
Abstract
Objective
Keratoconus is a corneal ectasia that leads to thinning and steepening of the corneal surface. We aimed to assess the relationship between quality of life and corneal tomography indices, irrespective of visual acuity.
Methods
This was a cross-sectional study using a translated and validated Keratoconus Outcomes Research Questionnaire (KORQ) in Arabic language. We screened patients with keratoconus using the Belin/Ambrósio D-Index. We included the best-seeing eye in each patient with keratoconus, with a best corrected visual acuity better than 0.5. We collected variables including KORQ scores, flattest meridian keratometry, steepest meridian keratometry, mean keratometry front, maximum simulated keratometry, astigmatism front, Q value front, and thickness at the thinnest location. We performed linear regression analysis to identify predictors of the visual function score and symptom score.
Results
Sixty-nine patients were included in this study, 43 (62.3%) male and 26 (37.7%) female patients, with a mean age 34.0 ± 11.50 years. The only predictor for visual function score was sex (β = 11.64, 95% confidence interval: 3.50–19.78). None of the topographic indices were related to quality of life.
Conclusion
In this study, quality of life in patients with keratoconus was not related to specific tomography indices and might be related to visual acuity itself.
Introduction
Keratoconus is a corneal ectasia that leads to thinning and steepening of the corneal surface, which impairs visual acuity.1–3 Keratoconus negatively impacts the patient’s quality of life (QoL), with the effect of keratoconus on visual acuity being the main impact.4,5 Patients with keratoconus experience mild blurring or slightly distorted vision, which is often treated with contact lenses or eyeglasses. 6
Several research groups have sought to establish a tool that can reliably assess the subjective impact of keratoconus on QoL. 7 The Keratoconus Outcomes Research Questionnaire (KORQ) was developed as an instrument to measure patient-reported outcomes specifically among patients with keratoconus. 8 The KORQ was further assessed in terms of psychometric properties in 2020, and its reliability was confirmed. 9 A recent review of questionnaires used to measure QoL in patients with keratoconus concluded that KORQ was the only validated keratoconus-specific questionnaire and had superior psychometric properties. 7
The evaluation of health-related QoL outcome indicators in patients with keratoconus has received increased interest because such assessment might reveal a worse QoL in these patients, despite having a best corrected visual acuity (BCVA) of 1.0. 10 Such a finding that might suggest the presence of high-order aberrations that could affect QoL itself, irrespective of visual acuity.
Whether keratoconus has an impact on QoL, independent of the effect of visual acuity, is not yet understood. In this work, we aimed to assess the association of the KORQ with objective tomography indices extracted using Pentacam tomography to find indices that might affect QoL among patients with keratoconus. Additionally, we developed a validated Arabic version of the KORQ for use in future research.
Methods
Study design
This was a cross-sectional study conducted from August 2020 to January 2021 in a hospital among patients with keratoconus diagnosed in the previous 6 months. The study hospital is a 600-bed tertiary care teaching center. Ethical approval for this study was waived by the institutional review board of the University of Jordan. The ethical principles related to human rights and professional integrity laid down in the Declaration of Helsinki were followed in the conduct of the study. Informed verbal consent was obtained from all patients.
Participants
We reviewed Pentacam tomography (OCULUS Pentacam® HR; Oculus Inc., Arlington, WA, USA) images from patients who visited the ophthalmology clinic from August 2020 to January 2021. The Belin/Ambrósio D-Index (BAD-D) was used to screen all patients with keratoconus. The BAD-D index is an index automatically calculated by the Pentacam software in regression analysis using nine parameters. The BAD-D has previously been found to be reliable in keratoconus screening. 11 According to previous studies, a cut-off value for the BAD-D of 1.88 was used to screen patients with potential keratoconus for study inclusion.12,13 Among those who were screened, we included only one eye from each patient after measuring the BCVA in both eyes. To recruit participants with similar visual acuity for better comparisons, we only included the best-seeing eye in each patient, with a BAD-D value of more than 1.88, a BCVA of 0.5 or better, and no previous corneal transplantation surgery.
Variables
All included participants were contacted via telephone to obtain verbal consent to participate in the study. After agreeing to participate, patients were asked to complete the KORQ in Arabic, the official language in the study area. The questionnaire was translated from English to Arabic and then translated back to English to ensure accuracy of the Arabic translation (Appendix). Reliability analysis indicated that the Arabic version of the KORQ had good validity, with Cronbach’s alpha for the 18 visual function questions of 0.874 and that for the 11 symptom questions of 0.783.
The KORQ includes two types of questions: visual function questions and symptom questions. Visual acuity questions comprise 18 items to assess the impact of keratoconus on daily activities such as reading, watching television, and driving. These questions are intended to understand how the individual’s vision affects their ability to perform daily tasks. Symptom questions comprise 11 items focusing on subjective symptoms experienced by the individual such as eye pain, sensitivity to light, and blurred vision. These questions are used to understand the extent to which the individual is affected by their symptoms and how symptoms impact their QoL. Answers were scored as follows: “Not at all” = 3, “A little” = 2, “Quite a bit” = 1, “A lot” = 0, with a higher score for each question denoting better QoL and less impact on QoL owing to keratoconus. To allow for comparisons between of visual function domain and symptom domain with objective topographic indices, a total percentage score for each domain was calculated as follows: visual function score = (sum of scores on the 18 visual function questions)/18 × (100/3) and symptom score = (sum of scores on the 11 symptom questions)/11 × (100/3).
The following topographic indices were obtained for comparison once the KORQ was completed: flattest meridian keratometry, steepest meridian keratometry, mean keratometry front, maximum simulated keratometry, astigmatism front, Q value front, and thickness at the thinnest location.
We obtained visual acuity measured in decimals for the better-seeing, included eye as well as for the other eye. We converted counting fingers visual acuity into 0.014. 14
Statistical analysis
We used IBM SPSS version 26.0 (IBM Corp., Armonk, NY USA) for the statistical analysis. Continuous variables are described using mean ± standard deviation and nominal variables are described as frequency and percentage. The reliability of the questionnaires was determined according to Cronbach’s alpha.
We used an independent samples t-test to analyze the mean difference between sexes and each KORQ score; the data are presented as mean difference and 95% confidence interval (CI). We performed linear regression analysis to determine those variables that can predict visual function score and factors that can predict symptom score by estimating the beta coefficient (β) and 95% CI. We adopted a model building strategy where we performed Pearson correlation for continuous variables and the chi-square test for categorical variables to analyze factors with a significant correlation to these scores, with an inclusion significance threshold of p < 0.1. All underlying assumptions were met. A p value <0.05 was considered statistically significant.
Results
Sixty-nine patients with keratoconus were eventually included in this study, with a mean age of 34.0 ± 11.50 years (range, 14–66 years). Forty-three (62.3%) male and 26 (37.7%) female participants were included. Table 1 demonstrates the characteristics of the included patients.
Characteristics of the included participants.

KC, keratoconus; BCVA, best corrected visual acuity; K1, flattest meridian keratometry; K2, steepest meridian keratometry; Kmax, maximum keratometry; KPD, keratometric power deviation.
*Keratoconus Outcomes Research Questionnaire.
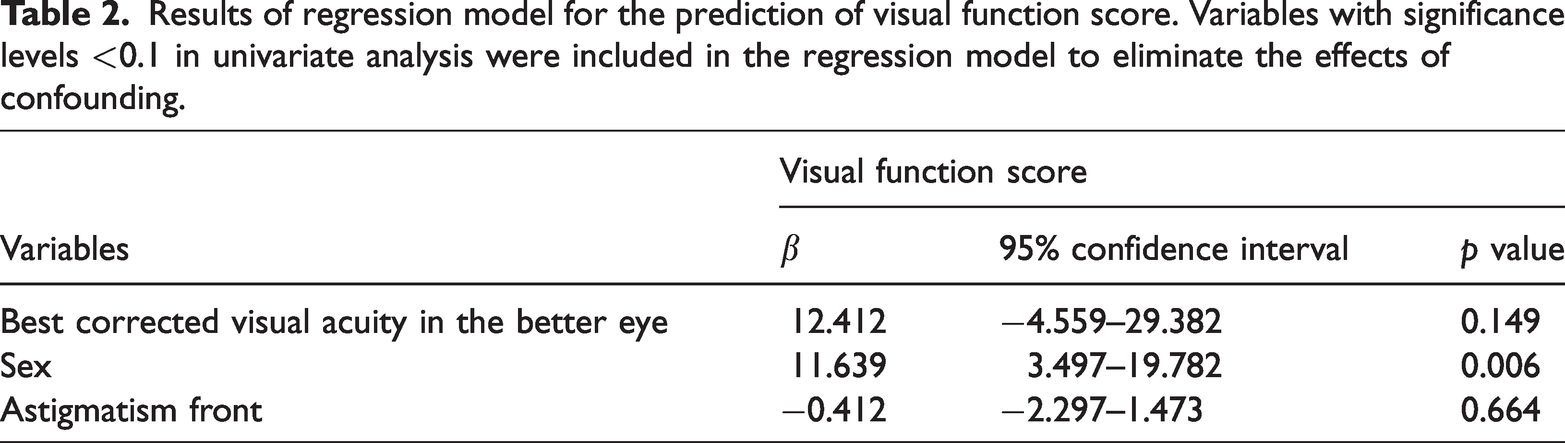
Variables that showed potentially significant associations (p < 0.1) in the univariate analysis were included in the linear regression model to control for possible confounding factors; these variables included sex (p = 0.001), BCVA in the better-seeing eye (p = 0.022), and astigmatism (p = 0.099). The model had an R value of 0.425 with an ANOVA significance of 0.005. The only significant predictor for visual function score was sex (β = 11.64, 95% CI 3.50–19.78, p = 0.006). BCVA in the better-seeing eye and astigmatism were not significant predictors in the regression model. Table 2 shows the results of the regression model for visual function score prediction.
Results of regression model for the prediction of visual function score. Variables with significance levels <0.1 in univariate analysis were included in the regression model to eliminate the effects of confounding.
Upon comparing sex differences with regard to visual function and symptom scores, there was a significant difference for visual function score only (p = 0.001; mean difference 13.35, 95% CI 5.48–21.23), with a mean visual function score for female patients of 81.27 ± 15.76 and 67.92 ± 5.95 for male patients. For symptom score, scores for female patients were higher, with a mean of 62.35 ± 22.2, as compared with the mean score of 55.81 ± 18.32 for their male counterparts. However, this difference did not reach statistical significance. Figure 1 depicts the sex differences in KORQ scores.

Sex differences in visual function score and symptom score on the Keratoconus Outcomes Research Questionnaire.
We used linear regression to analyze the predictors of symptom score. Variables with a p value <0.1 in univariate analysis were entered into the model. These included the duration of keratoconus (p = 0.067) and Q value (p = 0.065). The model had an R value of 0.231 with an ANOVA significance of 0.169. None of the variables included in the model was able to predict the symptom score. Table 3 details the results of the regression model for symptom score prediction.
Results of regression model for the prediction of symptom score. Variables with significance levels <0.1 in univariate analysis were included in the regression model to eliminate the effects of confounding

Discussion
Our study was conducted in a well-curated sample with strict exclusion criteria. We used a version of the KORQ translated into Arabic and validated. Then, we collected the topographic indices of the included patients and investigated the predictors of both visual function score and symptom score in the KORQ. Our data showed that sex was the only significant predictor of visual function score in multivariate regression analysis, despite astigmatism being significantly related to visual function in tomography. For the symptom score, none of the variables reached the threshold for statistical significance in multivariate regression analysis.
In a previous study that recruited patients with keratoconus who had a BCVA of 1.0, the authors reported an improvement in QoL after the cross-linking procedure, which they related to the decentration caused by keratoconus itself, measured in topographic images. 10 We did not find any corneal tomography indices that might be correlated to QoL, irrespective of visual acuity. In another study that assessed data from the Collaborative Longitudinal Evaluation of Keratoconus Study, the authors concluded that the visual acuity of the best-seeing eye has the greatest influence on patient QoL, irrespective of corneal steepening. 15 In longitudinal studies assessing the QoL of patients with keratoconus before and after treatment using refractive laser and cross-linking, or cross-linking alone, the authors reported improved QoL and visual acuity.16,17 Other studies have found a strong relationship between patients' worse QoL indices and the visual acuity in their best-seeing eye.18,19 In this study, we did not investigate topographic indices of the worst-seeing eye, an approach that has been previously confirmed. 20
A similar study on QoL in patients with keratoconus that used the KORQ found lower visual function scores in male patients. 21 This is in accordance with our results showing that male patients had a lower mean visual function score than female patients. A study among over 100 patients with keratoconus found that men responded differently than women to QoL questions related to vision, explaining the difference in QoL scores. 22 A small-sample study did not find a sex difference with regard to QoL in patients with keratoconus. 18 Such findings mandate further studies among patients with keratoconus in which correcting for sex-related confounding effects in assessing other variables is considered. Moreover, various studies have found that BCVA in the better-seeing eye is related to QoL.21,22 However, according to our findings, the BCVA in the better eye was not a significant predictor in the regression model, even though it had a significant correlation with the visual function score in univariate analysis. Another study suggested that vision in the better-seeing eye has a significant influence on the patient’s QoL and should be taken into account when assessing the impact of keratoconus, as well as focusing on treating the better eye rather than the worse eye, according to the patient’s preferences. 20 In a recent cross-sectional study that included 100 patients with keratoconus who completed the KORQ, BCVA in the better eye and a history of cross-linking were found to factors associated with better QoL scores. 21
The KORQ was previously translated and validated in the populations of Brazil, 21 Colombia, 23 and Italy. 24 The KORQ has been found to be a reliable and well-validated questionnaire. However, its main limitation is its length, with responses to 29 questions needed to construct both scores, a limitation that newer questionnaires seek to resolve. 25 Moreover, newer questionnaires are attempting to incorporate emotional assessment to determine the psychological impact of keratoconus. 26 The Arabic version of the KORQ used in this study showed good validity in the visual function domain and symptom domain.
The main limitation of the current study is the limited number of participants, which was mainly owing to the strict inclusion criteria, via which we aimed to include participants with comparable visual acuity. The importance of having participants with comparable, relatively good visual acuity is according to the findings of previous studies showing that a visual acuity worse than 20/40 is associated with worse QoL for nearly all ocular measures. 4 Thus, including only participants with visual acuity better than 20/40 allowed us to assess the effect of other factors, irrespective of visual acuity. Moreover, taking into consideration that this was a cross-sectional QoL study, we could not establish any causal relationships in the absence of longitudinal evaluation. Future studies should consider assessing other objective measures that could contribute to patient QoL (e.g., contrast sensitivity) to better understand the association between clinical parameters and patient QoL.
Conclusion
We found that the effects of keratoconus on patient QoL was not related to specific topographic indices. Moreover, we found that QoL in male patients was generally more affected by keratoconus in comparison with female patients. We also developed a validated Arabic version of the KORQ in this study.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231170549 - Supplemental material for Quality of life and tomography indices in patients with keratoconus
Supplemental material, sj-pdf-1-imr-10.1177_03000605231170549 for Quality of life and tomography indices in patients with keratoconus by Muawyah Al Bdour, Saif Aldeen AlRyalat, Razan Salameh, Laith Alomari, Ahmad Riyalat, Zaid Fakhouri, Laith Al-Abdallat, Kamal Naser, Mohammad A. Alshrouf and Ahmad Al-Amer in Journal of International Medical Research
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.