
Abstract
Objective
To investigate if the implementation of enhanced recovery after surgery (ERAS) pathways could be effective in paediatric patients undergoing appendectomy.
Methods
This retrospective study analysed the data from patients aged ≤18 years that underwent appendectomies. The data collected included age, sex, application of enhanced recovery concepts (ERCs) and clinical outcomes.
Results
A total of 93 paediatric patients were retrospectively categorized into two groups: patients in group 1 did not experience the use of ERCs during their appendectomies; and patients in group 2 had ERCs applied during their appendectomies. Patients in both groups were exposed to some elements of ERAS, including preoperative patient/parent counselling, limited fasting durations, antibiotic prophylaxis and no bowel preparations. Duration of hospital stay was significantly longer in group 1 compared with group 2 (3.47 ± 1.81 days versus 2.24 ± 1.52 days, respectively. There were no significant differences between the two groups in term of postoperative pain control, hospital cost, readmissions, reoperations and emergency room visits.
Conclusion
Implementing ERCs in paediatric patients undergoing appendectomies provided a significant improvement in patient recovery with a shorter hospital stay, with no increase in postoperative pain, hospital cost, rate of readmission and reoperation.
Keywords
Introduction
Recovery after surgery is difficult for anyone who has undergone surgery, but there are variations depending upon the type of surgery undertaken, the patient's condition, their age, anaesthesia type, operation duration, whether it is an outpatient or inpatient procedure, and many other factors as well.1,2 When it comes to paediatric patients, they may be overwhelmed by new sights or sounds and may not always understand or even know how to express their concerns and their uncomfortable feelings. Therefore, more attention is required to enhance their surgical recovery. Several studies have been conducted in different regions of the world to help children cope better with surgical stress and ease their discomfort.3–7 Enhanced recovery after surgery (ERAS) protocols and guidelines have also been implemented.3–6 Studies have demonstrated that fast-track protocols can be applied safely in paediatric patients undergoing routine gastrointestinal (GI) paediatric surgery.3–5
An enhanced recovery approach is a multimodal preoperative, intraoperative and postoperative healthcare programme that incorporates evidence-based best practices including protocols and guidelines intending to provide standardized care for patients and increase their satisfaction. It was first described by the Danish surgeon Henrik Kehlet in the 1990 s to reduce the perioperative stress response and organ dysfunction in surgical patients. 8 The use of ERAS protocols in adult surgeries in previous studies has provided a good basis for pathway design and some supporting data to encourage the development of paediatrics-specific guidelines,9,10 which have been used in subsequent paediatric studies with a focus on the importance of having specific data for paediatric ERAS pathways effects.6,7 Similarly, a series of evidence-based care elements for paediatrics were evaluated in multiple regions for different types of GI surgeries, including appendectomies, with significantly positive outcomes represented by shorter hospital stays and fewer postoperative complications.4,7 Research in paediatric patients has supported the use of minimal preoperative fasting, early initiation of enteral nutrition, and the avoidance of routine lines and drains, in order to improve patient comfort, shorten the duration of postoperative hospital stay, reduce hospital costs and accelerate postoperative recovery without increasing the incidence of postoperative complications.3,7,11
In Jordan, ERAS protocols are not routinely used for paediatric patients. This current retrospective cohort study was undertaken to investigate if the implementation of ERAS pathways could be effective in paediatric patients undergoing appendectomy.
Patients and methods
Study design
This retrospective cohort study enrolled consecutive paediatric patients that underwent appendectomy at the Department of General Surgery, Division of Paediatric Surgery, School of Medicine, The University of Jordan, Amman, Jordan between January 2017 and December 2018. The inclusion criteria were as follows: (i) patients aged between 6 months and 18 years; (ii) patients that underwent appendectomy. Surgeries were conducted by the same team and patients were retrospectively categorized into two groups; patients in group 1 did not experience the use of enhanced recovery concepts (ERCs) during their appendectomies; and patients in group 2 had ERCs applied during their appendectomies. The ERAS protocols were adapted from the adult guidelines as there is a lack of sufficient data or guidelines on paediatric protocols for enhanced recovery. The use of these protocols was supported by their successful implementation in paediatric patients undergoing GI surgeries described in previous studies.3–7
The study was approved by the Institutional Review Board of the University of Jordan, Amman, Jordan (no. IRB: 67/2019/6216). All procedures were undertaken following the ethical standards of the institutional ethics committee and the 1964 Helsinki declaration as well as its later amendments. All applicable international, national and/or institutional guidelines for the care of patients were followed. Written informed consent was obtained from all the parents and/or legal guardians of the study participants. The data from each patient were obtained from the hospital medical records and consents were signed by the parents of the patients on the day of the operation. All personal details were deidentified. The reporting of this study conforms to STROBE guidelines. 12
ERAS protocol
The ERAS protocols were divided into three stages (Table 1): (i) preoperative protocols that consisted of preoperative patient counselling, the non-use of bowel preparation, using antibiotic prophylaxis and reducing the preoperative fasting periods (maximum fasting duration was 6 h); (ii) intraoperative protocols that included using minimally invasive techniques in those whose conditions allowed for this and the non-use of surgical drains and tubes; and (iii) postoperative protocols such as the early introduction of oral nutrition and early mobilization.
The enhanced recovery concepts used in a retrospective cohort study undertaken to investigate how the implementation of enhanced recovery after surgery pathways could be effective in paediatric patients undergoing appendectomy.

Study outcomes
The primary outcomes were: length of postoperative hospital stay; hospital expenses; postoperative complications that were associated with the implementation of the ERAS protocols as measured by emergency room (ER) visits within 30 days of the operation, readmission and reoperations. Pain after surgery was recorded using a numerical scale out of 10 (where 10 was the maximum level of pain). How well the pain was controlled was recorded using a numerical scale out of 10 (where 10 was indicative of complete pain control). The patients were discharged when they were in a good general condition, pain was controlled, complete oral nutrition, normal micturition and bowel motion were established.
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, NY, USA). Patient data were entered into a spreadsheet. Descriptive statistics obtained included the mean ± SD and frequencies for each variable measured. Wilcoxon–Mann–Whitney test was used to correlate the relationship between ERCs and patient cost of stay. Fisher's exact test was used to correlate the relationship between ERCs and reoperations, readmission and ER visits. Independent samples t-test was used to analyse the impact of ERCs on pain after surgery, pain control and duration of hospital stay. A P-value < 0.05 was considered statistically significant.
Results
Data were collected from 93 patients. Of these, 38 patients did not experience the use of ERCs during their appendectomies (group 1); and 55 patients had ERCs applied during their appendectomies (group 2). Demographic and clinical data are presented in Table 2. Age, sex distribution, comorbidities and a history of previous surgeries were all comparable between the two groups.
Demographic and clinical characteristics of patients included in a retrospective cohort study undertaken to investigate how the implementation of enhanced recovery after surgery pathways could be effective in paediatric patients undergoing appendectomy.
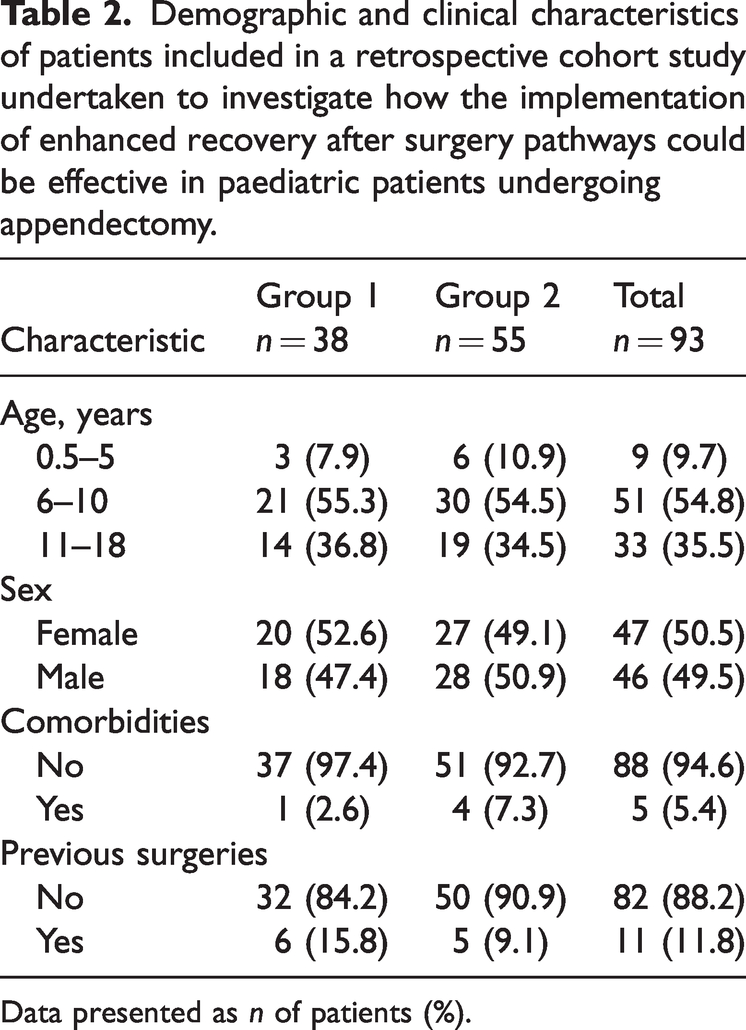
Data presented as n of patients (%).
Patients in both study groups were exposed to some elements of ERAS, including preoperative patient/parent counselling, limited fasting durations, antibiotic prophylaxis and no bowel preparations. All patients in the study underwent appendectomy under general anaesthesia and none of them required a nasogastric tube or a Foley catheter to be kept in place postoperatively. All patients received the same postoperative pain assessment and control. Surgical drains were freely used in group 1, but were only used when there was extreme need in group 2 (Table 3). All patients in group 2 underwent a minimally invasive technique (laparoscopic appendectomy), while all of group 1 underwent open appendectomies. All patients in group 2 had no postoperative restrictions to start oral nutrition, of whom 80% (44 of 55 patients) started feeding within the first 24 h compared with 55% (21 of 38 patients) in group 1.
Implementation of enhanced recovery concepts in patients included in a retrospective cohort study undertaken to investigate how the implementation of enhanced recovery after surgery pathways could be effective in paediatric patients undergoing appendectomy.

Data presented as n of patients (%).
The majority of patients in both groups had hospital costs in the range of 400–1500 Jordanian dinars (1 JOD = 1.41 USD) and there was no significant difference between the two groups (Wilcoxon–Mann–Whitney test) (Table 4). There were no significant differences between the two groups in terms of reoperations within 90 days, readmissions within 30 days and ER visits (Fisher's exact test), which were all low in both groups. There were no significant differences between the two groups in terms of pain score after surgery and level of pain control between the two groups (independent-samples t-test). Patients in both groups had low pain scores with good pain control postoperatively. Duration of hospital stay was significantly longer in group 1 compared with group 2 (3.47 ± 1.81 days versus 2.24 ±1.52 days, respectively; between-group difference, 1.23 [95% confidence interval, 0.5, 1.93]; t(91) = 3.572; P = 0.001.
Outcomes of enhanced recovery concepts in patients included in a retrospective cohort study undertaken to investigate how the implementation of enhanced recovery after surgery pathways could be effective in paediatric patients undergoing appendectomy.

Data presented as n of patients (%) or mean ± SD.
aBetween-group comparisons: *Wilcoxon–Mann–Whitney test; **Fisher's exact test; †Independent samples t-test; NS, no significant between-group difference (P ≥ 0.05).
JOD, Jordanian dinar.
Discussion
The current study retrospectively reviewed the data from 93 paediatric patients aged from 6 months up to 18 years that underwent appendectomies between January 2017 and December 2018. This current study investigated the relationship between some ERAS protocols and important indicators of their benefit during appendectomies. These indicators were chosen according to the results of previous studies conducted in different parts of the world.3–7
In order to investigate differences in the ERCs implemented, the patient cohort was stratified according to the type of surgery that they experienced: group 1 underwent open appendectomies and group 2 underwent a minimally invasive technique (laparoscopic appendectomy). Paediatric patients that underwent laparoscopic surgery (group 2) were discharged significantly earlier compared with patients that underwent open surgery (group 1) (P = 0.001), a finding that was supported by the results of an Italian study that recorded a decrease in postoperative stay in laparoscopic appendectomy patients compared with open appendectomy patients. 9
The majority of patients (51 of 55 patients; 92.7%) in group 2 did not have drains fitted, which might have contributed to their earlier discharge from hospital. A recent study in the US that investigated both open and laparoscopic surgery for inflammatory bowel disease surgery demonstrated that the application of multiple ERAS principles including the avoidance of routine postoperative drains lead to a benefit of decreased mean hospital stay duration by 80 h, but this reduction was not statistically significant. 6 However, an Egyptian study that compared the results of implementing enhanced recovery involving no routine drains after GI resection and anastomosis surgeries versus the traditional methods, reported a significantly shorter postoperative hospital stay in the enhanced recovery group. 13
The majority of patients (44 of 55 patients; 80.0%) in group 2 had their first oral intake of nutrition within the first 24 h, which might have contributed to their earlier discharge from hospital. These findings were similar to a previous study that demonstrated that patients who received oral nutrition immediately after their GI operation had a significantly decreased length of hospital stay in comparison to oral nutrition initiated later. 14
The effect of ERAS protocols on length of hospital stay is considered to be one of the most significant indicators of the effectiveness of these protocols. In the current study, paediatric patients that received the ERCs (group 2) were discharged significantly earlier compared with patients that did not receive the ERCs (group 1) (P = 0.001), a finding that was supported by the results of a previous study that demonstrated a positive relationship between ERCs application and duration of hospital stay for children with perforated appendicitis. 15
Despite the significant difference in the duration of hospital stay between the two groups, there was no significant difference in the hospital cost. This can be explained by the fact that laparoscopic appendectomies cost more than open surgeries, which would result in the overall hospital cost being similar for both groups.
There was no significant difference in the pain scores after surgery between the two groups in the current study, even though previous research has demonstrated significant improvements in pain after surgery due to the implementation of ERAS protocols; 16 and other studies have shown less postoperative opioid use.6,17,18 This current study found no relationship between ERAS protocol implementation and postoperative complication rates represented by ER visits, readmissions within 30 days and reoperations within 90 days, in contrast to previous studies that showed significantly lower complication rates both during the hospitalization period and after discharge when using ERAS protocols,10,13,19 while others showed no difference in ED visits and readmissions before and after implementing ERAS protocols. 6 The failure to show significant differences between the two groups in terms of postoperative complications might be due to the fact that patients undergoing open appendectomies usually receive some elements of enhanced recovery, in addition to the fact that most open surgeries are undertaken using small incisions.
This current study had several limitations. First, there was a lack of documentation regarding several aspects involving the recovery of the patients, such as the exact time of the first bowel movement, time to first mobility after surgery and several other parameters. Secondly, the study design was not a case–control study so it was not possible to identify two distinct groups in order to identify the exact effect of ERCs on a particular group.
In conclusion, the implementation of ERAS protocols in the management of paediatric patients undergoing appendectomy can decrease the duration of hospital stay compared with open techniques. The early introduction of feeding might also be associated with a faster recovery and shorter duration of hospital stay. Based on these current findings, ERAS protocols are being implemented in Jordan University Hospital protocols. However, more controlled studies are needed to evaluate the effectiveness of ERAS protocols in paediatric patients undergoing GI surgeries such as appendectomies and other procedures. Although there is evidence in the literature that ERAS programmes should be used on paediatric patients, official guidelines on the ERAS protocols that should be used in paediatrics str still missing and additional prospective studies investigating the implementation of ERAS protocols in paediatric surgical patients are needed.
Footnotes
Author contributions
Raed Al-Taher: first author, supervision and direction of the study, final manuscript editing and publishing; Mohammad Rashdan: manuscript revision and checking the references; Marzouq Amarin: revision of the results of the data analysis; Rami Addasi: creation of graphs, charts and tables; Hebah Alshahwan: data collection and manuscript editing; Saja Abdelhadi: data collection and literature review; Farah Abu Abeeleh: data collection and analysis; Doha Alsaraireh: data collection and manuscript design; Ahmad Abu-shanab: supervision and reviewing the scientific content; Nader Alaridah: reviewing and manuscript writing.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from funding agency in the public, commercial, or not-for-profit sectors.