
Abstract
The formation of stone in the ductal system of the salivary gland is termed sialolithiasis, with the submandibular gland being the most commonly affected. The precise aetiology is unknown but certain factors peculiar to the submandibular gland accounts for its likelihood of developing a calculous disease. Stones are classified based on their dimension, and may be silent or present with symptoms attributable to the size, location and complications. Here, a 50-year-old female who presented with a painless swelling in the left submandibular region that had grown slowly over the previous year, is reported. Following clinical and radiologic evaluation, left submandibular stone disease was preoperatively diagnosed. The patient underwent sialoadenectomy with transient palsy of the marginal mandibular branch of the facial nerve. Histopathology confirmed sialolith (2.7 cm) with severe squamous metaplasia of the duct. This presentation demonstrates some peculiar features attributable to the size, vertical orientation and location of the stone, in addition to the compression of the gland, thick fibrous capsule and significant squamous metaplasia of the duct. These findings require further evaluation for optimal treatment in view of the emerging trends for managing sialolithiasis.
Keywords
Introduction
Sialolithiasis refers to the formation of a stone within the duct system of the salivary gland, and is one of the most common diseases of the salivary glands, commonly involving the submandibular gland. 1 Found in 1.2% of the adult population, sialolithiasis affects more adults than children, and more males than females in the third to sixth decades of life.2,3 The exact aetiology is unknown, but it is associated with salivary stasis and ductal inflammation resulting in ductal injury with mucus plugs and eventual calcification. 1 The propensity towards occurrence in the submandibular gland has been attributed to the larger calibre and antigravity angulation of Whartons duct. 4 Other causes include foreign bodies and ductal metaplasia. 1 Sialoliths greater than 15 mm in any one dimension are considered large, while those of 35 mm or more are described as giant.1,5 Stones may be silent, clinically diagnosed, discovered on X-ray or ultrasonography, or present with complicating symptoms due to obstruction or infection. 1 Treatment depends on the location and size of the stone.4,6 Herein, the case of a 50-year-old female patient with a painless large submandibular sialolith is described, in order to highlight various peculiar features that may predispose to stone formation and possible risk associated with calculous disease.
Case report
A 50-year-old female presented to the University of Calabar Teaching Hospital Calabar, Nigeria, in March 2022, with a painless swelling beneath the left side of the jaw for the previous year. The swelling had gradually increased it, with an initial sensation of heat over the mass externally and in the intraoral location. The patient experienced no pain associated with feeding. Initial examination revealed an oval mass measuring about 5 × 3 cm in the left submandibular region. The mass was hard, non-tender, mobile, not adherent to the overlying skin or underlying structures, and was not associated with regional lymphadenopathy (Figure 1). Bimanual examination revealed no tenderness or intraoral purulent discharge. Part of the swelling was felt intraorally at the base of the tongue with slight elevation of the left side of the tongue. The patient was clinically diagnosed with submandibular stone disease.

Clinical photograph showing swelling of the left submandibular gland in a 50-year-old female patient diagnosed with submandibular sialolithiasis.
Investigations included the following blood results: haemoglobin, 11 g/dl; packed cell volume, 33%; white blood cell count, 3.2 × 109/l (comprising lymphocytes, 22%; monocytes, 4.0%; neutrophils, 72.0%; eosinophils, 1%; and basophils, 0.5%); and platelets 254 × 109/l. Urinalysis was unremarkable. A mandibular occlusal radiograph revealed a calcified left swelling adjacent to the root of 3rd molar in a vertical orientation relative to the lower border of the mandible, with a central radiolucent area. No bony involvement was found (Figure 2). The patient was preoperatively diagnosed with sialolithiasis of the left submandibular gland to rule out calcified submandibular gland tumour.

Radiograph of the Jaw (left lateral view) in a 50-year-old female patient diagnosed with submandibular sialolithiasis.
Under general anaesthesia by endotracheal intubation with halothane and maintenance with intravenous propofol, the patient underwent excision of the submandibular gland, via an incision placed 2 cm beneath the lower border of the mandible. Figure 3a shows the submandibular gland in situ. The wound was closed in layers. The cut surface of the gland revealed a rough fibrous mass that enclosed the stone, with compressed glandular structure (Figure 3b). Due to no internal facility for analysing the stone, the specimen was sent away for histology. The postoperative period was uneventful except for transient marginal mandibular facial nerve palsy that resolved at 2 weeks after surgery.
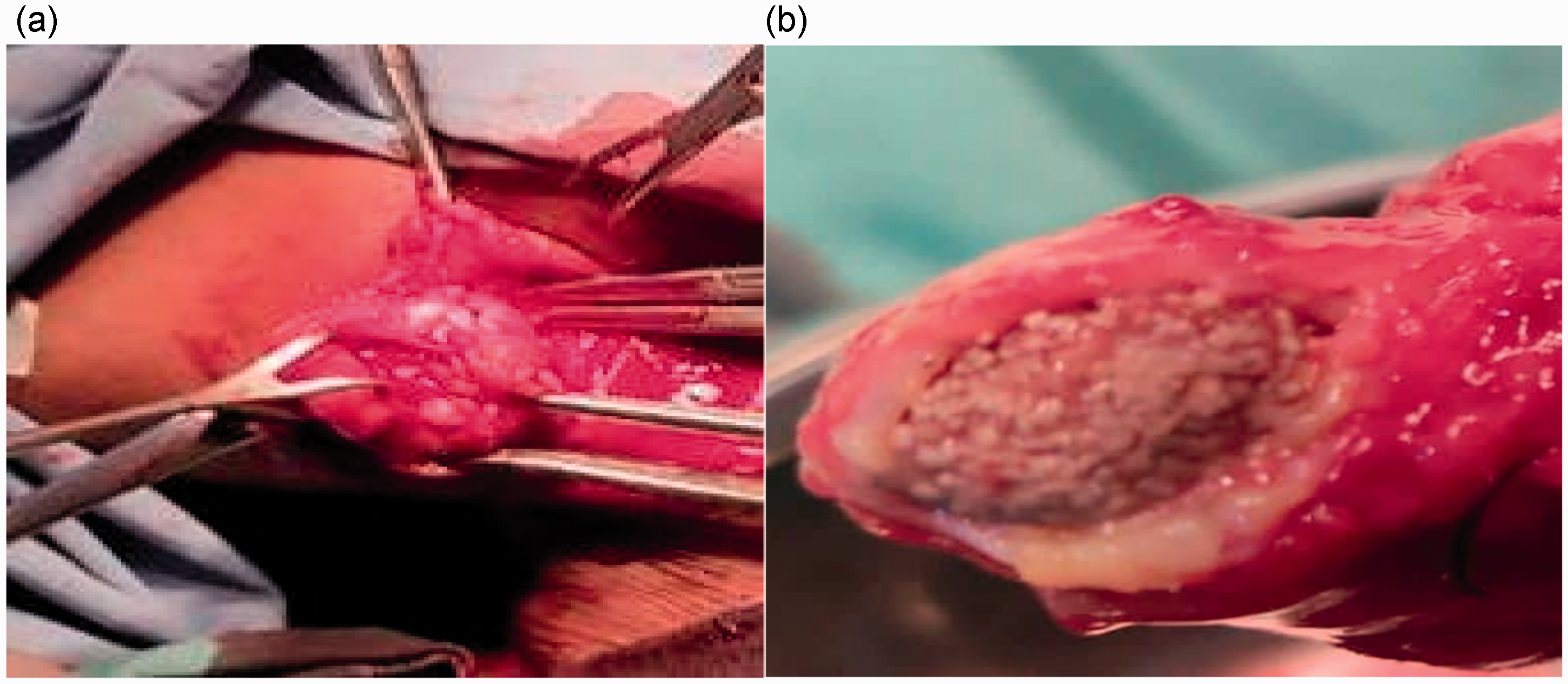
(a) Intraoperative photograph showing the submandibular gland in situ in a 50-year-old female patient diagnosed with submandibular sialolithiasis and (b) photograph of the cut surface of the submandibular gland from a 50-year-old female patient diagnosed with submandibular sialolithiasis, showing the encapsulated stone.
At histology, the cut surface of the mass revealed a thick fibrous capsule with the stone in situ and a smooth surface of the cavity (dilated duct). The stone was found to measure 2.7 cm × 1.5 cm (Figure 4a and 4b). Histological analysis revealed submandibular gland sialolithiasis with severe ductal squamous metaplasia (Figure 5a and b and Figure 6a and b), and the patient received a definitive diagnosis of submandibular sialolithiasis.
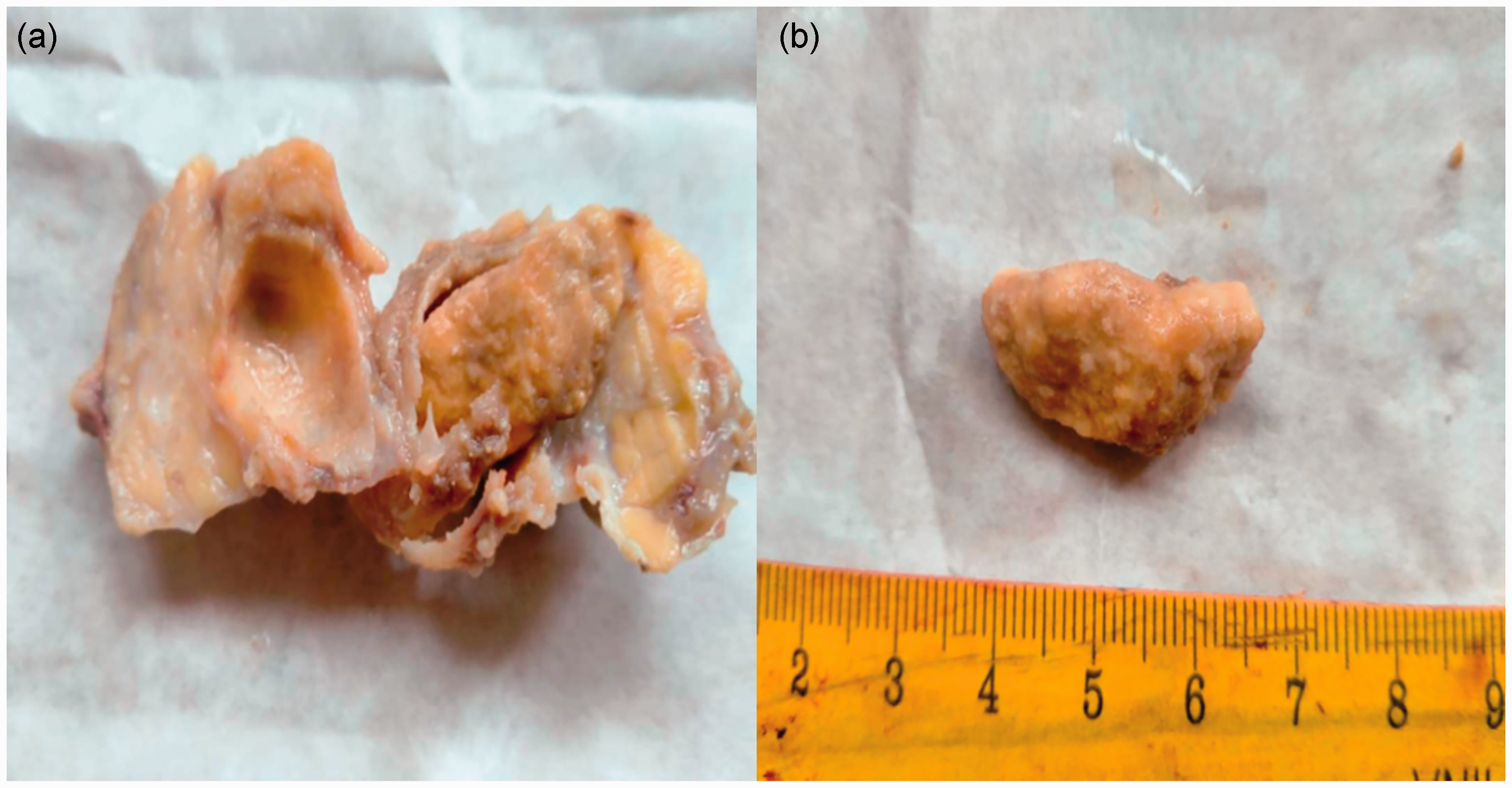
(a) Photograph of the cut surface of the mass from a 50-year-old female patient diagnosed with submandibular sialolithiasis, showing the dilated duct and stone in situ and (b) photograph of the sialolith from a 50-year-old female patient diagnosed with submandibular sialolithiasis.

(a) Photomicrograph of a haematoxylin and eosin-stained tissue section of the excised submandibular gland with dilated duct from a 50-year-old female patient diagnosed with submandibular sialolithiasis (original magnification, × 40) and (b) photomicrograph of a haematoxylin and eosin-stained tissue section of the excised submandibular gland with dilated duct from a 50-year-old female patient diagnosed with submandibular sialolithiasis (original magnification, × 100).

(a) Photomicrograph of a haematoxylin and eosin-stained ductal epithelium tissue section from a 50-year-old female patient diagnosed with submandibular sialolithiasis (original magnification, × 40) and (b) photomicrograph of a haematoxylin and eosin-stained ductal epithelium tissue section from a 50-year-old female patient diagnosed with submandibular sialolithiasis, showing squamous metaplasia (original magnification, × 100).
The patient provided both verbal and written informed consent for the reporting of this case and all accompanying images. The requirement for ethics approval was waived because this study was the report of a case managed by a clinical team at the University of Calabar Teaching Hospital, and not an interventional study (i.e., no intervention or experimentation was conducted for the purpose of the study). The reporting of this study conforms to CARE guidelines. 7
Discussion
Sialolithiasis is a common disease of the salivary gland that is more common in adults than children and is estimated to affect 12 in 1000 of the adult population. Calculous disease of the salivary gland may occur at any age, but commonly occurs in the third to sixth decades of life,1,2 with the current patient presenting in their fifth decade. Sialolithiasis is more common in males, with a male to female ratio of 2:1, however, there is no predilection for the right or left side, and it may present as multiple and bilateral disease.6,8,9
More than 80% of sialoliths occur in the submandibular gland or ducts, 5–20% occur in the parotid gland, and 1–7% occur in the sublingual gland.1,2 Stones may be intraductal or intraglandular, with most stones (75–85%) found in the ducts, 10 as was demonstrated in the present case, with ductal epithelium that showed severe squamous metaplasia. Ductal stones are elongated in shape as opposed to the oval shape found in the hilar region. 11
Inherent factors peculiar to the submandibular gland favour stone development: larger and longer calibre of ducts, anti-gravity flow of saliva due to angulation around the mylohyoid muscle resulting in slower flow rate of saliva, in addition to higher alkalinity, mucin and calcium content of saliva. The vertical orientation and location of the stone in the present case depicts an anti-gravity disposition of the duct, a likely contributory factor to stone formation in this patient.
Sialoliths of more than 15 mm in any one dimension are considered large, while those of 35 mm or more are considered giant.1,2 The largest reported Sialolith was 6 cm long, and was found in the submandibular gland. 9 Salivary stones are composed mainly of calcium phosphate with an organic matrix of glycoprotein and mucopolysaccharides. Bacteria have not been identified in the core of salivary stones. 12 Radiologic features of the sialolith in the present case included a radiolucent core and outer radiopaque area, in keeping with the allusion of having matrix on which calcium is deposited. However, some stones may be radiolucent and unlikely to be detected on X-ray, but ultrasonography and computed tomography detect both radiopaque and radiolucent calculi. 1
Stones may be silent and present as an incidental finding, or may typically present with recurrent painful swelling following meals, known as ‘mealtime syndrome’. Presentation may be in the form of complication with acute suppurative sialadenitis and abcess. 1 The patient in the current case presented with painless swelling. This was due to the ability of the duct adjacent to the sialolith to dilate, allowing normal secretion of saliva around the stone, which allows a stone to grow into a huge or giant calculus. 13
Generally, algorithms for the treatment of sialolithiasis depend upon the location and size of the sialolith. Total conservative management is used for small stones, and requires good rehydration, warm moist heat and gland massage. This may be in addition to the use of sialagogues used to promote saliva secretion that will flush the stone out of the duct. Appropriate antibiotics are indicated when signs of infection are present. Sialolithotomy is indicated when conservative management has failed. Sialodochoplasty may also be performed to deliver stones located close to the opening of the duct. Concerning distal stones, a transincision is made distally guarding against injury to the lingual nerve. Patients with large sialoliths in a proximal location may be offered extracorporeal shock wave lithotripsy (ESWL). Endoscopic intracorporal shock wave lithotripsy (EISWL) is gaining importance in the treatment of calculous disease as it is associated with less damage to adjacent tissue. Sialendoscopy, a non-invasive technique, is indicated for large stones and ductal obliteration. Minimal bleeding and less scaring occurs with the use of a CO2 laser. Other advantages are clear vision and minimal postoperative complications, and thus, CO2 laser treatment is gaining popularity.
The treatment approach is based on the size and location of the sialolith. 1 Stones located within 2 cm of the duct orifice may be removed intraorally, while those located in the posterior part of the duct and those within the gland require submandibular sialoadenectomy, as indicated in the present case. The hypoglossal nerve, lingual nerve, and the marginal mandibular branch of the facial nerve are usually at risk depending on the route of treatment. The patient in the present case experienced transient marginal mandibular nerve palsy with complete recovery within 2 weeks of surgery.
Histology of the dilated duct revealed severe squamous metaplasia. The risk of squamous metaplasia of the duct epithelium associated with long-standing stones requires further evaluation in view of the possible risk of malignancy development. This may also serve as a precipitating factor for further development of calculous disease when left behind after stone extraction. 8 If squamous metaplasia predated the process of stone formation, might it be a precipitating factor for the formation of a stone?
In conclusion, the presentation in this case highlights certain peculiarities of size, orientation, location of stone, glandular compression/atrophy, thick fibrous capsule and risk of significant squamous metaplasia of the duct that require further evaluation. In addition, the emerging modalities of treatment are highlighted for improved outcomes in the management of sialolithiasis.