
Abstract
Objective
This study was performed to compare the performance of rotational versus standard insertion of the i-gel® (Intersurgical, Wokingham, Berkshire, England) in patients of advanced age.
Methods
This single-center, randomized, double-blind trial involved 140 patients of advanced age undergoing general anesthesia. The patients were randomized into the standard group and rotational group. The primary objective of this study was to compare the success rate of the first attempt. The secondary outcome indicators were the insertion time and postoperative complications.
Results
The placement success rate on the first attempt was significantly higher in the rotational group than in the standard group (92% vs. 73%, respectively). The overall success rate was 100% for the rotational method and 95% for the standard method. The mean ± standard deviation insertion times were similar (15 ± 7.34 vs. 14 ± 7.26 s, respectively). The incidence rates of blood staining of the i-gel®, hoarseness, and sore throat did not increase with the rotational technique and were not significantly different from those of the standard method.
Conclusion
Compared with the standard method, the rotational method of i-gel® insertion had a higher success rate and did not increase the insertion time and complications in patients of advanced age.
Trial registration: This trial was registered at the Chinese Clinical Trial Registry (ChiCTR2000038763, Date of registration: 30/09/2020).
Introduction
With the aging of the global population, the need for supraglottic airway management has been increasing in patients of advanced age. 1 For this purpose, the i-gel® laryngeal mask (Intersurgical, Wokingham, Berkshire, England) has been widely used in geriatric anesthesia because of its superior performance. The i-gel® is inserted through the oral cavity and advanced along the hard and soft palates until it reaches the larynx, where it is positioned in the area of the base of the tongue. 2 This is the standard i-gel® insertion method. The i-gel® is usually inserted with its concave surface facing the lower jaw. In some cases, this insertion method may be obstructed by the tongue, 3 preventing the i-gel® from reaching the pharynx.
One case report suggested the use of a reverse approach for placing a supraglottic airway device after failure of the standard technique 4 ; this was the first report of reverse placement. Ghai and Wig 5 reported that laryngeal mask placement by the reverse insertion technique was easily performed in children. Some studies have shown improved success rates and reduced times required for i-gel® insertion using the rotational method in young patients.6,7 Kim et al. 8 reported that the classic laryngeal mask airway was less effective in advanced-age patients than in young adult patients because of age-related changes in the upper airway.
The internal muscles of the oral cavity are more relaxed in advanced-age patients than in young patients. Additionally, older patients are more prone to posterior tongue folding. 8 Consequently, i-gel® insertion is different between advanced-age and young patients. However, few studies have assessed i-gel® insertion by rotation in patients of advanced age. Therefore, we have improved the process of inserting the i-gel®. Specifically, we insert the i-gel® with the concave surface facing the hard palate; after the entire hooded capsule has been placed in the oral cavity, the i-gel® is rotated 180 degrees clockwise and advanced until the resistance of the pharynx is felt. Rotational placement is an improvement of standard placement with an additional rotation action. However, few studies have assessed i-gel® insertion by rotation in patients of advanced age. Outcomes such as the success rate of the first placement, the overall success rate of laryngeal mask placement, the insertion time, and postoperative complications after rotational insertion of the i-gel® have not been fully demonstrated. Therefore, we designed the current study to compare the efficacy of rotation versus standard i-gel® insertion methods in an advanced-age population.
Materials and Methods
Study design
This single-center, randomized, double-blind trial was conducted at Anqing Municipal Hospital from October 2020 to June 2021 in accordance with the Declaration of Helsinki. The study was approved by the Anqing Municipal Hospital's research ethics committee (Medical Ethics Approval No. 62 of 2020) on 12 October 23. It was registered in the Chinese Clinical Trial Registry (ChiCTR2000038763, Principal investigator: Jinjuan Duan, Date of registration: 30/09/2020). This randomized trial was reported according to the CONSORT statement. 9 Written informed consent was obtained from all participants. The inclusion criteria were having been scheduled to undergo elective short-term surgery, a requirement for the supine position and general anesthesia, age of 60 to 80 years, American Society of Anesthesiologists status of I or II, modified Mallampati airway classification grade of I or II, and body mass index of 18 to 28 kg/m2. The exclusion criteria were predicted airway difficulties, risk of accidental aspiration, a smoking habit, and a history of sore throat or hoarseness.
Randomization and masking
Randomization was determined using the Python random number generator, and this information remained hidden in opaque envelopes until the induction of anesthesia. Randomization was not blocked or stratified. The patients were randomly assigned to the standard group or rotational group at a ratio of 1:1. Throughout the study, all patients, researchers, anesthesiologists, surgeons, nurses in the post-anesthesia nursing unit and wards, and recorders of the perioperative observation aims remained blinded to the study group allocations.
Study treatments
All patients underwent the same preoperative evaluation and fasting protocol. Upon arrival in the operating room, the patients were monitored using noninvasive blood pressure measurement, electrocardiography, pulse oximetry, and bispectral index monitoring. Their head was supported by a 5-cm-high square pad (gel pad, silicone pad, or sponge pad) to prevent it from swaying from side to side after anesthesia. All patients were pre-oxygenated with a face mask at an oxygen flow rate of 6 L/min for approximately 3 minutes. Before anesthetic induction, the head end of the table was separated by a curtain to blind the designated person to the insertion technique; this person stayed at the foot end of the table and recorded data in the patient’s chart. Standardized general anesthesia was induced using 0.05 mg/kg of midazolam, 0.5 μg/kg of sufentanil, 2 mg/kg of etomidate, and 0.2 mg/kg of cisatracurium. Three minutes after cisatracurium administration, the i-gel® was inserted by an anesthesiologist with more than 10 years of experience. All i-gel® devices were inserted by the same single anesthesiologist in both groups. The i-gel® size was selected based on the patient’s body weight in accordance with the manufacturer’s instructions (30–60 kg, size 3; 50–90 kg, size 4; and >90 kg, size 5). The i-gel® cuffs were lubricated with water-based jelly on the front, sides, and back.
In the standard group, the i-gel® was inserted into the mouth with its concave side facing the lower jaw. Using a pen-holding grip, it was then advanced along the hard palate, soft palate, and posterior pharynx until it reached the larynx. In the rotational group, the i-gel® was inserted with the concave side facing the hard palate. The entire hood was rotated 180 degrees clockwise as it reached the oropharynx, and the device was further inserted into the laryngopharynx until the final position was reached.
The appropriate position of the i-gel® was determined by auscultation, observation of chest wall motion and tidal volume, and the square-wave end-tidal carbon dioxide waveforms. If ventilation was poor, manipulations such as head extension, chin lift, chin push-down, neck flexion, and changing the position of the i-gel® in the pharynx were used to improve ventilation. When air leakage persisted, the attempt was considered a failure, and the i-gel® was reinserted by the same technique. The performance of three or more insertion attempts was considered an overall failure, and airway management was performed using a tracheal tube. The insertion time and the number of insertion attempts were recorded for both techniques. The insertion time was measured from the cessation of mask ventilation to the appearance of the carbon dioxide square wave; it did not include the time between the two attempts.
Intraoperative monitoring included noninvasive blood pressure, heart rate, electrocardiography, pulse oximetry, and end-tidal carbon dioxide. Anesthesia was maintained using remifentanil and propofol in balanced proportions. At the end of the surgical operation, the i-gel® was pulled out as soon as the patient had fully resumed coughing and accurately responded to verbal commands. Observers who did not participate in the study checked for traces of blood on the i-gel® after removal. Postoperative airway morbidities, including hoarseness (defined as a lower or thicker tone of voice, or even a whisper or loss of sound) and sore throat (defined as patient-reported pain in the throat when swallowing), were recorded immediately and 24 hours after the procedure.
Statistical analysis
According to the pre-experiment, the success rate of the first attempt at insertion of the i-gel® using the standard technique was 80%. Accepting a 20% incremental improvement in the success rate, we calculated that a minimum sample size of 61 patients was required in each group. Therefore, 70 patients per group were enrolled to compensate for possible dropouts.
The statistical analyses were performed using SPSS 11.0 (SPSS Inc., Chicago, IL, USA). Categorical data are presented as number (percentage) and were analyzed by the chi-square test or Fisher’s exact test. Continuous variables are presented as mean ± standard deviation or median (interquartile range) and were analyzed by the independent t-test or the Mann–Whitney U test A two-tailed p value of <0.05 was considered statistically significant.
Results
The primary objective of this study was to compare the success rate of the first attempt. The secondary outcome indicators were the insertion time and postoperative complications.
Of the 140 patients enrolled from October 2020 to June 2021, 16 refused to participate in this study and 4 had difficult airways. Finally, 120 patients (60 in each group) completed the study (Figure 1).
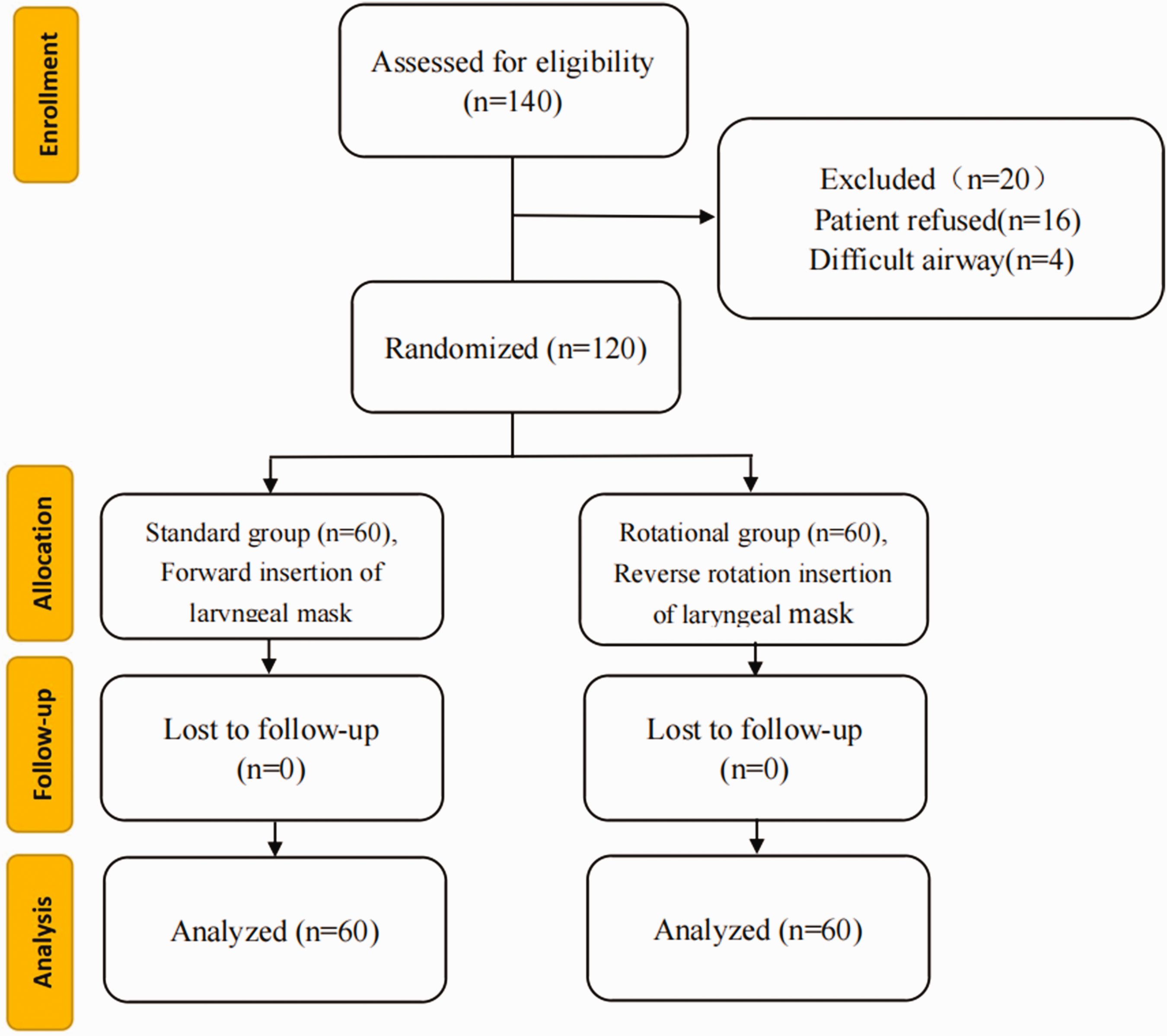
Study flow diagram.
There were no significant differences in sex, age, body mass index, American Society of Anesthesiologists status, Mallampati grade, weight, height, or site of surgery between the two groups (Table 1).
Patients’ demographic data.

Data are presented as n or mean ± standard deviation.
F, female; M, male; BMI, body mass index; ASA, American Society of Anesthesiologists.
Table 2 shows the parameters associated with i-gel® insertion. Compared with standard insertion, rotational insertion had a significantly higher success rate on the first attempt (92% vs. 73%, respectively; p = 0.015) and higher overall success rate (100% vs. 95%, respectively) but a similar mean time required for i-gel® insertion (rotational method: 15 ± 7.34 s vs. standard technique: 14 ± 7.26 s). Therefore, rotational insertion did not require more time.
Comparison of airway management success between the two groups.

Data are presented as n (%) or mean ± standard deviation.
The incidence of airway complications is shown in Table 3. Significantly more patients developed hoarseness in the rotational group than in the standard group (14 vs. 3, respectively; p = 0.007), but similar numbers of patients had blood staining of the i-gel® (7 in both groups), developed a sore throat (18 vs. 11, respectively), and developed airway complications 24 hours postoperatively (hoarseness: 8 vs. 3 and sore throat: 9 vs. 6, respectively).
Comparison of postoperative complications between the two groups.

Data are presented as n (%).
AR, immediately after removal of the i-gel®; POD, postoperative day.
Discussion
This study showed that the success rate of i-gel® insertion at the first attempt was higher with the rotational method than with the standard method in patients of advanced age. In addition, the overall success rate was higher for the rotational technique than for the standard technique. The success rate of the first attempt of i-gel® insertion is a key parameter when considering the important role of the supraglottic airway in maintaining airway patency and oxygenation. In the present study, this parameter was used as the main outcome variable, and the overall insertion success rate, insertion time, and airway complications were also included to provide more comprehensive information.
Some researchers have reported that the success rate of standard insertion of the i-gel® at the first attempt was 78% to 100% in young patients.10,11 However, this rate was lower in the present study (73%). The aged population is more prone to posterior tongue folding, 12 which might contribute to lower first-attempt success of i-gel® insertion.
Kim et al. 13 reported a significantly higher first-attempt success rate with the rotational method than with the standard method. Similarly, the present study showed a higher first-attempt success rate with the rotational technique (92%) than with the standard technique (73%). The traditional method of inserting the i-gel® may obstruct oropharyngeal access because of folding of the tongue, making advancement of the i-gel® difficult. Backward displacement or folding of the tongue is the main cause of failed supraglottic airway insertion. 14 The rotational method of i-gel® insertion can reduce airway obstruction and enable smooth insertion of the i-gel® by reducing the incidence of backward displacement or folding of the tongue. This would explain the improved overall and first-attempt insertion success rates with the rotational technique of i-gel® placement.
Prolonged apnea during anesthetic induction may lead to hypoxia, 7 which is more likely to occur in patients of advanced age with an insufficient oxygen reserve. Kumar and Joshi 15 reported no significant differences in the i-gel® insertion time between the rotational and standard techniques. Likewise, our results showed that the rotational technique did not increase the insertion time compared with the standard technique.
One study showed that the incidence of trauma and blood staining was significantly reduced with use of the rotational i-gel® insertion technique. 16 In our study, the incidence of hoarseness was significantly lower with rotational insertion than with standard insertion, but the incidence of sore throat and blood staining was similar. The development of upper respiratory complications may be related to the operator’s skill level. Nevertheless, rotational insertion of the i-gel® did not increase the number of airway complications in patients of advanced age.
Our study had some limitations. The sample size was limited; therefore, a comparison of the two techniques of i-gel® insertion should be performed on a large sample of advanced-age patients. Another limitation is that this study did not compare the condition of the patients’ teeth in the two groups. The number of teeth may impact the placement of the i-gel® and should be accounted for in future studies. Finally, the position of the i-gel® was not evaluated by the fiberoptic view.
Conclusions
Rotational insertion of the i-gel® laryngeal mask might be considered a more successful technique than the standard method in patients of advanced age because of the higher first-attempt and overall success rates without an increase in the insertion time or airway complications.
Footnotes
Authors’ contributions
JD and YL designed this study and wrote the manuscript. JD and LS performed the experiments. JD assisted with the data analysis. YL and SW revised the final manuscript. All the authors contributed to the final version of the manuscript.
Availability of data and materials
The datasets of the current study are available from the corresponding author upon reasonable request.
Consent for publication
Written informed consent for publication was obtained from all participants.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.