
Abstract
Objective
To compare the incidence of falls between patients with visually significant cataracts in both eyes and those who have undergone first-eye cataract surgery.
Methods
This retrospective case–control study involved patients with a history of cataracts in both eyes who had undergone first-eye cataract surgery within the past 9 to 12 months (pseudophakic group). The control group comprised patients with cataracts in both eyes (cataract group). We assessed best-corrected visual acuity (BCVA), systemic comorbidities and medications (using the Charlson comorbidity index), and independent daily activities (using the Lawton Instrumental Activities of Daily Living scale). The patients were questioned about experiencing two or more falls in the last 6 months.
Results
Each group comprised 50 patients. Binocular BCVA was significantly better in the pseudophakic group (0.05 ± 0.06 logMAR) than in the cataract group (0.77 ± 0.34 logMAR). Of all participants, 22% reported experiencing two or more falls in the last 6 months. Multivariate analysis demonstrated significantly better BCVA in participants with less than two falls.
Conclusions
Patients of advanced age with visually significant cataracts in both eyes are at a higher risk of falling. First-eye cataract surgery may mitigate the occurrence of falls by improving binocular BCVA.
Introduction
Falls among individuals of advanced age represent a significant health concern. The annual incidence of falls is 33% among individuals aged >65 years and 50% among those aged >80 years. 1 Although most falls have no substantial consequences and resolve without professional intervention, a substantial proportion lead to medical consultations, hospitalization, and prescribed periods of physical inactivity.2–4 Notably, approximately 15% of falls culminate in fractures, with a minimum of 5% resulting in severe soft tissue injuries or head trauma. 5 The aftermath of such falls can have far-reaching impacts on an individual’s lifestyle, encompassing reduced functional capacity, heightened dependency, social isolation, depression, anxiety, and a surge in medical service requests and referrals.6,7
Although medical conditions such as dementia, osteoarthritis, cerebrovascular incidents, and movement disorders such as Parkinson’s disease undoubtedly heighten the susceptibility to falls, it is imperative to recognize that normal age-related physiological changes can also render otherwise healthy individuals more prone to falling.1,8–10
Many studies have established a link between compromised visual function and an increased risk of falls.11–13 Diminished visual acuity, a restricted visual field, reduced contrast sensitivity, and impaired stereopsis collectively predispose individuals to falls. Notably, various researchers have proposed that the presence of cataracts elevates the risk of falls and this risk can be mitigated through lens extraction.14–17
Against this backdrop, the present study was performed to compare the incidence of falls between individuals with cataracts and those who have undergone cataract surgery. By evaluating the impact of cataract surgery on fall rates, we endeavor to contribute to the broader understanding of how visual interventions may mitigate the risk of falls in patients of advanced age.
Methods
Study Design and Participants
The reporting of this study conforms to the STROBE guidelines. 18 This retrospective case–control study was conducted from January 2018 to June 2019 at the eye clinic of 5-Azar Hospital in Gorgan, Iran. The participants were selected using convenience sampling and enrolled consecutively based on specific criteria. The groups were matched by age and sex. The pseudophakic group comprised patients with a history of visually significant cataracts in both eyes who had undergone first-eye cataract surgery within the preceding 9 to 12 months. The surgical procedures were performed exclusively by a single surgeon (MAK) using a standard phacoemulsification technique accompanied by the implantation of a one-piece hydrophobic acrylic intraocular lens (enVista; Bausch & Lomb, Vaughan, Ontario, Canada). Patients in the cataract group, serving as controls, were selected based on the presence of binocular visually significant cataracts. The criterion for significant cataract was a Snellen best-corrected visual acuity (BCVA) of less than 20/40, attributable to lens opacity. 19
Ethical Considerations
The study adhered to the principles outlined in the Declaration of Helsinki. Written consent was obtained from all participating patients. The Ethics Committee of The Golestan University of Medical Sciences approved the study (ethics code: IR.GOUMS.REC.1397.164). Furthermore, all participants’ data were de-identified.
Ophthalmic Assessments
A single examiner (MAK) conducted comprehensive ophthalmic examinations of all participants, including autorefractometer measurement of refractive errors, monocular and binocular BCVA assessments, slit-lamp biomicroscopy, Goldmann tonometry for intraocular pressure measurement, and dilated fundus examinations using a 90-diopter lens. Logarithm of the minimal angle of resolution (LogMAR) equivalents were assigned to BCVA values for statistical analysis. Participants below the age of 50 years; those with significant refractive errors (spherical equivalent of <−2.00 or >+2.00 diopters), visual field defects, any comorbid eye diseases (including diabetic retinopathy, glaucoma, or macular degeneration), a history of ocular surgeries in either eye, or cognitive impairment (assessed via the Mini-Mental State Examination); and individuals unable to walk independently were excluded from the study. 20
Data Collection and Analysis
Systemic comorbidities and medications were documented using the Charlson comorbidity index (CCI). 21 The patients’ independent daily activities were assessed using the Lawton Instrumental Activities of Daily Living (IADL) scores. 22 Participants were questioned about experiencing two or more falls during the last 6 months. A fall was defined as unintentionally coming to rest on the ground or at a lower level, with or without loss of consciousness. 23
Statistical analysis was performed using SPSS software version 24 (IBM Corp., Armonk, NY, USA). Descriptive statistics were employed for continuous and categorical variables. Between-groups comparisons were performed using the t-test (continuous variables) and the chi-square test (categorical variables). Multiple linear regression analysis was performed to evaluate the relationship and predictability of independent variables on the falling rate as the dependent variable. Furthermore, Pearson’s coefficient was used to calculate correlation coefficients between the variables. A P value of <0.05 was considered statistically significant.
Results
The pseudophakic and cataract groups comprised 50 patients each. The patients’ demographics are summarized in Table 1. The patients’ mean age was 66.50 ± 8.68 years in the pseudophakic group and 63.68 ± 8.29 years in the cataract group. No significant differences were observed in age, sex, CCI score, or IADL score between the two groups. Notably, binocular BCVA was markedly better in the pseudophakic group (0.05 ± 0.06 logMAR) than in the cataract group (0.77 ± 0.34 logMAR, P < 0.001).
Demographics and binocular BCVA in the pseudophakic and cataract groups.
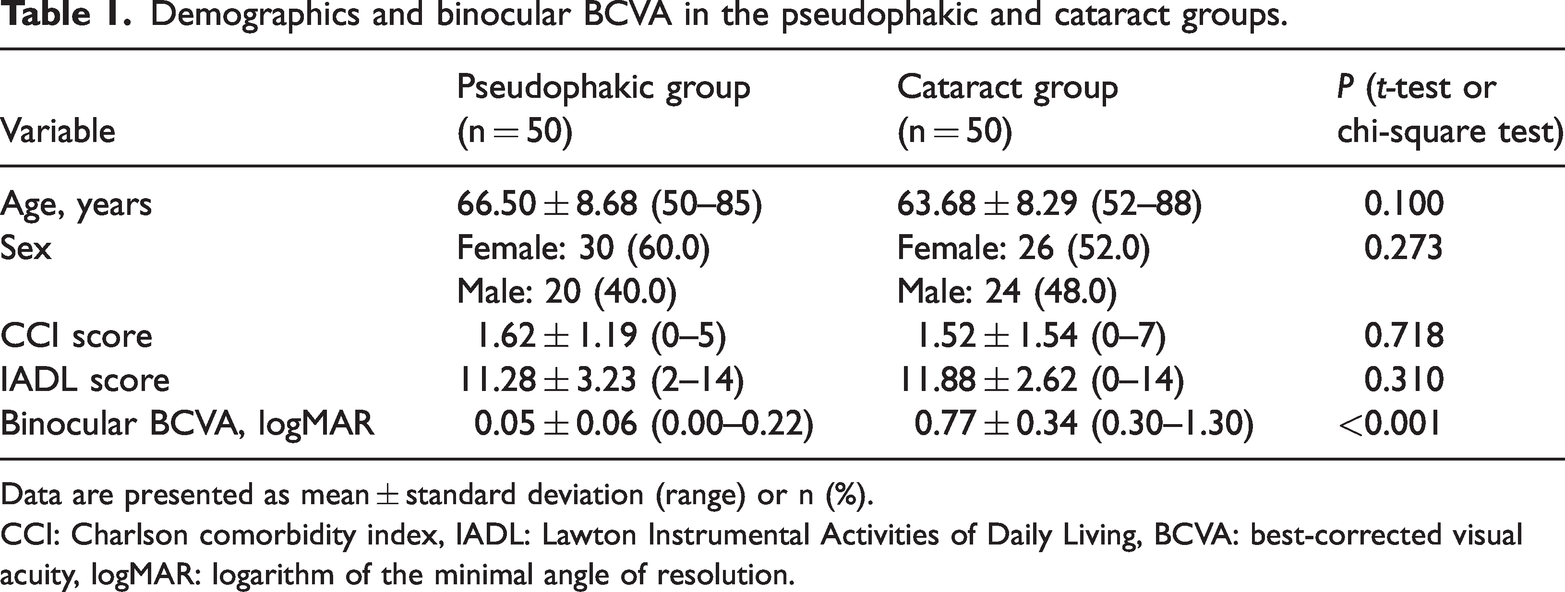
Data are presented as mean ± standard deviation (range) or n (%).
CCI: Charlson comorbidity index, IADL: Lawton Instrumental Activities of Daily Living, BCVA: best-corrected visual acuity, logMAR: logarithm of the minimal angle of resolution.
Among all participants, 78% reported experiencing no or one fall within the preceding 6 months, while 22% indicated two or more falls in the same period. In the multivariate analysis using multiple linear regression, variables including age, sex, CCI score, IADL score, and history of cataract surgery showed no statistically significant associations with the occurrence of two or more self-recalled falls within the previous 6 months. Importantly, the sole variable that demonstrated a significant difference between the two fall frequency groups was binocular BCVA, which proved better among participants with fewer than two falls (P = 0.003) (Table 2).
Distribution of two or more falls during the last 6 months according to demographics, history of cataract surgery, and binocular BCVA
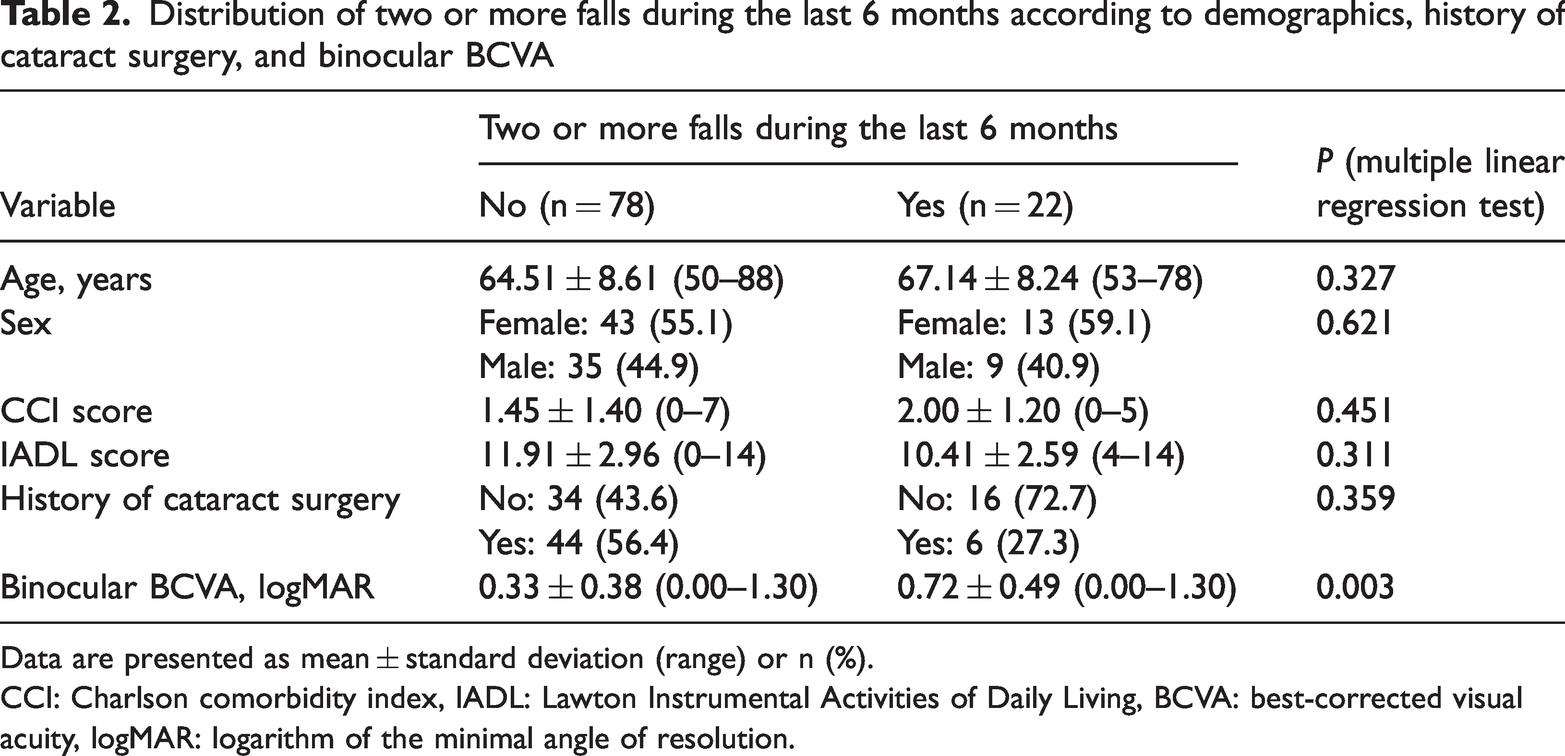
Data are presented as mean ± standard deviation (range) or n (%).
CCI: Charlson comorbidity index, IADL: Lawton Instrumental Activities of Daily Living, BCVA: best-corrected visual acuity, logMAR: logarithm of the minimal angle of resolution.
A significant negative correlation emerged between binocular BCVA and the falling rate (P < 0.001, r = −0.375). Additionally, the CCI score showed a significant negative correlation with the IADL score (P < 0.001, r = −0.350).
Discussion
This study was performed to assess the fall rates among individuals with visually significant cataracts in both eyes versus those who had recently undergone first-eye cataract surgery. We found that individuals with better binocular BCVA exhibited a significantly lower incidence of two or more self-recalled falls within the previous 6 months. This corroborates existing literature, which has consistently demonstrated a notable correlation between visual acuity and the risk of falling.24–26 Moreover, several researchers have suggested that surgical interventions aimed at improving visual acuity can effectively reduce the likelihood of future falls.14,27–29 For instance, Feng et al. 28 reported a 54% decrease in the risk of falls after timely first-eye cataract surgery and a 73% reduction after second-eye surgery. Similarly, To et al. 30 documented a 78% fall reduction following the first eye surgery and an 83% decrease after the second eye surgery. Other studies have also revealed statistically significant postoperative reductions in the number of falls after lens extraction.16,23 These findings collectively underscore the potential for interventions, including cataract surgery, to reduce the risk of falls in older individuals by enhancing their visual acuity.
Interestingly, our study also revealed that participants reporting fewer than two falls displayed higher independent daily activity levels (based on IADL scores) and a lower burden of systemic comorbidities (based on CCI scores). However, these differences failed to attain statistical significance in the multivariate analysis. Moreover, we identified a negative correlation between the CCI and IADL scores, a trend consistent with prior research.11,31–33
It is important to acknowledge the limitations of our study, including its retrospective design, potential recall bias regarding self-reported falls, and relatively small sample size. Additionally, we did not assess other facets of visual function, such as contrast sensitivity or stereopsis.
In conclusion, our findings suggest that individuals of advanced age with visually significant cataracts in both eyes are at an elevated risk of falling. Notably, first-eye cataract surgery is a promising intervention that may reduce the occurrence of falls by improving binocular visual acuity.
Footnotes
Acknowledgements
The authors are grateful to the research participants and all the hospital staff who took interest in and assisted with the study.
Authors’ contributions
MAK designed the study, supervised the project, and performed the ophthalmic examinations and surgeries. HH, MN, AG, and FA collected the data. SC, SH, and AZ performed the statistical analysis. FA, SH, SSA, and MKF wrote and revised the main manuscript text. All the authors read and approved the final manuscript.
Data availability
The datasets used during the current study are available at the Department of Ophthalmology, 5-Azar Hospital, Golestan University of Medical Sciences, Gorgan, Iran. The data are not available publicly for confidentiality reasons. However, the data can be obtained from the corresponding author upon reasonable request
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.