
Abstract
This paper presents a clinical case study investigating the pattern of a saxophonist’s embouchure as a possible origin of orofacial pain. The rehabilitation addressed the dental occlusion and a fracture in a metal ceramic bridge. To evaluate the undesirable loads on the upper teeth, two piezoresistive sensors were placed between the central incisors and the mouthpiece during the embouchure. A newly fixed metal ceramic prosthesis was placed from teeth 13 to 25, and two implants were placed in the premolar zone corresponding to teeth 14 and 15. After the oral rehabilitation, the embouchure force measurements showed that higher stability was promoted by the newly fixed metal-ceramic prosthesis. The musician executed a more symmetric loading of the central incisors (teeth 11 and 21). The functional demands of the saxophone player and consequent application of excessive pressure can significantly influence and modify the metal-ceramic position on the anterior zone teeth 21/22. The contribution of engineering (i.e., monitoring the applied forces on the musician’s dental structures) was therefore crucial for the correct assessment and design of the treatment plan.
Introduction
The orofacial complex is the primary link between the instrument and the musician’s embouchure. The embouchure is a common term used among saxophonists to denote the combination of orofacial structures, such as the lower lip and the upper maxillary dentition, that contact the mouthpiece at the saxophone tip. 1 Previously published studies have focused on the complex neuromuscular patterns involved in the embouchure to elucidate the mouthpiece forces, tooth displacement, and eventual effects on the dental occlusion of wind instrumentists.2–4 The extensive practice required to master the complex physical activities of the embouchure can involve study hours that range from 25 hours per week during adolescence to as much as 50 hours per week during adulthood.
In this clinical study, we investigated the pattern of a saxophonist’s embouchure to determine the extent to which it may have been related to the musician’s orofacial pain, subsequent modifications in the dental occlusion, and fracture of the metal ceramic bridge. A rehabilitation procedure was necessary to maintain both the esthetic and functional aspects of the saxophonist’s occlusion. The aim of this article was to describe a new dentistry approach for such patients, focusing on aesthetics without disregarding the fundamental aspects of the forces that are transmitted to the teeth by the mouthpiece during the embouchure and musical performance.
Case Report
The patient was a white male saxophone player in his early 60s who had more than 40 years of experience playing saxophone. He presented orofacial pain and underwent a clinical examination in the orofacial region, including a panoramic X-ray (Figure 1). The patient localized the orofacial pain to the anterior zone of the upper jaw, where a dental prosthetic was present on tooth 21. He had been involved in a car accident at the age of 18 years, necessitating rehabilitation with a prosthetic device (Figure 2) and root canal procedures. He underwent an apicectomy of tooth 21 several years later because of pain in that area. At his first appointment in the clinic, we observed a fracture of the metal ceramic bridge between teeth 13 and 12. The reporting of this study conforms to the CARE guidelines. 5

Panoramic X-ray.

(a) Intraoral view of the saxophonist player’s occlusion. (b) Intraoral right view and (c) Left view showing the fracture of the existing bridge between teeth 12 and 13.
During the embouchure examination, the musician played Orchestral Suite No. 1 by Bach (Figure 3), which he had been rehearsing for his next concert. Embouchure force measurement was accomplished by the placement of two piezoresistive force sensors (FlexiForce A201, 111 N; Tekscan, Norwood, MA, USA) on the upper part of the mouthpiece where the central incisors stabilize the embouchure. The sensors allowed quantification of the forces between the mouthpiece and the existing oral rehabilitation (Figure 4).
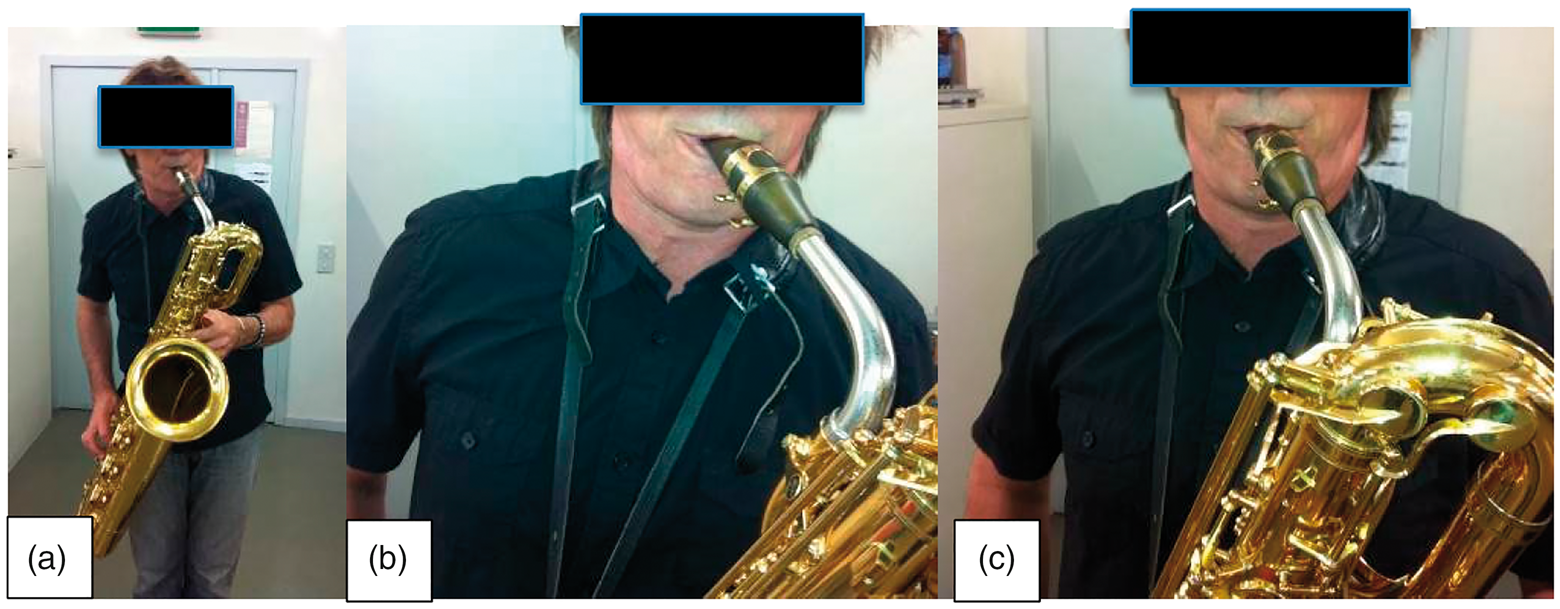
(a) Saxophonist playing the baritone. (b) Musician’s embouchure with mouthpiece deviated from the normal position and (c) Mouthpiece with a slightly more centered embouchure.
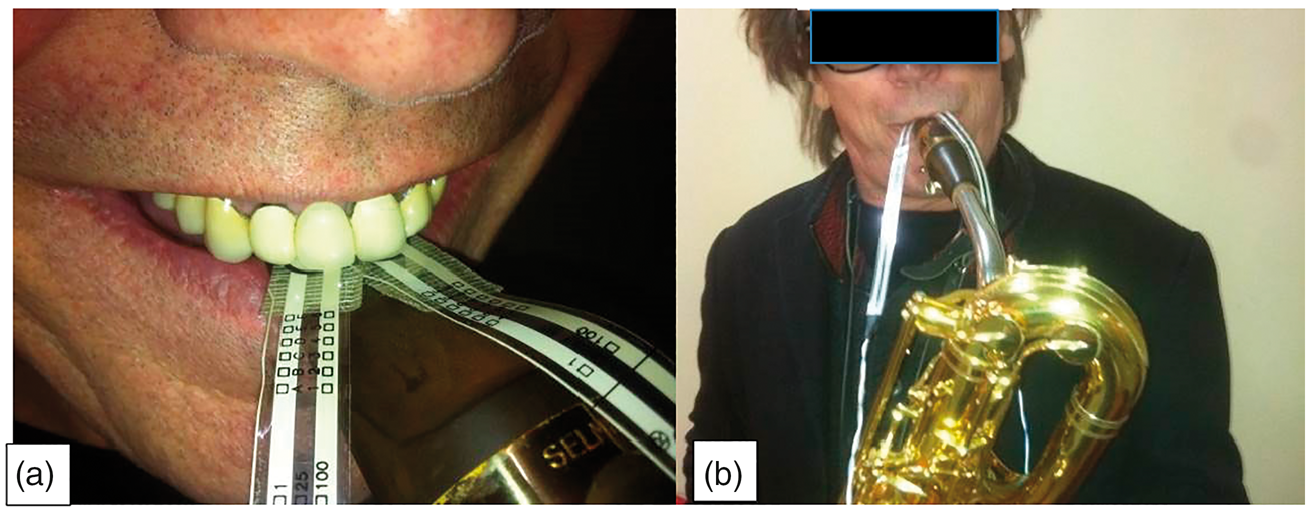
(a) Sensors applied to saxophonist’s mouthpiece and (b) Measurement of forces during musical performance.
Dental impressions of the maxillary and mandibular jaws were made to create dental casts. The oral rehabilitation plan for the saxophone player involved removal of the broken bridge from the premolar zone of the first quadrant by leaving the crown on tooth 16 and cutting its mesial zone with a bur. Because the fracture was in the mesial zone of tooth 13, the metallic ceramic bridge was removed. Two implants were placed in the premolar zone, corresponding to teeth 15 and 14 (Figure 5(a), (b)). The anterior teeth were prepared and a provisional acrylic bridge was made with a special reinforcement to sustain the saxophonist’s pressure during his performance. These provisional teeth were applied because the surgical implant procedure was carried out in two steps. The crowns were placed over the implants 4 to 5 months after the surgery. The patient provided written consent for this treatment in advance; he also gave his written permission to publish his clinical case. The requirement for ethics committee approval was waived because the treatment was performed at a private clinic.

(a) Panoramic X-ray after implant surgery and (b) Lateral cephalogram with saxophone player’s embouchure.
The final prosthodontic procedure was performed with consideration of the anatomy of the incisal edge from the previous crowns. Special attention was paid to the aesthetics and function of the oral rehabilitation, with particular care to the inclination of the incisal edge of the central incisor crowns because this is a crucial point for the “grip” of the musician’s embouchure (Figure 6(a)–(c)).

(a) Lateral view of prosthetic treatment with crowns over implants correspondent to teeth 15 and 14. (b) Final metal ceramic fixed dental prostheses from teeth 13 to 25 and (c) Panoramic X-ray 2 years after treatment.
Because the intraoral examination at the first appointment revealed misaligned central incisors in the maxillary arch; gingival recession at the canines, lateral incisors, and central incisor 21; pronounced overjet; and tooth wear, an occlusal splint (night mouthguard) was applied after the oral rehabilitation to stabilize and maintain the effects of the dental procedures (Figure 7(a)–(c)). The design and fabrication of this splint was in accordance with our evaluation of the eventual technical and biological complications secondary to the patient’s bruxism pattern. With the implementation of this device, we also attempted to promote an occlusal adjustment attaining equal intercuspal positions, equilibrium of the masticatory system by reducing muscle hyperactivity, and protection of the temporomandibular joint against undesirable loads. The new dynamic embouchure force was measured to establish the relationship of the forces transmitted by the mouthpiece after the dental treatment. The saxophone player was asked to perform low, middle and high notes three times in a row to compare the force distribution with the new oral rehabilitation.

Intraoral views after adjustment of occlusal splint. (a) Right view. (b) Front view and (c) Left view.
Results
The embouchure force measurements made before the oral rehabilitation showed that the saxophone player exerted more pressure on the crown of tooth 21 than on the crown correspondent to tooth 11. This occurred during the playing of all notes (high, medium, and low). There was minimal loading of the saxophone mouthpiece in the first quadrant; the embouchure was mainly directed to the left maxillary arch. When playing a high note, the force produced by the fixed prosthodontic device of the metal-ceramic crown of tooth 21 reached 1.86 N (0.19 kgf), while the crown correspondent to tooth 11 reached 0.637 N (0.065 kgf). The medium pitch exerted a force of about 1.27 N (0.13 kgf) on tooth 21, while tooth 11 maintained a lower load of 0.637 N (0.065 kgf). The low note produced less force on the mouthpiece (0.98–1.08 N (0.10–0.11 kgf) on tooth 21) (Figure 8).

Saxophone embouchure’s forces.
By contrast, after the dental treatment and placement of the newly fixed metal-ceramic bridge, there was an even distribution of pressure on the anterior zone correspondent to crowns 11 and 21 (Figure 9(a), (b)). The high tone reached 3.92 N (0.40 kgf) on tooth 11 and 2.94 N (0.30 kgf) on tooth 21. These measurements revealed exactly the opposite situation than before the oral rehabilitation. That is, after the prosthodontic treatment, the saxophone player achieved more stability of his embouchure while playing high and middle notes, allowing him to sustain higher loads on the right upper incisor than the left central incisor. An equilibrium of the force distribution was thus attained between the two central incisors, eventually allowing a more “centered” embouchure. The clinical effectiveness of the oral rehabilitation is notable with respect to maintenance of the mouthpiece at a new position with objective improvement of the contact area of the metal-ceramic fixed bridge. Significant changes were observed at low tones, during which tooth 11 could support a force of 3.43 to 4.9 N (0.35–0.50 kgf) (in contrast to tooth 21 at just 1.76 N (0.18 kgf)).

Saxophone embouchure’s forces after oral rehabilitation.
Discussion
This study revealed the importance of the load distribution from the mouthpiece to the dental structures and provided a more complete understanding of the physical properties associated with the embouchure. This in vivo investigation demonstrates the correct approach to combining the history and physical examination findings of the orofacial structure of a saxophone player to obtain an optimal treatment outcome.
Previously published studies have focused on measuring the mouthpiece forces during brass instrument playing. Borchers et al. 6 found that the peak force was 29 N (2.96 kgf) for tuba playing with minimal tooth deflection (43 µm) compared with the peak force of about 50 N (5.10 kgf) for trumpet playing with horizontal deflection of up to 100 µm on the central incisors (teeth 11 and 21). Rindisbacher et al. 7 found that playing wind instruments had no or only a minor influence on the face or dentition.
The results of this study allow confirmation of the relationship of an “ideal” embouchure. We found that during saxophone playing, the forces applied by the musician’s upper teeth on the mouthpiece can exceed the standard light, continuous forces of fixed orthodontic treatment (2.45–4.90 N (0.25–0.50 kgf)). Fortunately, the forces applied by a single-reed instrument player are discontinuous forces during the “flexible” embouchure and performance.
The functional demands of the saxophone player and consequent application of excessive forces can significantly influence and modify the metal-ceramic position on the anterior zone (teeth 21/22). The embouchure force measurements after oral rehabilitation showed that higher stability was promoted by the newly fixed metal-ceramic prosthesis, thus highlighting four important findings. First, before the oral rehabilitation, there was a significant difference in the embouchure force measurements on tooth 21 compared with tooth 11. Second, the anterior open bite of the metal-ceramic bridge was associated to the existing disequilibrium of the embouchure pressure. Third, the new oral rehabilitation was based on the knowledge previously acquired by the sensors to design a more stable structure of the new metal-ceramic bridge. Fourth, after the dental treatment, more symmetric loading of the central incisors was achieved.
Liebman 3 reported that the high register often reclaims greater freedom in the embouchure and a larger reed vibration area. By contrast, the low register tends to be better activated by tighter pressure and a smaller reed vibration area. The methodologic analysis of our results revealed a correlation with the findings reported by Liebman 3 with respect to the fact that 2 years after rehabilitation, higher pressure was exerted on tooth 11 while playing a low note. While increasing the range pitch to a higher note, our patient achieved greater freedom in the embouchure and moved his mouthpiece slightly toward the left side of the maxilla with higher pressure on tooth 21. Analysis of these micro-movements during the embouchure/playing of a wind instrument is only possible with appropriate protocols and implementation of sensor devices. 8 , 9 FlexiForce piezoresistive sensors can be used to evaluate and measure the existing differences in the embouchure mechanism between woodwind instruments and brass instruments, specifically elucidating the differences in labial pressure and tooth pressure. 10 Clemente et al. 11 , 12 studied the inter-relationship of the craniofacial morphology and tooth position in wind instrument players with cephalometric analysis to compare the anatomical characteristics or landmarks that could eventually be altered by musical performance. These results have high significance in dentistry and performing arts medicine with direct implications for clinical practice because heavy forces applied to certain structures of the stomatognathic system can be particularly harmful.
This system was revealed to be appropriate for the development of a treatment plan. Further studies are needed to measure the embouchure forces in players of woodwind instruments and brass instruments and determine whether there are differences in labial pressure and tooth pressure. These issues can be of major importance when dealing with aesthetic dentistry procedures of wind instrument players.
Notably, the saxophone player in the present case had many years of experience in musical performance and had certain specificities that characterized his embouchure (insertion of the mouthpiece inside the oral cavity and use of the orofacial muscles). Therefore, regular clinical evaluation of teeth 21 and 22 must be continued because the eventual disequilibrium of forces applied to these teeth while playing the saxophone may result in recurrence of the initial symptoms. If this occurs, another apicectomy can be part of the future treatment plan.
The implementation of technologies that can contribute to the quantification and understanding of undesired forces applied to the oromaxillomandibular area in patients with orofacial pain can be one of the main goals of dentistry. Although the sensors used for this purpose are flexible and the thinnest available on the market (0.203 mm), this may present a limitation regarding the adaption of wind instrumentalists. With this in mind, we found that it was possible to achieve a correct diagnosis and predict a better outcome of the oral rehabilitation in this particular case.
Conclusions
Orofacial pain can cause limitations from a functional point of view, considering that the main functions of the masticatory system include mastication and, in this particular case, saxophone playing. The embouchure mechanism executed by this wind instrumentalist for more than 40 years was likely associated with the development of malocclusion involving proclination of the upper left incisors. The asymmetrical forces applied to the anterior zone by the mouthpiece, which were quantified by the piezoresistive sensors, were in accordance with the proclined anterior teeth.
The introduction of piezoresistive sensors is an important landmark in oral rehabilitation, especially for wind instrument players, because these sensors have made it possible to monitor the forces induced on the upper teeth before and after dental treatment.
With the new prosthodontic treatment in the present case, the embouchure mechanism allowed a more harmonious distribution of forces on the upper teeth. The pressures measured where more symmetrical, resolving the orofacial pain because the pressure of the mouthpiece was not being exerted at one singular point. The use of piezoresistive sensors is easily replicated in the clinical environment when a wind instrument player requires an oral rehabilitation.
Footnotes
Authors’ contributions
Conceptualization, M.P.C.; data analysis, J.M. and H.V.T.; original draft preparation, M.P.C. and G.B.; final text version to be published, J.M.A., A.P.F., and J.M. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by FCT, under LAETA projects UIDB/50022/2020 and UIDP/50022/2020.