
Abstract
Objective
To clarify the clinical characteristics and laparoscopic surgical outcomes of dermoid cysts complicated by spontaneous rupture.
Methods
This was a single-center retrospective observational study of patients with dermoid cysts treated between January 2005 and December 2021.
Results
Among 1205 cases of dermoid cysts, spontaneous rupture occurred in nine and torsion occurred in 83 cases. No obvious triggers for rupture were identified, except for one postpartum case with fundal uterine pressure maneuver. Rupture was identified by computed tomography (CT) in six cases. Patients with ruptured cysts had significantly higher serum C-reactive protein (CRP), cancer antigen 125 (CA125), carbohydrate antigen 19-9 (CA19-9), and squamous cell carcinoma antigen (SCC) levels compared with patients with uncomplicated dermoid cysts or cysts with torsion. Laparoscopic management was possible except for one case with severe adhesion, which required laparotomy. Two patients required prolonged postoperative administration of antibiotics due to refractory chemical peritonitis.
Conclusion
Combined use of CT imaging and elevated levels of CRP, CA125, CA19-9, and SCC may help to differentiate cyst rupture from torsion. Laparoscopic surgery may be a feasible option; however, prompt laparotomic conversion should be considered in cases with difficult adhesiolysis. Refractory chemical peritonitis may occur after successful surgical management.
Keywords
Introduction
Dermoid cysts or mature cystic teratomas, originating from primordial germ cells, 1 account for 10% to 25% of all ovarian tumors.2,3 Dermoid cysts are slow-growing tumors 4 that typically present as an asymptomatic adnexal mass, detected incidentally during routine pelvic ultrasound examination 1 or by the identification of a fat component and/or calcification on pelvic computed tomography (CT).1,2
The major complication of dermoid cysts is torsion, while other less-frequent secondary complications include malignant transformation, infection, and rupture.3,4 Torsion or rupture of dermoid cysts poses a diagnostic and therapeutic challenge and requires timely surgical intervention.4,5 Furthermore, chemical peritonitis caused by leakage of sebaceous material into the peritoneal cavity can cause significant co-morbidity before and even after surgery.5–7 However, the clinical characteristics, imaging findings, and preoperative blood indices and serum tumor markers that can help to differentiate between spontaneous rupture and torsion are not well documented.
Based on accumulated clinical experience, we retrospectively evaluated a series of cases of dermoid cysts with spontaneous rupture, and compared their clinical characteristics with those of dermoid cysts with torsion. Our findings may facilitate the timely diagnosis and treatment of this entity.
Materials and methods
Patient characteristics
This was a retrospective observational review of consecutive cases of surgically confirmed dermoid cysts with spontaneous rupture (Group C) extracted from electronic chart records between January 2005 and December 2021. These patients were compared with the 30 most recent consecutive cases of dermoid cysts with adnexal torsion (Group B) and 30 with uncomplicated dermoid cysts (Group A).
To describe the clinical presentations, patients were divided arbitrarily into three categories with acute, subacute, or chronic clinical manifestations, respectively, based on the duration from symptom onset to surgical management (≤24 hours, 2 days, or ≥3 days, respectively). 8
The reporting of this study conforms to the STROBE guidelines in the EQUATOR Network guidelines (https://www.equator-network.org/). 9 This study was approved by the Institutional Review Board of Gifu Prefectural Tajimi Hospital (IRB number: 2022-18-1). The privacy rights of all subjects were observed. All patients’ details were de-identified in the study. All patients provided signed informed consent for the relevant procedures after an explanation the potential benefits and surgical risks of exploratory laparotomy. Only women who consented to have their clinical information used for research purposes were included in the study cohort.
Preoperative management
All patients underwent ultrasonographic evaluation at their initial visit. Contrast-enhanced CT was also performed to further characterize the adnexal mass. The detection of fatty droplets in ascitic fluid (Figure 1a), increased density of the mesenteric fat, high-attenuation ascites, and thickened peritoneum, together with an adnexal mass with calcified and/or fatty components, indicated a preoperative diagnosis of dermoid cyst with spontaneous rupture.
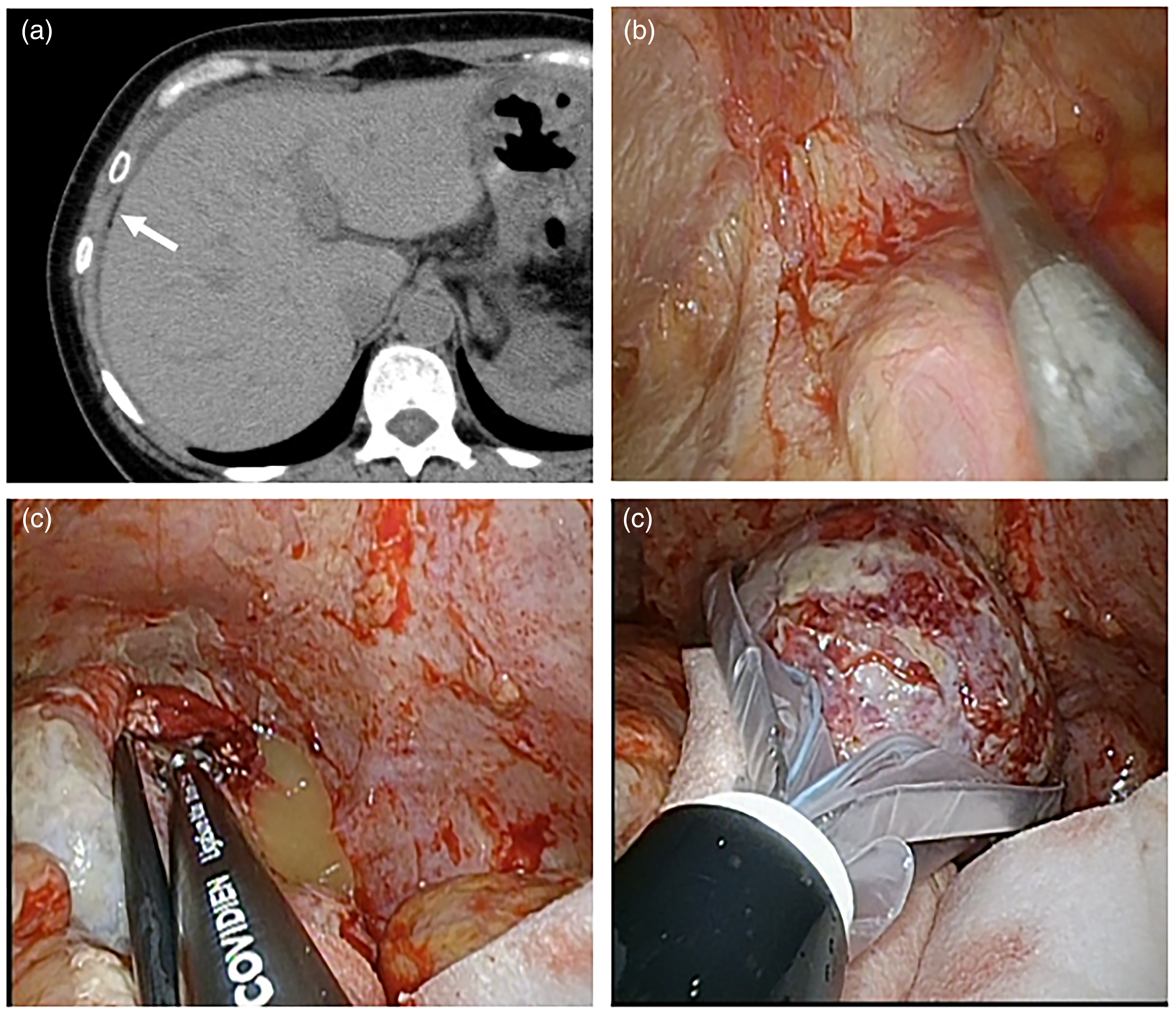
A 55-year-old nulligravid woman (Case 9 in Table 1) presented with lower abdominal pain, loss of appetite, and fever lasting for 15 days. (a) Axial contrast-enhanced abdominal computed tomography showing fatty droplets (arrow) in perihepatic ascites. (b) Laparoscopic view showing severe pelvic adhesion, which was adhesiolyzed by blunt and sharp dissection. (c) Identification of leaked sebaceous material from spontaneously ruptured right dermoid cyst, followed by right salpingo-oophorectomy using a LigaSure Atlas and (d) Extraction of excised tissue through working port after placing in an Endo Catch II retriever bag.
Blood examinations included complete blood count, C-reactive protein (CRP) (normal range: 0–0.14 mg/dL), and serum tumor markers: cancer antigen 125 (CA125) (normal range: 0–35 U/mL), carbohydrate antigen 19-9 (CA19-9) (normal range: 0–37 U/mL), and squamous cell carcinoma antigen (SCC) (normal range: 0–1.5 ng/mL).
Surgical management
Laparoscopic surgery was chosen as the primary surgical procedure (Figure 1b, 1c). 8 All patients provided informed consent prior to surgery, including consent for potential conversion to laparotomy if the intra-abdominal findings were not amenable to laparoscopic surgery. If the patient was in too much pain to understand their condition, their family members were allowed to explain it.
In the event of extensive adhesion, adhesiolysis was carried out by blunt and sharp dissection (Figure 1b). If the patient did not express a wish to salvage the affected ovary, salpingo-oophorectomy was chosen as the primary procedure, with sealing and cutting of the supporting ligaments using a LigaSure Atlas (Covidien Japan, Tokyo, Japan) (Figure 1c). The excised tissue was extracted through the working port after placing it in an Endo Catch II retriever bag (Covidien Japan) (Figure 1d). For patients who wished to preserve the ovary, all efforts were made to achieve this, but immediate conversion to salpingo-oophorectomy was carried out if necrotic changes with progressive gangrene were noted. Laparoscopic surgery was also converted to laparotomy in the event of difficult adhesiolysis.
At the end of surgery, the peritoneal cavity underwent extensive lavage with >3000 mL of saline and a peritoneal drain was placed, if appropriate. After completion of surgery, the volume of intraoperative aspiration was measured and the volume of intraperitoneal lavage fluid was subtracted to estimate the intraoperative blood loss. The removed tissue was weighed and sent for pathological examination.
Patients were monitored closely during the immediate postoperative period to detect complications. Complete blood counts and CRP measurements were performed on the first and third postoperative days. Antibiotic administration was extended in cases with a persistent inflammatory response.
Patients were discharged when they were fully ambulatory and afebrile, as per protocol. They were subsequently monitored carefully for the development of early postoperative comorbidities, such as infection, within 1 month after surgery, and readmission was recommended in the event of postoperative complications, such as relapse of chemical peritonitis.
Clinical data analysis
Extracted data included patient demographics, time from the onset of symptoms to consultation, radiological findings, blood indices, surgical procedures and diagnosis, pathological diagnosis, and postsurgical complications. Statistical analyses were performed using Excel for Microsoft 365 (Microsoft Corp., Redmond, WA, USA) with StatPlus:mac Pro (AnalystSoft Inc., Walnut, CA, USA).
The variables exhibited a nonparametric distribution, as shown by the Kolmogorov–Smirnoff test, and the results were therefore presented as median and range. Variables were compared among the three groups using the Kruskal–Wallis test and continuous variables were compared between two groups using the Mann–Whitney U test. Differences in proportions of categorical variables were evaluated using χ2 tests. A P value <0.05 was considered significant.
Results
Patient demographics and clinical background
Dermoid cysts were surgically confirmed in 1205 patients during the study period (Figure 2), of which 1113 (92.4%) were uncomplicated dermoid cysts. The remaining patients included 83 cases of torsion (6.9%) and nine cases of spontaneous rupture (0.8%) (Table 1).

Flow chart of the summarized case series. There were 1205 surgically confirmed cases of dermoid cysts in the 16-year period (January 2005 to December 2021), including 1113 cases of uncomplicated dermoid cysts (92.4%). Among the complicated cases, torsion and spontaneous rupture occurred in 83 (6.9%) and nine cases (0.8%), respectively. Among the nine cases with dermoid cyst rupture, laparoscopic management after extensive adhesiolysis was possible in eight cases (ovarian cystectomy and salpingo-oophorectomy in three and five cases, respectively), while one patient with severe adhesion underwent salpingo-oophorectomy after laparotomic conversion due to difficult adhesiolysis. Seven patients had uneventful postoperative recovery but two required prolonged administration of antibiotics after readmission due to refractory chemical peritonitis.
Clinical characteristics and surgical outcomes of patients with dermoid cysts complicated by spontaneous rupture.

All patients complained of abdominal pain. One patient developed rupture 25 days postpartum (Case 7 in Table 1), which appeared to be associated with vacuum-assisted delivery with uterine fundal pressure maneuver. No obvious triggers for rupture were identified in the other cases. There were no significant differences among the three groups with respect to age, body mass index, and laterality (Table 2). Parity differed among the groups: Group A included more nulliparous than parous women, while Group B included more parous women, and the numbers of nulliparous and parous women were similar in Group C.
Selected preoperative evaluation values in the three groups.

aAcute, subacute, or chronic manifestations based on duration from symptom onset to surgical management (≤24 hours, 2 days, or ≥2 days, respectively). Cases with unspecified time of symptom onset were classified as chronic manifestation.
There were significant differences in tumor diameter between Groups A and B, but no differences between Groups A and C or between Groups B and C (Table 2) (Figure 3a). The proportion of patients with subacute/chronic presentation (≥2 days after symptom onset) was significantly greater among cases with rupture compared with those with torsion (Tables 1 and 2).
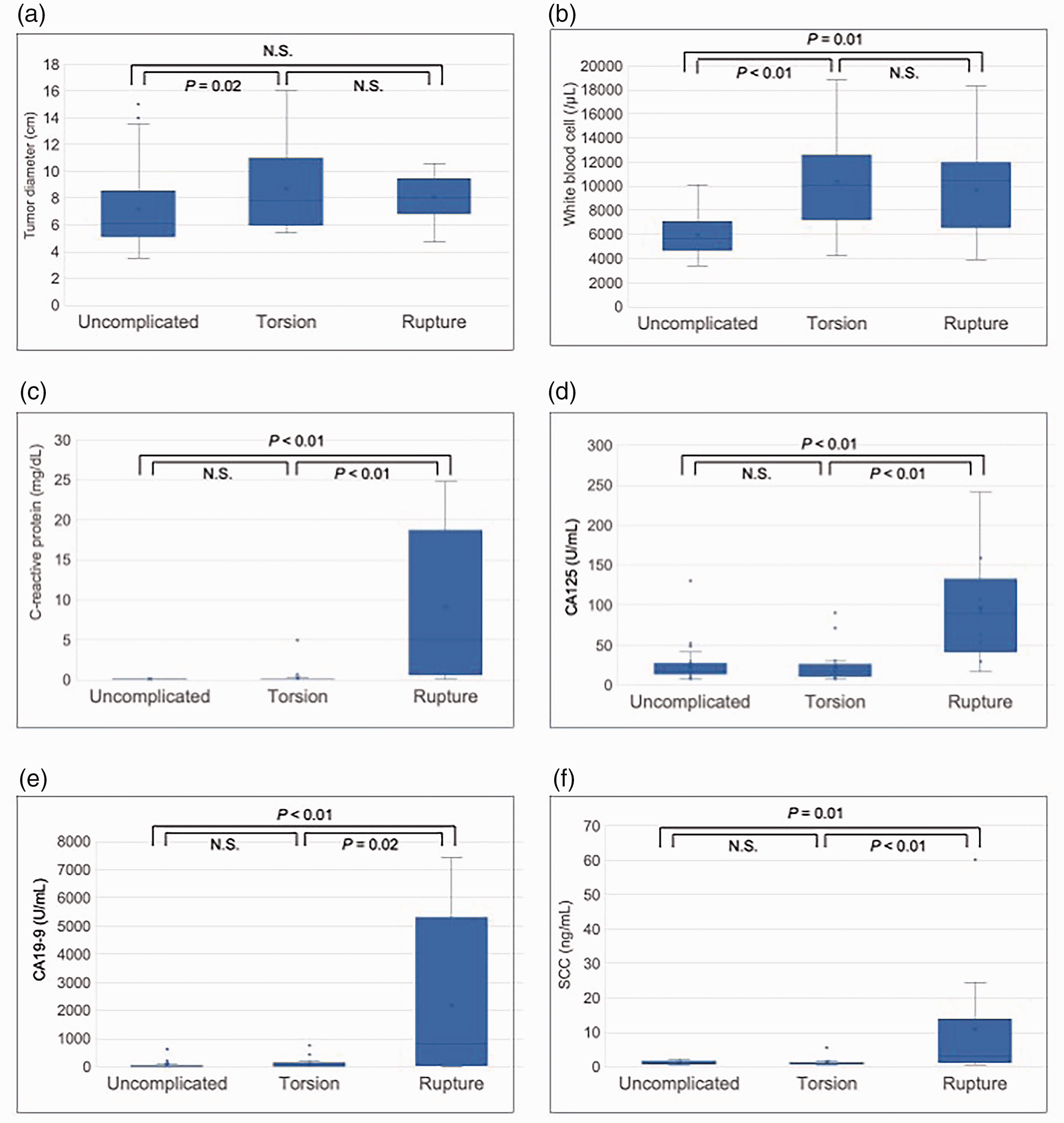
Box-and-whisker plots of variables in patients with uncomplicated dermoid cysts, dermoid cysts with torsion, and dermoid cysts with spontaneous rupture. (a) Tumor diameter; (b) white blood cell count; (c) serum C-reactive protein; (d) cancer antigen 125 (CA125); (e) carbohydrate antigen 19-9 (CA19-9); and (f) squamous cell carcinoma antigen (SCC).
Imaging findings and laboratory indices
CT (Table 1) revealed a pelvic mass with calcification and sebaceous materials indicating an ovarian dermoid cyst in all cases. Rupture was suspected based on increased fat density of the mesentery and high-density ascites in three cases (Cases 2, 4, and 5) and the presence of ascites containing multiple fat droplets and fatty implants in three cases (Cases 7, 8, and 9). No preoperative radiological diagnosis of rupture could be made in the remaining three cases (Cases 1, 3 and 6).
Blood examination (Figure 3) (Table 2) indicated significantly elevated white blood cells in Groups B and C compared with Group A, but no difference between Groups B and C (Figure 3b). CRP (Figure 3c), CA125 (Figure 3d), CA19-9 (Figure 3e), and SCC (Figure 3f) levels were also higher in Group C compared with Groups A and B, suggesting that elevated levels of these parameters may be a preoperative predictor of a ruptured dermoid cyst. Notably, CA19-9 levels were also markedly elevated in Cases 1, 3, and 6 (Table 1), who showed no signs of rupture on preoperative CT imaging.
Surgical and postsurgical outcomes
Laparoscopic management after extensive adhesiolysis was possible in eight cases, including ovarian cystectomy and salpingo-oophorectomy in three and five cases, respectively. Salpingo-oophorectomy was performed after laparotomic conversion in one case with severe adhesions, due to difficult adhesiolysis (Table 1). The postoperative period was uneventful in seven cases, while two patients (Cases 4 and 9) required prolonged administration of antibiotics after readmission due to refractory chemical peritonitis.
Discussion
Dermoid cysts can rupture accidentally during surgery 10 or spontaneously5–7,11; however, spontaneous rupture is rare (reported prevalence: 0.3%–2%) because of their usually thick capsular wall. 11 A similar incidence of rupture (0.8%) was observed in the current case series.
Various events have been suggested to trigger dermoid cyst rupture, 5 including torsion with infarction of the tumor, direct trauma, prolonged pressure due to pregnancy or during delivery, infection of the dermoid contents, malignant transformation, and internal pressure from rapid accumulation of the cystic contents. 11 However, the exact cause of rupture in most cases remains unknown. Similarly, the apparent causative events were unclear in the current case series, except for one postpartum patient who underwent vacuum delivery with fundal pressure maneuver (Case 7).
In the worst-case scenario, rupture of dermoid cysts into the peritoneal cavity, resulting in leakage or spillage of the cyst contents with sebaceous material, may induce chemical peritonitis, which is an aseptic inflammatory peritoneal reaction.5–7,11 The clinical symptoms of chemical peritonitis caused by dermoid cyst rupture may be acute or chronic, depending on the duration and amount of leakage. 5 Acute chemical peritonitis is induced by massive leakage of sebaceous material due to a sudden extensive cyst rupture, while slow leakage through a small tear in the wall of the dermoid cyst may cause chronic granulomatous peritonitis. 12 Chronic manifestations were more common than acute/subacute presentations in the current case series.
Patients with acute disease present with severe acute abdominal symptoms, such as pain, 5 while chronic chemical peritonitis has an insidious symptom onset.5–7,11 Worsening peritoneal damage caused by leaked sebaceous materials may be accompanied by other complications, such as pelvic adhesive disorder or bowel obstruction, abdominal wall abscesses, enterocutaneous fistula formation. 5 Abdominal symptoms therefore develop eventually, even under chronic conditions, including progressive abdominal pain, abdominal distention, fever, and gastrointestinal disturbances such an anorexia, nausea, vomiting, and diarrhea. 13
Timely intensive medical as well as surgical management 14 should thus be considered, irrespective of the manifestations (acute or chronic), to minimize complications, especially chemical peritonitis. This requires ruptured dermoid cysts to be differentiated from a wide range of other gynecological and non-gynecological disorders, especially dermoid cyst torsion.
Ultrasonography is widely accepted in gynecological practice as the initial imaging modality of choice for evaluating acute abdominal events. 1 However, despite recent improvements in the resolution of ultrasound devices and imaging techniques, the method has limited sensitivity for differentiating between cyst rupture and torsion. 6 A diagnosis of a ruptured ovarian dermoid cyst can thus only be made solely by ultrasonography in a small number of cases. 6
CT has been advocated as an adjunct method for diagnosing dermoid cyst rupture when discontinuity of the cyst wall is confirmed, along with intraperitoneal fatty implant, commonly around the liver surface, and increased fat density in the peritoneum.1,12 However, the sensitivity of CT for detecting peritoneal inflammatory changes due to cyst rupture was lower in the current study (66.7%) than in a previous case review (88%). 6
Serum tumor markers are also useful for the diagnosis and management of benign and malignant ovarian tumors. 2 Because dermoid cysts contain well-differentiated tissues derived from the three germ cell layers (ectoderm, mesoderm, and endoderm), elevated levels of tumor markers produced by these tissue components have been demonstrated, not necessarily related to malignant transformation. 2 However, the feasibility of using serum tumor markers as diagnostic markers for dermoid cyst rupture has not yet been clarified.11,15–17
In the current case series, in addition to elevated levels of CRP reflecting the development of chemical peritonitis, CA125, CA19-9, and SCC levels were also raised compared with patients with uncomplicated dermoid cysts and torsion. This also applied in three patients with no apparent CT findings indicative of rupture, while elevated white blood cell counts could not differentiate rupture from torsion.
CA125 is normally expressed in coelomic epithelia, such as Müllerian epithelium, peritoneum, pleura, and pericardium.18,19 Elevated levels of CA125 are commonly found in patients with ovarian malignancies or other benign gynecological disorders, such as endometriotic cysts and adenomyosis.18,19 High CA125 levels have also been shown in patients with ascites unrelated to malignant conditions, or patients with peritoneal inflammatory disease, mostly due to increased reactive production of CA125 in peritoneal cells under such conditions.18,19 Cases of dermoid cysts associated with elevated CA125 levels have rarely been reported.2,15–17 The significant elevation of CA125 levels in patients with ruptured dermoid cysts in the current series may thus be attributable to the increased expression of CA125 in peritoneal cells stimulated by chemical peritonitis associated with ascites pooling, rather than the increased production of CA125 by the dermoid cyst itself. 2
CA 19-9 is highly expressed by adenocarcinomas of the digestive tract, 2 while the Müllerian duct-derived mucosa of the uterus and fallopian tubes can also produce CA19-9. 2 Immunohistochemical staining of dermoid cysts also showed that CA19-9 was expressed by bronchial epithelial cells. 2 The increased levels of CA19-9 in uncomplicated dermoid cysts are primarily caused by leakage of accumulated CA19-9 from the cystic cavity into the bloodstream. 2
SCC is synthesized by the squamous cell epithelium and is used as a marker of squamous cell carcinoma in various organs. 20 Regarding gynecological malignancies, in addition to cervical cancer, squamous cell carcinomas arising in dermoid cysts can also show elevated SCC levels. 21 Serum SCC levels were also shown to be increased in blood samples contaminated with small pieces of skin tissue, or in patients with dermatological diseases.20,21 Elevated serum SCC levels occasionally occur in patients with dermoid cysts due to its production by lining epithelial squamous cells and leakage into the general circulation. 21
Although actual mechanisms responsible for the elevated levels of CA19-9 and SCC in the current series of patients with ruptured dermoid cysts are unknown, they may be attributable to the secondary release of accumulated cyst contents containing CA19-9 and SCC into the peritoneal cavity. The identification of elevated tumor markers, especially CA19-9 and SCC, in addition to elevated CRP as an inflammatory marker, may thus facilitate the diagnosis of a ruptured dermoid cyst at the initial presentation, even in patients with equivocal imaging findings, while elevated CA125 may reflect the presence of chemical peritonitis.
Once rupture of the dermoid cyst is diagnosed or highly suspected, immediate surgical intervention is needed to remove the ovarian cyst, along with thorough peritoneal lavage,5–8,11,14 although conservative non-surgical management can be considered on extremely rare occasions. 15 Laparoscopic surgery is an accepted feasible option for the surgical management of dermoid cysts. 10 Although ruptured dermoid cysts can also be managed effectively by laparoscopy, 6 a previous review of case reports found that most spontaneously ruptured dermoid cysts were initially managed via laparotomy. 6 This preference for a laparotomic approach could mostly be due to concerns over possible injury to adjacent organs, such as the bowel, during the dissection of severe adhesions caused by chemical peritonitis. 14
Laparoscopic surgery is the primary surgical approach for benign adnexal masses in our department, 8 and was therefore chosen for the management of ruptured dermoid cysts in the current case series. All procedures were successful with careful dissection, except for one case that required conversion to laparotomy due to significant concerns regarding bowel injury during adhesiolysis.
Minimizing the risk of chemical peritonitis is a key concern after the surgical removal of ruptured dermoid cysts.6,11 However, extensive peritoneal lavage to remove leaked sebaceous contents is generally sufficient to prevent prolonged chemical peritonitis, and the postoperative prognosis is therefore favorable in most cases. 11 In some cases, the contents of the cyst may form firm peritoneal implants or nodules that are difficult to remove from the peritoneal surface. Information on the management of chronic granulomatous peritonitis following spontaneously ruptured dermoid cysts is scarce,11,15 but prophylactic or therapeutic antibiotics are generally effective in such cases, as shown in two cases in the current report. Furthermore, prolonged use of systemic corticosteroids, 11 and even the immunosuppressive drug, azathioprine, may be required to improve the postoperative resolution in cases of chronic granulomatous peritonitis. 22
The current study had several limitations. First, the rarity of the condition meant that this retrospective study included only a limited number of cases with ruptured dermoid cysts at a single center, and further studies with larger numbers are needed to validate the results. Second, because of the small number of cases, this study included cases experienced over a relatively long period, which may have influenced the outcomes, although similar diagnostic and surgical procedures were carried out by the same physicians throughout the study period. The obtained results need to be verified by expanding the number of cases in the future. Furthermore, the study may have been affected by selection bias, and patients from multiple centers should be included in future studies to reduce selection bias.
Conclusion
Spontaneous rupture of dermoid cysts is a relatively rare event, accounting for only 0.8% of dermoid cysts in the current series, and resulting in a more chronic clinical course than torsion. The combined use of CT imaging and detection of elevated levels of CRP, CA125, CA19-9, and SCC may help to differentiate between cyst rupture and torsion at the initial evaluation. Laparoscopic surgery may be a feasible option, but prompt conversion to laparotomy should be considered in cases of difficult adhesiolysis. Notably, refractory chemical peritonitis may occur even after successful surgical management with extensive peritoneal lavage.
Footnotes
Acknowledgements
Author contributions
Akihiro Takeda and Wataru Koike conceived and designed the study. Akihiro Takeda and Wataru Koike collected the data. Akihiro Takeda analyzed the data and wrote the manuscript. Wataru Koike assisted with the data analysis. All authors have read and approved the final manuscript.
Data availability statement
The original research data supporting the results/tables/figures presented in the manuscript are available on reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.