
Abstract
Objective
To examine the effectiveness of decortication to treat chronic tuberculous empyema (TE) using uniport video-assisted thoracoscopic surgery (VATS) versus conventional triport VATS.
Methods
Data from consecutive patients with stage II or III TE who underwent decortication with either uniport VATS (uniportal group) between July and December 2017, or triport VATS between January and July 2018 (triportal group), were retrospectively analysed. VATS procedures were performed under general anaesthesia with double lumen endotracheal intubation and clinical outcomes were compared between the two groups.
Results
Clinical data were comparable between the groups (20 patients in each) regarding demographic and baseline characteristics, operative and postoperative characteristics, surgical procedure-related complications, and postoperative adverse events. No surgical procedure-related complications occurred during the perioperative period in either group. Threshold values for mechanical pain at 8 h postoperatively were significantly higher in the triportal group versus the uniportal group. Furthermore, the incidence of nausea and vomiting was significantly lower in the uniportal versus triportal group. In the triportal group, one patient required readmission and further intervention due to recurrence.
Conclusions
Uniport VATS decortication for stages II and III TE may be a feasible and safe procedure in selected patients. Moreover, uniport VATS may be less painful than triport VATS.
Keywords
Introduction
Tuberculosis (TB) remains a serious threat to global public health. Tuberculous empyema (TE) is a rare form of pleural infection caused by TB, characterized as a purulent infection of the pleural space with pleural effusion containing TB bacilli. 1 According to the American Thoracic Society, an empyema can be classified into three progressive stages (stages I, II, and III). 2 Besides anti-TB drug therapy, surgical management is recommended as a treatment option for patients with stages II and III TE. Surgery is beneficial to diagnose the disease condition, remove fluid, allow the trapped lung to re-expand, reduce the impairment of pulmonary function, and prevent collapse of the chest wall. 3
Several studies into the role of decortication or debridement in the management of TE have confirmed that conventional video-assisted thoracoscopic surgery (VATS), using two or three ports, is feasible and safe.4–6 Uniport VATS was recently introduced as a novel procedure for various thoracic surgical procedures, including wedge resection, lobectomy, segmentectomy, and sleeve lobectomy.7–10 To date, no articles have been published on the use of uniport VATS decortication and debridement in patients with stages II and III TE.
The aim of the present study was to compare uniportal decortication with triportal decortication regarding the short-term outcomes for postoperative analgesia in patients with stages II and III TE.
Patients and methods
Study design and study population
The reporting of this study conforms to STROBE guidelines. 11 This retrospective cohort study included data from patients treated at the Department of Thoracic Surgery, The Third People’s Hospital of Shenzhen, China – a 1500-bed hospital. The study protocol was approved by The Third People's Hospital of Shenzhen Ethics Committee, and the requirement of written informed consent was waived by the ethics committee due to the anonymous retrospective nature of the study. All patient details were de-identified.
Consecutive patients diagnosed with stage II or III TE based on a combination of clinical symptoms, radiological findings, pleural adenosine deaminase, histological examination, T-SPOT.TB Test (Oxford Immunotec, Oxford, UK), and GeneXpert (Cepheid, Sunnyvale, CA, USA), and who received either uniport VATS (TC201, Karl Storz, Tuttlingen, Germany; 10 mm diameter) decortication and debridement between July 2017 and December 2017, or triportal decortication (introduced to improve pain relief and promote postoperative recovery) between January 2018 and July 2018, were enrolled into the study.
Enrolment criteria were as follows: chest computed tomography (CT) and ultrasound data; aged between 15 and 70 years; pleural thickening <1.0 cm without calcification; no serious underlying diseases or complications, such as severe diseases of the heart, liver, kidney, or brain, pulmonary cavity, bronchiectasis, bronchial stenosis, or bronchopleural fistula; stage II TE, early stage III TE, and no pulmonary involvement; and underwent decortication by either unitportal or triportal VATS. The exclusion criteria were as follows: aged <15 or >70 years; serious underlying diseases or complications; slow responses to anti-TB treatment; good radiological response to anti-TB treatment; stage III TE with thoracic collapse, intercostal stenosis, or requiring open surgery, TE occupying the entire pleural space, or TE with lung destruction.
All participants had received standard first-line drugs, consisting of isoniazid, rifampicin, ethambutol, and pyrazinamide for 2 months before the operation; and had received the above standard first-line drugs for a further 2 months after surgery, followed by isoniazid, rifampicin, and ethambutol for at least 4 months.
VATS
Before VATS decortication, pleural fluid was removed under local anaesthesia by local blockade of intercostal nerve using a formulation of 100 ml saline, 60 ml sodium bicarbonate, 30 ml ropivacaine, and 1 µg/kg dexmedetomidine.
Uniportal VATS: Patients were positioned in the lateral decubitus position with a forward incline of 30°. All patients were conventionally intubated with a double-lumen endotracheal tube. Under general anaesthesia (induced with 2 mg/kg propofol, 5 µg/kg sufentanil and 2 mg/kg homeopathic atracurium, intravenously [i.v.], and maintained with 0.2 µg/kg/h dexmedetomidine, 2–4 µg/ml propofol by targeted-controlled infusion [TCI], 1–2 ng/ml remifentanil by TCI, and 5 mg/30 min homeopathic atracurium, i.v.), a 4 cm single incision was made in the 7th intercostal space, based on radiological findings. Uniport VATS was then performed to carefully separate the pleural peels from the visceral pleura to free the lungs completely. After decortication, two chest tubes were placed for drainage.
Triportal VATS: Patients were positioned and maintained under general anaesthesia as described above. The incision location varied in accordance with the location of the abscess that required intervention. Normally, the operating hole was located in the 7th intercostal space, and another two holes were created in the 8th intercostal space of the posterior auxiliary line and the subscapular angle line, respectively.
Pain was evaluated at 1, 6, 24, and 48 h following surgery using a Visual Analog Scale (VAS), with possible scores ranging from 0 (no pain) to 10 (severe pain).
After the operation, intravenous morphine was routinely administered within 10 min for both groups as follows: 150 mg morphine in 150 ml normal saline at 1 mg/ml, bolus dose only, 1 mg per bolus, lockout interval. For enhanced recovery, in the early stage (about 3 or 4 h after surgery), the patient was encouraged to ambulate to re-expand the lungs.
Chest tubes for drainage
Two tubes were used for the uniportal group; one tube (28F) was placed in front of the chest cavity, the other (24F) was placed behind the chest cavity, and the two tubes were pushed into the same incision. For the triportal group, two chest tubes were placed in the two holes in the 8th intercostal space, respectively. Due to the use of two tubes, local pleural effusion and a pneumothorax were routinely avoided.
Chest x-ray was performed after 1 day and a thoracic CT scan was performed after 3 days. If there was no air leak or if the pleural effusion in the thoracic cavity was <200 ml, the chest tubes were removed and the patient was considered for discharge. All participants were followed-up in the outpatient department at 7 days and 1 month postoperatively.
Data collection and statistical analyses
Data regarding the following parameters were extracted and assessed: operation time, intraoperative blood loss, postoperative length of bed-rest, chest tube duration, postoperative length of hospital stay; pain scores, rescue analgesia, adverse events during analgesia (such as nausea or vomiting, dizziness, hypotension, pruritus, or bradycardia), and postoperative complications, including persistent air leak (>7 days), post-surgical bleeding in the pleural cavity, wound infection, recurrence that required re-operation, and death.
Data are presented as mean ± SD for continuous variables and n (%) prevalence or incidence for categorical variables, and all data were analysed using SPSS software, version 22.0 (IBM, Armonk, NY, USA). Continuous data were compared between groups using Student’s t-test and categorical data were compared using χ2-test. A P value <0.05 was considered to indicate statistical significance.
Results
A total of 40 patients were included (20 patients in each group). Participant baseline demographics and clinical data were comparable between the two treatment groups (uniportal and triportal groups; Table 1). The maximal diameter of the tuberculous empyema cavity and maximal fibrous pleural thickening were also comparable between the two groups. All procedures were 100% successful, and the lungs were fully expanded in all cases. Operative time, intraoperative blood loss, chest tube duration, postoperative chest tube drainage, and postoperative length of hospital stay were similar between the groups. None of the patients in either group required conversion to other surgical procedures including triport VATS in the uniportal group or thoracotomy in the triportal group (Table 1 and Table 2).
Demographic characteristics of patients with tuberculous empyema who underwent either uniportal decortication or triportal decortication.
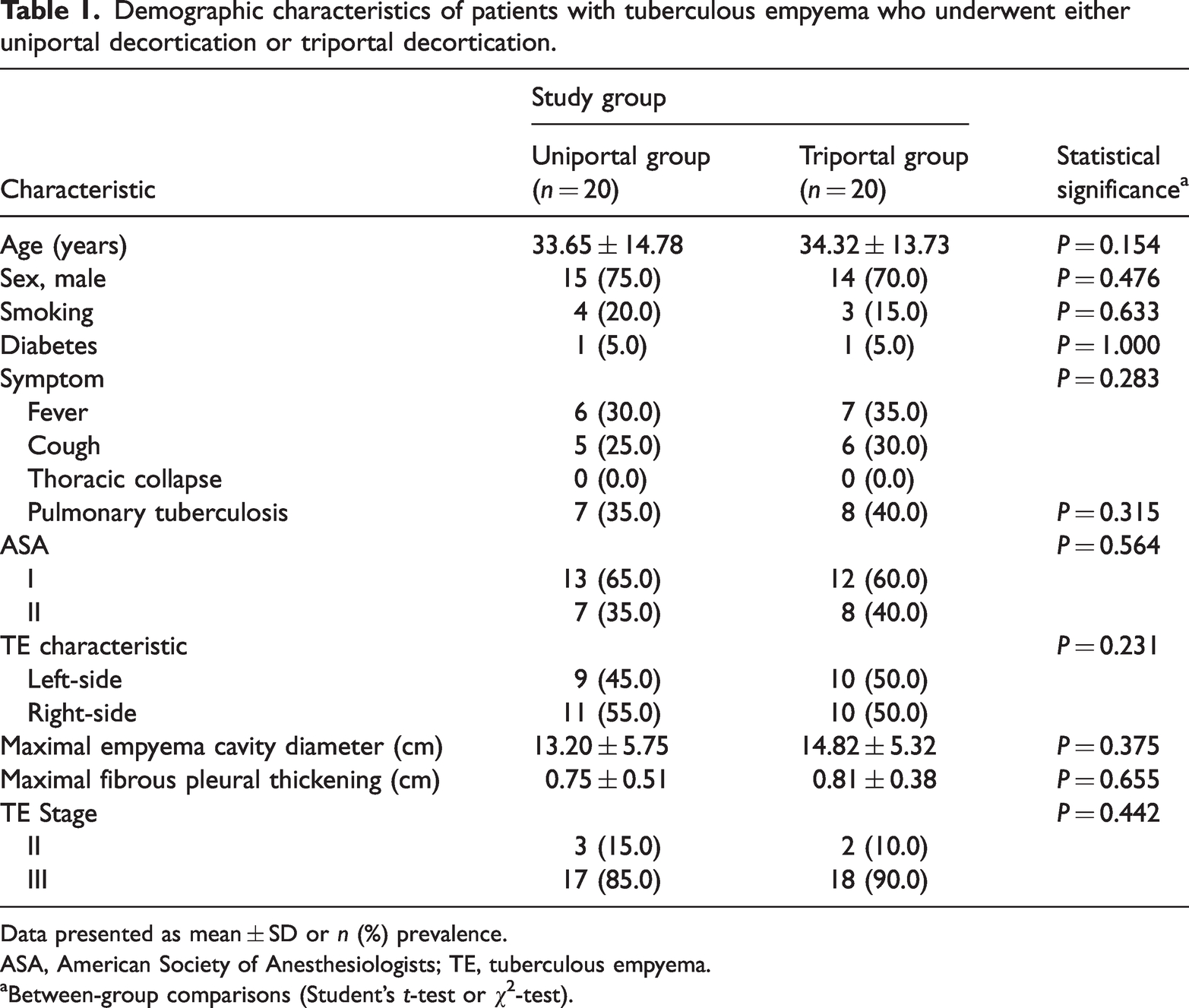
Data presented as mean ± SD or n (%) prevalence.
ASA, American Society of Anesthesiologists; TE, tuberculous empyema.
aBetween-group comparisons (Student’s t-test or χ2-test).
Perioperative data for patients with tuberculous empyema who underwent either uniportal decortication or triportal decortication.

Data presented as mean ± SD or n incidence.
PACU, postanaesthesia care unit.
aBetween-group comparisons (Student’s t-test or χ2-test).
The VAS scores were significantly lower in the uniportal group than in the triportal group at 8 h and 12 h postoperatively (P = 0.005 and P = 0.037, respectively; Table 3), as was postoperative morphine consumption (P = 0.003; Table 2). Furthermore, there was no significant difference between the two groups in terms of the threshold for mechanical withdrawal preoperatively, however, the threshold value was higher in the uniportal group than in the triportal group at 4 h and 8 h postoperatively (P = 0.006 and P = 0.009, respectively; Table 4).
Comparison of pain scores between patients with tuberculous empyema who underwent either uniportal decortication or triportal decortication.

Data presented as mean ± SD.
*P < 0.05 compared with the triportal group (Student’s t-test).
Comparison of perioperative mechanical withdrawal threshold between patients with tuberculous empyema who underwent either uniportal decortication or triportal decortication.

Data presented as mean ± SD.
*P < 0.05 compared with the triportal group (Student’s t-test).
The incidence of postoperative nausea and vomiting was significantly lower in the uniportal group than in the triportal group (P = 0.024; Table 5). A few adverse effects occurred in both groups, specifically, wound infection for one patient in the uniportal group; and wound infection for one patient and recurrence that required re-operation for another patient in the triportal group. There were no deaths in either group.
Incidence of adverse events during the analgesia procedure in patients with tuberculous empyema who underwent either uniportal decortication or triportal decortication.
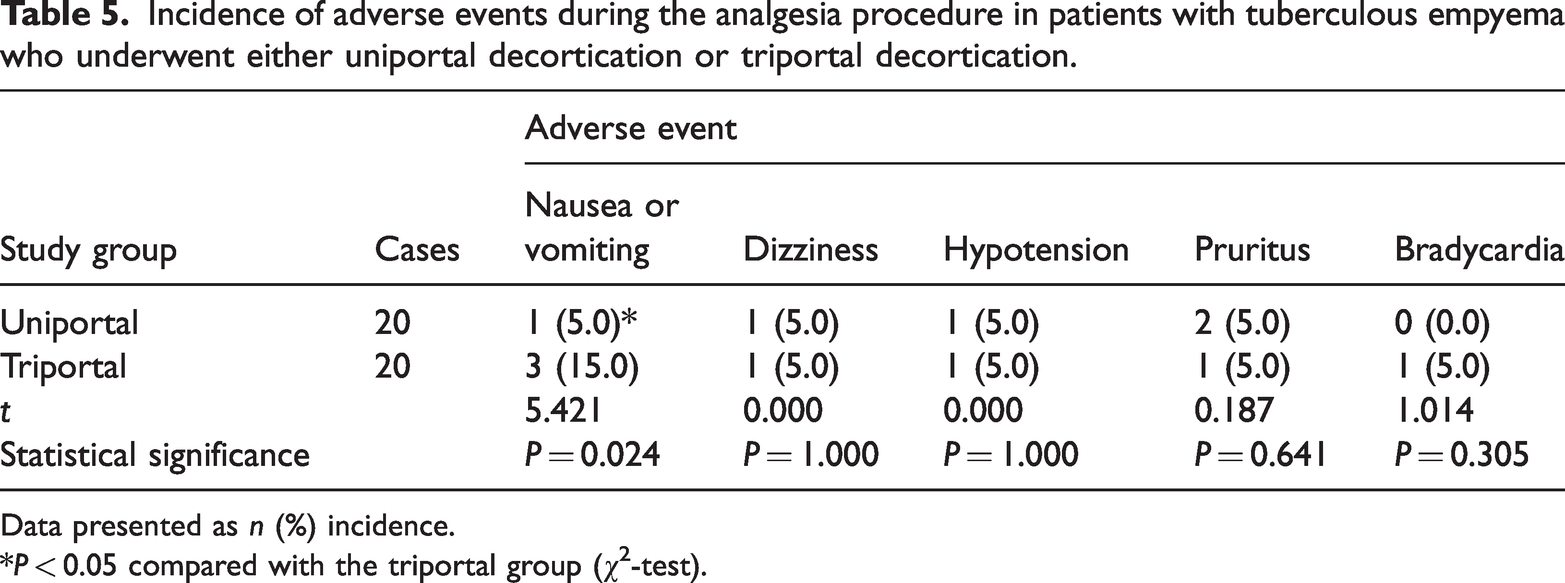
Data presented as n (%) incidence.
*P < 0.05 compared with the triportal group (χ2-test).
Discussion
In the past, open thoracotomy was the only tool for decortication and debridement in the treatment of TE. Open thoracotomy involves the removal of one rib and usually results in significant bleeding and major trauma. 12 VATS has since been introduced for the treatment of TE, and VATS decortication was shown to be safe and effective for stage II and stage III TE in a study conducted at Taizhou Hospital, LinHai, China. 13 Limited data exist on the role of uniport VATS for decortication in the treatment of TE. Therefore, in the present study, the effectiveness and safety of uniportal decortication and debridement were assessed. The present findings showed that uniport VATS decortication was less painful than triport VATS for patients with TE. These findings were consistent with the performance of VATS for other procedures (such as lobectomy and segmentectomy).14,15
Uniport VATS has become increasingly popular within the field of thoracic surgery. First, with improvements in the experience of surgeons and surgical techniques, the indications for uniport VATS have been expanded. Currently, uniport VATS is also indicated in more complex surgical procedures, such as double sleeve lobectomy. 10 Secondly, when uniport VATS is performed, an incision is usually made at the intercostal space. However, a subxiphoid uniportal approach was employed in a recent study as a novel method for insertion. 16 Thirdly, uniport VATS is permitted for most thoracic cancers and has a high priority for simple surgeries (such as resection, pleural biopsy, lobectomy, and segmentectomy). Lung decortication for empyema by uniportal VATS was first performed by Dr Migliore in Italy, during 1998, and studies on the procedure under local anaesthesia and sedation were published in 2001, 2002, and 2003.17–19
Uniport VATS is frequently performed for lung resections at the Third People’s Hospital of Shenzhen. In the authors’ experience, decortication and debridement using uniport VATS for the treatment of TE is an effective procedure, and no patient has required further treatment with conventional VATS or thoracotomy. Unfortunately, uniport VATS has several contraindications, such as a collapsed lung, intercostal stenosis, fibrous pleural thickening, and serious adhesion. Hence, thoracotomy remains a useful tool for patients with TE who display the abovementioned conditions. Compared with the triportal group, uniportal decortication was associated with a similar level of surgical procedure-related complications in the current study, with no incidences of cardiac or aortic injury, or massive haemorrhage.
In terms of decortication and debridement for TE treatment, several studies have demonstrated that VATS is superior to thoracotomy regarding outcomes, such as blood loss, length of hospital stay, VAS score, recurrence, and other complications.5,20 Because only one intercostal incision is needed for the insertion, uniport VATS is considered a less invasive procedure that may significantly improve the life quality of TE patients. A previous study revealed that complete debridement and decortication were achieved for all patients with purulent empyema through a uniport VATS approach. 21 No conversion or further access was needed for any reason, and no major complication was recorded. Therefore, uniport VATS performed by an expert surgeon was concluded to be a safe and effective option for the treatment of stage II and stage III purulent empyema. 21 As the role of uniport VATS in the treatment of TE remains unclear, the current retrospective study was conducted to assess the performance of uniport VATS compared with triportal decortication in TE. In this study, no significant differences were observed between the two procedures in the treatment of patients with stage II TE and early stage III TE. Several clinical characteristics reflecting the safety and efficiency of uniport VATS were assessed, such as VAS score, postoperative length of hospital stay, postoperative length of bed rest, and other postoperative complications. The data were consistent with previous reports, and indicated that, compared with triport VATS, uniport VATS may be considered a safe and effective option in the treatment of TE.
Based on the present authors’ experience, uniport VATS has several advantages over traditional three-port VATS and thoracotomy, such as less pain, decreased physiological trauma, and better cosmesis. First, an incision is usually made through the 7th intercostal space at the posterior axillary line, which enables easy access to the pus cavity and facilitates the surgical procedure, with effective results. Secondly, uniport VATS may be helpful in alleviating injury to the lungs and may improve the lung function. We propose that when a high level of expertise is achieved, uniport VATS should be considered as the first choice for the treatment of patients with stages II and III TE.
Although some interesting findings were obtained, the present study has certain limitations, such as the retrospective study design and the small sample size. A prospective, randomized and controlled trial, with a larger sample size is necessary to confirm the role of uniport VATS for selected patients with stages II and III TE.
In conclusion, uniport VATS decortication may be a safe and feasible therapeutic option for patients with stages II and III TE.
Footnotes
Author contributions
Zhaohua Xia contributed to the study design; Shuo Zheng, Qinlang Shi, Haijiang Wang, Xinzhong Ning, and Pilai Huang participated in data collection; Guohuan Wen and Ning Xiang participated in data analysis and supervision; Mingfeng Liao and Mingfei Ma participated in the drafting of this manuscript; and Kun Qiao revised the manuscript.
Data availability statement
Data that support the findings of this study are available on request from the corresponding author.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the Natural Science Foundation of China (31500727), the Science and Technology Project of Shenzhen (JCYJ20150402111430624), the Shenzhen Municipal Health and Family Planning Commission (201501030), and the Chen Jingyu team of the Sanming Project of Medicine in Shenzhen (SZSM201812058).