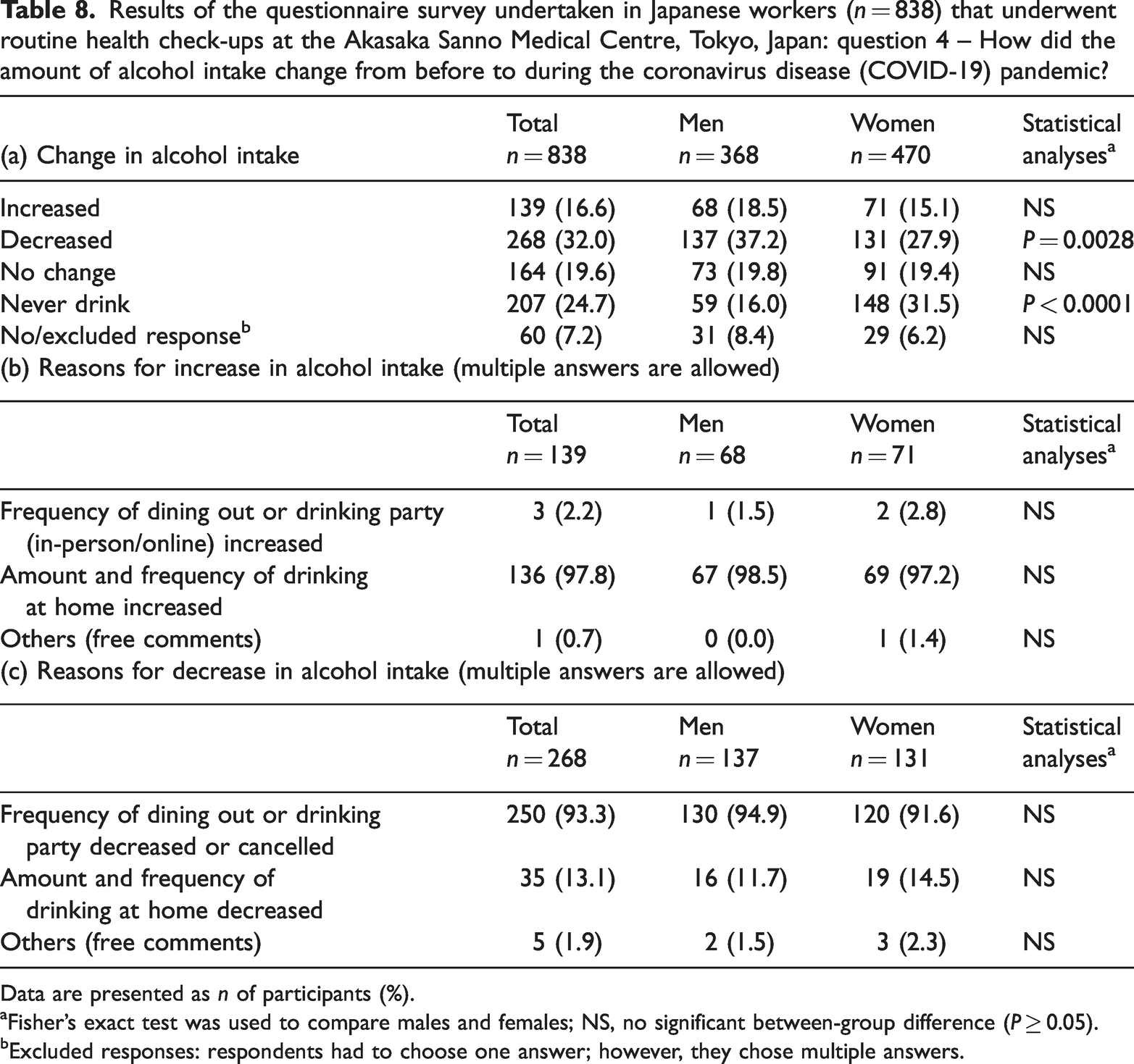
Data are presented as n of participants (%).
Fisher’s exact test was used to compare males and females; NS, no significant between-group difference (P ≥ 0.05).
Excluded responses: respondents had to choose one answer; however, they chose multiple answers.
The answers to question 5 are summarized in Table 9. In both men and women, the most selected answer was ‘non-smoker’. Among the smokers, the most selected answer both by men and women was ‘no change’.
Results of the questionnaire survey undertaken in Japanese workers (n = 838) that underwent routine health check-ups at the Akasaka Sanno Medical Centre, Tokyo, Japan: question 5 – How did the amount of smoking change from before to during the coronavirus disease (COVID-19) pandemic?

Data are presented as n of participants (%).
Fisher’s exact test was used to compare males and females; NS, no significant between-group difference (P ≥ 0.05).
The answers to question 6A are summarized in Table 10a. In both men and women, the most selected answer was ‘increased’ and significantly more women selected it than men (P = 0.0009). The second most selected answer in both men and women was ‘No change’. Compared with women, significantly more men selected it (P = 0.0037). Respondents who answered that their mental stress increased or decreased were asked to choose the main reasons among nine choices (question 6B). Although question 6B asked respondents to choose one main reason (single response), there were instances where respondents choose multiple reasons. These reasons were included as there could be instances where respondents felt two or more reasons could be equally valid. The reasons for an increase in mental stress are summarized in Table 10b. In both men and women, the most selected answer was ‘staying indoors’. The second most selected answer by men was ‘teleworking’ and significantly more men than women selected this reason (P = 0.0007). Representative free comments for ‘others’ included various comments, such as ‘I am anxious and worried about being infected’, ‘Due to teleworking, my husband is constantly at home’, ‘Because of teleworking and closure of schools, my family stays home and my household chores increased’, ‘Fewer opportunities to meet people’, ‘I feel lonely’, ‘Lack of communication with colleagues or clients’, ‘My work load increased’ and ‘Infection prevention measures bother me’. The reasons for mental stress reduction are summarized in Table 10c. In both men and women, the most selected answer was ‘teleworking’. Representative free comments for ‘others’ included ‘Frequency of commuting decreased’, ‘I could have more time to spend with my family’, ‘I have less stress regarding interpersonal relationship’, ‘I could have more free time’ and ‘I could enjoy my hobby’.
Results of the questionnaire survey undertaken in Japanese workers (n = 838) that underwent routine health check-ups at the Akasaka Sanno Medical Centre, Tokyo, Japan: question 6A – How did your mental stress change from before to during the coronavirus disease (COVID-19) pandemic and question 6B – What is the main reason for the answer above?

Data are presented as n of participants (%).
Multiple responses for this (single-response) question were included in the results.
Fisher’s exact test was used to compare males and females; NS, no significant between-group difference (P ≥ 0.05).
The answers to question 7 are summarized in Table 11. In both men and women, the most selected answer was ‘I consulted or intended to consult a hospital regardless of the COVID-19 pandemic’. Representative free comments for ‘others’ included ‘No follow-up needed’, ‘I will go to a hospital after I receive a vaccination’, ‘I will consult my family doctor’ and ‘I have no time to go to a hospital’.
Results of the questionnaire survey undertaken in Japanese workers (n = 838) that underwent routine health check-ups at the Akasaka Sanno Medical Centre, Tokyo, Japan: question 7 – Applicable to those recommended for further examination or treatment for health issues after completing the comprehensive health check-ups underwent before/during the COVID-19 pandemic, when did you consult a hospital or intend to consult?

Data are presented as n of participants (%).
Fisher’s exact test was used to compare males and females; NS, no significant between-group difference (P ≥ 0.05).
Discussion
The COVID-19 pandemic affected people’s lives and individual’s health issues. Based on the results (Table 1), the pandemic and associated circumstances negatively affected blood pressure, liver function, kidney function and bone density. Although the possibility that these changes were due to the natural aging of the participants cannot be ruled out, the decline over a short period of time suggests that they might have resulted from the impact of the COVID-19 pandemic.
In terms of PA levels, although it may not be clearly perceived by workers, commuting or being out of the office for sales provides a good opportunity to increase PA levels. However, due to the lockdown in many countries and the strong promotion of teleworking in Japan during the COVID-19 pandemic, workers became physically inactive with an increased sedentary behaviour. Furthermore, they tended to suffer weight gain, musculoskeletal pain and symptoms of eye problems.21,23–27 In this current study, the answers to question 2 revealed that 80.5% of men and 66.2% of women considered that their levels of PA had decreased mainly due to teleworking. In addition to the disturbance of dietary habits, lack of PA and longer sitting times are well-known risk factors for non-communicable diseases (NCDs), such as diabetes mellitus and cardiovascular disease. Thus, the COVID-19 pandemic surely increased the risk of onset or aggravation of these NCDs.18,22,40–50 In addition, due to the pandemic, a reduction in the total PA time in older adults was reported and raised concerns of a higher incidence of disability in the future. 51 As a result of the pandemic, teleworking in Japan was drastically promoted and will likely continue into the foreseeable future. Therefore, governments, organizations and health professionals should develop effective and feasible methods of promoting exercise, especially for a population that will almost certainly engage in teleworking.
With regard to diet, a study examined the impact of the COVID-19 pandemic on diet and showed population-wide shifts in dietary interests in 18 countries in 2020. 3 Furthermore, it demonstrated that the largest increase occurred with calorie-dense carbohydrate-based foods, such as pastries, breads and pies. 3 Such shifts represented a trend toward having a more unhealthy diet and could lead to obesity especially when PA was also reduced. 3 Interruption of working patterns, stockpiling food due to the shopping restrictions and boredom due to confinement at home were all associated with a greater energy intake.4,52 In addition, stress led people to over eat, so-called ‘food craving’, favouring comfort foods, usually rich in sugar and/or fat (snacks and sweets).4,53–57 Although this current study did not ask for specific details of the participants’ dietary content, considering that 28.0% answered that their amount of food increased, and of these, 73.6% stated that their intake of sweets or snacks increased, it is possible to speculate that they had an unhealthy diet during the COVID-19 pandemic.
Irregular meal timing was associated with lower PA levels and higher productivity loss through greater problems with sleep and mental health;58–60 and metabolic abnormalities, such as diabetes mellitus, obesity, hypertension and hypercholesterolaemia.58,60 In addition, previous epidemiological findings suggested a potential detrimental effect of late meals on cardiometabolic health. 61 The results of question 3B showed that meal timing in men tended to become regular (43.2%) rather than irregular (5.4%). Although the reasons for this trend were not asked for, in combination with the results of question 3C, it is possible to speculate that the lower frequency of dining out or business dinners may have contributed to this result. More than half of the female respondents (57.0%) answered that their meal timing did not change. This may be a result of them having fewer opportunities to attend business dinners than men even before the COVID-19 pandemic. It can be argued that the impact of the pandemic on meal timing among women was smaller than that among men.
In terms of alcohol consumption, in order to investigate changes in drinking habits among adults during the COVID-19 pandemic, the International Alliance for Responsible Drinking (IARD) conducted an online survey in November 2020 with 14 representative countries, which included Japan. 62 According to the results, the percentage of drinkers whose alcohol consumption was less or who had quit drinking entirely was 21% overall, with 14% of that figure being in Japan. 62 Those whose alcohol consumption did not change accounted for 42% of the total group, of which 48% were in Japan. 62 Those whose alcohol consumption increased or who started to drink were 9% of the total group, of which 12% were in Japan. 62 Although the individual percentages observed in the current survey for question 4 were different from that of the IARD survey, these current results indicated a similar tendency as more people reduced their alcohol consumption during the COVID-19 pandemic. The main reason for this decrease was a decrease in the frequency of dining out or drinking parties. A cross-sectional comparative study of nine European countries also showed reduced alcohol intake secondary to home confinement and restrictions on sales. 63 In contrast, other studies reported increased alcohol consumption during lockdown compared with prior to lockdown.64,65 Factors associated with increased alcohol use included psychological distress related to COVID-19 (job loss, changes in sleep, higher anxiety and depression, loneliness and lower social connectedness), increased availability of free time and misinformation regarding alcohol.64,66
With regard to smoking habits, the prevalence of smoking in Japan has consistently decreased from 2001 to 2019; however, estimates for 2020 indicated flattening and increasing trends among men (29.0%) and women (8.8%), respectively. 67 Based on the answers to question 5, approximately 20.0% of men and 8.0% of women were smokers. Therefore, the prevalence of smoking among the current participants, both men and women, was lower than the estimated 2020 results. 67 Since the examinees who underwent check-ups at the ASMC were relatively young (the mean age was 47.8 years) and worked in large companies, they may have a high literacy rate and be concerned regarding their health. This may offer a partial explanation to the divergence in numbers. Patients with COVID-19 who smoked tended to suffer with greater severity and had a greater risk of mortality.68–73 Globally, many current smokers understand this risk and want to reduce their smoking frequency or quit smoking. However, previous studies reported that more current smokers had increased their smoking during the COVID-19 pandemic.74–79 The results of this current study complement these previous findings.67–79 Possible explanations for an increase in smoking frequency rather than a decrease included responding to pandemic-induced stress by increasing smoking frequency, 75 no restrictions against smoking while teleworking 74 or being bored due to self-isolation.77,80
In terms of mental health, the COVID-19 pandemic caused a negative effect on people’s mental health and emotions, such as depression, post-traumatic stress disorder, substance use disorder, confusion and anger.81–83 Stress-inducing factors included lengthier quarantine, fear of infection, frustration, boredom, diminishing supplies, unreliable information, monetary worries and social isolation. 83 According to a meta-analysis of longitudinal cohort studies that compared mental health prior to and during the pandemic in 2020, the overall increase in mental health symptoms was most pronounced during the first 2 months after the WHO pandemic declaration in March 2020. 84 A longitudinal study that analysed the influence of repeated mild lockdowns in Japan, during two emergency declarations, in May 2020 and February 2021, suggested that repeated mild lockdowns exacerbated social isolation and had cumulative negative effects on loneliness. 85 This current study simply asked about the overall fluctuation of levels of mental stress; however, questions regarding detailed mental symptoms or peak timing of mental stress were not included. Compared with men, a higher percentage of women answered that their mental stress had increased, which suggested that the impact of the COVID-19 pandemic on mental stress varied according to sex and that women tended to have a heavier burden.
With regard to teleworking, during the pandemic, to avoid infection and the transmission of COVID-19, the Japanese government encouraged people to stay home and promoted teleworking. According to a survey conducted by the Cabinet Office of Japan, 86 the teleworking efficacy rate before the pandemic in December 2019 was 10.3% nationwide and 17.8% in Tokyo. During the first state of emergency in May 2020, the efficacy rate increased to 27.7% nationwide and 48.4% in Tokyo. 86 As of June 2022, nationwide and Tokyo had a rate of 30.6% and 50.6%, respectively. 86 Teleworking has advantages, such as avoiding rush-hour traffic congestion, being an effective tool for achieving a good work-life balance,24,87 offering greater autonomy and lowering conflict between work and family;24,88 and thereby, producing favourable effects on job satisfaction and performance.24,25,88 In contrast, there are disadvantages such as occupational isolation that might result in poor job performance24,89 and encroachment into what was formerly home and family time by lengthening working hours.24,90 Teleworking may also increase work-to-family conflict by triggering the redistribution of household chores and sex inequality (especially in a male-orientated society). 24 Interestingly, according to this current study, ‘teleworking’ ranked high as both a reason for the increase and decrease in stress during the pandemic. Whether people consider ‘teleworking’ favourable or unfavourable may depend upon several factors, such as occupation, working conditions at the working place or home, marital status and individual personality.
In terms of accessing hospital-based care, the COVID-19 pandemic also affected the frequency of medical service usage by patients. Owing to fear of the contagion and also disruption in medical services, accessibility to non-COVID-19 health services was reduced in many countries, including Japan.42,91–98 This decrease in medical service usage was one of the most serious and detrimental impacts caused by the COVID-19 pandemic. 99 A recent population-based parallel cohort study undertaken in England showed an increased risk of mortality in people with diabetes mellitus who did not receive key diabetes care in the previous 2 years. 100 The study concluded that the increased rate of non-COVID-19 related mortality observed between July and October 2021 was associated with reduced completion of routine diabetes care following the onset of the pandemic in 2020. 100 As for the intention to consult a hospital regarding health issues revealed by check-ups in the current study, approximately half of the respondents answered that they would consult regardless of the pandemic, 23.5% answered that they thought they would wait until the government lifted the state of emergency or the pandemic subsided. One of the main purposes of check-ups is the early detection of cancer. Delayed cancer treatment has a significant impact on survival.101,102 Although check-ups detected some abnormalities, if examinees were reluctant or refused to visit the hospital, the prognosis for the disease would be unfavourable. The COVID-19 pandemic dissuaded people from cancer screening or diagnosis for cancer,103–106 which lead to cancer detection at an advanced stage 107 or a substantial increase in the number of avoidable cancer deaths. 108 The future of the COVID-19 pandemic remains unclear. However, measures to promote annual health check-ups and encourage the public to utilize health services are required and should be implemented.
This current study had several limitations. First, the sample size was relatively small and the study was conducted in a single centre in Tokyo, in an urban area close to the governmental district. Therefore, the majority of the examinees were office workers of large corporations or organizations and were relatively young and in the prime of their careers. Hence, a selection bias on socioeconomic status might have influenced the results. In addition, since it was a signed questionnaire survey (not anonymous), participants who returned the questionnaire might have been more cooperative and not so particular regarding the disclosure of personal information. Therefore, the participants could be a unique population with a biased selection. Secondly, the responses to the questionnaire were not evaluated quantitatively; however, the study employed a self-reported style. For example, the amount of meal intake was simply classified as ‘increased’, ‘decreased’ or ‘unchanged’ and not actually self-measured nor calculated by a dietician. Therefore, the results were subjective and may be inaccurate. Particularly, amounts of food intake, alcohol intake or smoking amount were known to be underreported due to recall and social desirability biases.109–113 Thirdly, since the survey period, between January 2022 and April 2022, was the timing of a transitional period after the state of emergency was lifted, people were not completely back to the life they had ‘before the COVID-19 pandemic’, changes in lifestyle were indefinable and difficult to assess. If it had been possible to conduct the survey before and during the pandemic (for example, in the middle of the state of emergency), it would have been possible to compare and demonstrate more distinct behavioural changes combined with a full statistical analysis.
In conclusion, based on an extensive comparison of the examination results of the check-ups undertaken ‘before the pandemic’, ‘during the pandemic’ and ‘during the survey period’, blood pressure, liver function, kidney function and bone density all tended to deteriorate. However, interpretation of these results should be done with caution and requires further study with a larger population. Although government measures for the pandemic in Japan have not been as strict as in other countries that implemented lockdowns, the current participants who underwent check-ups revealed the fact that the COVID-19 pandemic had surely affected their lifestyle and well-being. As in other published reports, workers shifted more to teleworking, which eventually led to decreased PA levels. Changes in the amount of food intake varied, with no change to most. Alcohol drinkers tended to decrease their alcohol intake. Most participants were non-smokers. Mental stress tended to increase especially in women, while 35.8% and 14.9% answered ‘no change’ and ‘decreased’, respectively. Approximately half of the participants who were recommended for further medical examinations or treatment had already consulted or intended to consult physicians; however, 23.5% were reluctant to do so until the government lifted the state of emergency or the pandemic subsided. Although, as of March 2023, the number of people infected with COVID-19 has decreased, and the disease seems to be gradually abating, further large-scale studies to reveal the longitudinal impacts of the pandemic are necessary. Using this unprecedented experience and sharing real-world information from studies such as this current study, the government, relevant organizations, medical staff and public health professionals should consider preventive methods to minimize the negative impacts of future pandemics on individuals and society. Future studies should establish desirable health interventions during pandemics and verify their effectiveness and feasibility.
Footnotes
Acknowledgements
The authors gratefully acknowledge Ms Mayumi Kobayashi and the other staff at the ASMC for their support in data collection.
Author contributions
M.K., K.M., S.Y. and S.N. designed the study and participated in all steps of the work. R.F. performed the statistical analyses. M.O. and M.Z. supervised the overall study process. All the authors approved the final version of the manuscript and its submission for publication.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.