
Abstract
Certain drugs can cause kidney stones but as far as we are aware, ceftazidime-related urinary calculi have not been previously reported. We report here a case of an 8-year-old boy who developed hydronephrosis secondary to urinary calculi after receiving ceftazidime 2.0 g by intravenous infusion daily for two weeks. Previously, his left kidney showed no signs of disease. A retrograde double J ureteral stent was inserted, ceftazidime terminated, fluids increased and urine alkalised. On day 25, the patient showed no signs of kidney stones or hydronephrosis. Clinicians should be aware of the possibility of ceftazidime-related urinary calculi particularly if patients are receiving long-term treatment.
Introduction
Ceftazidime is a third-generation cephalosporin antibiotic and is commonly used in clinical practice. 1 The drug has broad spectrum antimicrobial coverage, a long half-life, is generally well tolerated and is on the World Health Organization (WHO) list of essential medicines 1,2 We report a case of a young boy who developed severe hydronephrosis secondary to urinary calculi following treatment with ceftazidime.
Case report
An 8-year-old boy presented to our hospital with severe hydronephrosis in his right kidney. A day before admission, the patient experienced right lower back pain accompanied by nausea, vomiting, fever, polyuria, dysuria and haematuria. Ultrasound examination of the right kidney showed severe hydronephrosis and magnetic resonance imaging (MRI) showed severe hydrops. There were no obvious abnormalities in the patient’s left kidney (Figure 1). Before this event, the patient had been physically healthy and had no prior history of high blood pressure, diabetes, immunodeficiency or recent foreign travel

Magnetic resonance imaging (MRI) scan of the patient on admission. The solid arrow indicates the severe hydrops in the right kidney. No abnormalities were observed in the left kidney.
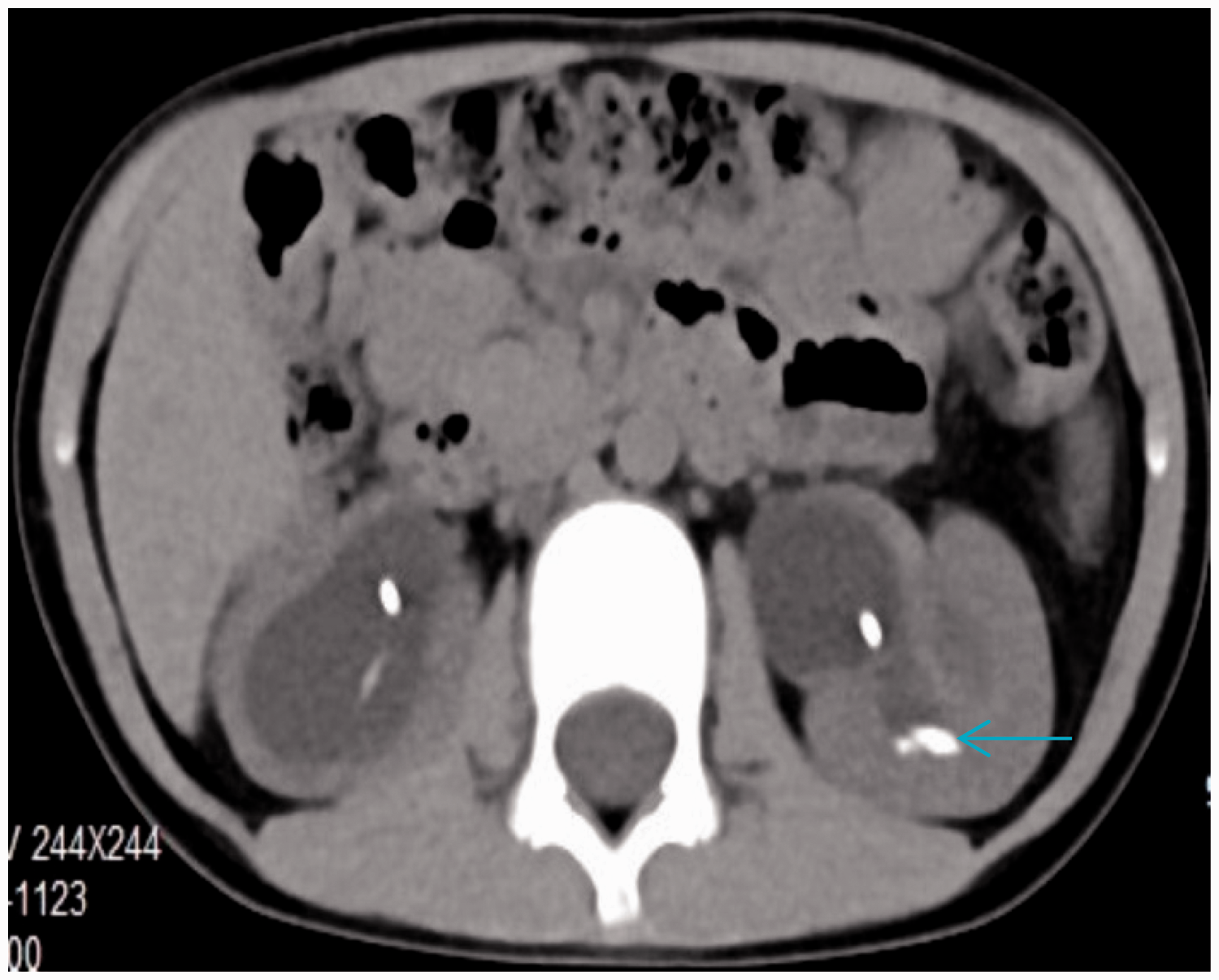
Initially, the patient was thought to have ureteropelvic junction stenosis and so transperitoneal pyeloplasty using the Anderson-Hynes technique was performed. 3 During the laparoscopy it was confirmed that there was right ureteropelvic junction obstruction. Post-surgery, the patient was prescribed a daily intravenous infusion of ceftazidime 2.0 g for two weeks. At the end of this period, a computed tomography (CT) scan of the lower abdomen and pelvis showed that the hydronephrosis of the right kidney had significantly reduced and the ureteral stent was in a good position. However, the previous healthy left kidney showed some high-density shadows in both the ureter and kidney, and hydronephrosis had developed (Figures 2 and 3).

A computed tomography scan (CT) of the patient two weeks after receiving ceftazidime 2.0 g by intravenous infusion daily. The arrows indicate the hydronephrosis and the high-density shadow that had developed in the left kidney.

A computed tomography scan (CT) of the patient two weeks after receiving ceftazidime 2.0 g by intravenous infusion daily. The arrow indicates the high-density shadow in the left ureter.
A retrograde double J ureteral stent was inserted on the left side and intravenous ceftazidime was terminated. The patient’s liquid intake was increased and he was given potassium sodium hydrogen citrate granules to alkalise his urine. Six days later, a CT scan showed that the left ureteral stones had decreased in size and had returned to the renal pelvis and the hydronephrosis had reduced significantly (Figure 4).
A computed tomography (CT) scan of the patient six days after a retrograde double J ureteral stent was inserted, ceftazidime terminated, fluids increased and urine alkalised. The arrow indicates that the left ureteral stones had decreased in size and had returned to the renal pelvis and hydronephrosis had significantly reduced.
Twenty-five days after the left kidney catheterization, a subsequent CT scan showed that the kidney stones and hydronephrosis had disappeared completely and so the stent was removed (Figure 5). Six months after the operation, a CT scan showed no signs of kidney stones or hydronephrosis in the left kidney.

A computed tomography (CT) scan of the patient 25 days after surgery. The arrow indicates that the left kidney stones and hydronephrosis had disappeared completely.
This case report did not require ethics committee approval. Written authorisation was obtained from the patient's family before publication of this article.
Discussion
Drug-related calculi account for approximately 1–2% of all kidney stones. 4 Although the exact mechanisms of drug-induced calculi are unknown, two main hypotheses have been suggested; one relates to solubility of the drug (i.e., low solubility results in high urine concentration which leads to crystal formation in the urinary tract) and the other to metabolic effects of the drug which induce calculi formation.4,5
Although there have been several reports suggesting cephalosporins have the potential to induce urolithiasis,6–11 as far as we are aware there have been no previous reports of ceftazidime-related urinary calculi. Our patient had no left kidney ureteral calculi or hydronephrosis on admission and with the exception of intravenous infusion of 500 ml 0.5% glucose on the day after surgery, ceftazidime was the only drug given to the patient. Therefore, we suggest that the formation of the urinary calculi in this patient was linked to ceftazidime.
On discovering the left urinary calculi and hydronephrosis we placed a ureteral stent which enabled urinary drainage, avoided aggravation of renal hydronephrosis and improved renal function. In addition, the patient’s fluid intake was increased and his urine was alkalised. The left urinary calculi gradually dissolved and on the 25th day after surgery, the stones and secondary hydronephrosis had disappeared. At the six-month follow-up, the patient showed no signs of urinary calculi or hydronephrosis.
Our case study suggests that clinicians should consider the possibility of ceftazidime-related urinary calculi when a patient who is receiving the antibiotic presents with symptoms of low back pain or abnormal kidney function. For management, we suggest insertion of a retrograde double J ureteral stent followed by increased fluid intake and urinary alkalinisation.