
Abstract
Objective
To determine the incidence and significance of ventilator avoidance in patients with critical coronavirus disease 2019 (COVID-19).
Methods
This prospective observational cohort study evaluated hospital mortality and 1-year functional outcome among critically ill patients with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)-associated acute respiratory distress syndrome (ARDS). The explanatory variable was ventilator avoidance, modeled as ‘initial refusal’ of intubation (yes/no). Modified Rankin Scale (mRS) scores were obtained from surviving patients (or their surrogates) via phone or email questionnaire.
Results
Among patients for whom intubation was recommended (n = 102), 40 (39%) initially refused (95% confidence interval [CI] 30%, 49%). The risk of death was 79.3% (49/62) in those who did not initially refuse intubation compared with 77.5% (31/40) in those who initially refused, with an adjusted odds ratio for death of 1.27 (95% CI 0.47, 3.48). The distribution of 1-year mRS scores was not significantly different between groups.
Conclusion
Among critically ill patients with COVID-19-associated ARDS, ventilator avoidance was common, but was not associated with increased in-hospital mortality or 1-year functional outcome.
Keywords
Introduction
Political and media polarization of the coronavirus disease 2019 (COVID-19) pandemic has resulted in misinformation that has undermined health system attempts to manage the pandemic.1–4 Misinformation has contributed to increased violence against healthcare workers, lawsuits demanding unproven medications and other patient–physician disagreement often resulting in non-adherence to medical recommendations. 5 Ventilator avoidance is a type of medical non-adherence that became common during the COVID-19 pandemic due to the rapid spread of misinformation that mechanical ventilators, and not severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, were the cause of high mortality rates associated with mechanical ventilation for COVID-19-related respiratory failure.6,7
Medical non-adherence (treatment refusal) is not a new concept and has been associated with worse clinical outcomes.8,9 Hippocrates noted ‘The effects of various potions were recorded with notations of whether the patient had taken them or not! Keep a watch on the faults of the patients, which often make them lie about the taking of things prescribed. For through not taking disagreeable drinks, purgative or other, they sometimes die’. 9 When specifically considering ventilator avoidance, there are reasons to believe that non-compliance will increase mortality. Mechanical ventilation has been shown to be lifesaving, while delayed intubation has been associated with worse outcome, in various forms of acute respiratory distress syndrome (ARDS). Expectedly, guidelines do not endorse frequent or prolonged trials of non-invasive positive-pressure ventilation (NIPPV).10–14
Despite clinicians frequently encountering ventilator avoidance during COVID-19 (refusal due to false belief that mechanical ventilation, not the virus, causes patient death), the incidence and significance of these patterns remain poorly described in the medical literature. Accordingly, the aim of the present study was to evaluate the incidence of ‘initial refusal’ of intubation (for mechanical ventilation) in patients with COVID-19-related ARDS, then to compare outcomes between those who initially refused a recommendation for intubation with patients who did not refuse. We hypothesized that patients who initially refused intubation would have higher in-hospital mortality and worse 1-year functional outcomes.
Patients and methods
Study population, setting and design
This prospective observational cohort study included consecutive eligible patients who were admitted to The University of Michigan Health West, Wyoming, MI, USA between March 2020 and June 2021 with confirmed SARS-CoV-2 infection causing critical COVID-19. Critical COVID-19 was defined as: (1) ARDS requiring intubation or (2) ARDS requiring ≥60% FiO2 on high flow nasal canula (HFNC) or NIPPV for >6 h. Patients were excluded from the analysis if they were aged <18 years, and/or were critically ill with confirmed SARS-CoV-2 but without ARDS (i.e., thrombo-embolic disease, recrudescence or exacerbation or chronic medical illness in the setting of COVID-19, or ‘incidentally’ confirmed SARS-CoV-2). Additional exclusion criteria from the primary therapeutic analysis were patients in whom intubation was not ever recommended or those who were ‘do not intubate’ (DNI) on admission.
The University of Michigan Health West is a 210-bed community teaching hospital with a single medical-surgical intensive care unit (ICU). The ICU employs a high intensity intensivist staffing model, in which all patients are managed with in-house intensivist involvement. During the study period, multiple COVID-19 surges placed the hospital in disaster mode, extracorporeal membrane oxygenation (ECMO) was unavailable, and no regional quaternary care center was accepting transfers for ECMO. The ICU capacity was expanded from 18 beds to 38. The institutional COVID-19 guideline was consistent with National Institute of Health and World Health Organization guidelines during the study period. Patients generally received between 6–20 mg of dexamethasone with frequent use of either tocilizumab or baricitinib for early decline resulting in critical illness. Therapeutic anticoagulation was optional in critically ill patients and generally utilized based on pre-test probability of thrombosis balanced against bleeding risk. Remdesivir was typically continued if started during a non-critical phase of COVID-19. The institutional guidelines for managing ARDS and sepsis are informed by the ARDS network (https://www.ARDSNET.org) and Surviving Sepsis Campaign (www.sccm.org/SurvivingSepsisCampaign/Home) guidelines. Management of intubated patients included the frequent use of prone positioning, paralytics for patient-ventilator dyssynchrony, and inhaled vasodilators. Scales to predict failure of respiratory support (e.g., HACOR and ROX scores) were not included in any institutional guideline or tracked as singular vital signs in the electronic medical record. The recommendation for intubation was decided by the ICU physician, based primarily on increased work of breathing not responsive to NIPPV and/or awake prone position.
Data were obtained from a prospective COVID-19 outcomes registry that included baseline demographics and outcomes of all patients admitted with SARS-CoV-2 infection. For patients admitted more than once during the study period, the index admission was defined as the admission with the highest disease severity due to COVID-19.
Patients or their surrogates were called and/or emailed to collect information on multiple functional, neurocognitive, depression, anxiety, and post-traumatic stress disorder outcomes scales. This sub-study represents a subset of patients who completed phone interviews to evaluate 1-year modified Rankin Scale (mRS) and estimate pre-COVID functional status (mRS score). Given the uncertainty on timing of intubation in COVID-19 and previously mentioned misinformation, the intensivists decided a priori to document the recommendation for intubation in the electronic medical record during the index hospitalization. The airway team at the hospital includes the intensivist physician for all hospitalized patients. Study data were managed using Research Electronic Data Capture (REDCap) software, a secure, web-based application designed to support data capture for research studies (https://projectredcap.org/), hosted at the University of Michigan Health System.
The study was conducted and reported in accordance with the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) statement on reporting observational trials. 15 The study was approved by the Metro Health–University of Michigan Health Institutional Review Board, Wyoming, MI, USA (IRB No. 2021-14; approved 28 June 2021). Informed consent was obtained verbally and online via survey completion. All patient information included in the manuscript was de-identified.
Study variables
The primary explanatory variable was ventilator avoidance defined as ‘initial refusal’ of a recommendation for intubation (dichotomous no/yes). The secondary explanatory variable was intubation for mechanical ventilation. The primary outcome was the risk of in-hospital death in patients who initially agreed to intubation compared with those who initially refused intubation. The secondary outcome was distribution of 1-year post-COVID-19 mRS scores.
Statistical analyses
Categorical data are presented as n (%) prevalence. Continuous variables were screened for normality using normality plots and histograms. Data with normal distribution are presented as mean ± SD, and data without normal distribution are presented as median [interquartile range]. The normal approximation method was used to calculate the 95% confidence interval (CI) for the proportion of patients who initially refused intubation. For bivariate analysis, continuous variables were compared by two-sample t-test or Wilcoxon rank–sum test, as appropriate. The mRS scores, presented as median [interquartile range], were compared between groups using Wilcoxon rank–sum test, and graphically presented using Grotta Bars. Logistic regression models were employed to estimate the adjusted odds ratio (OR) of in-hospital death between those who initially refused intubation and those who did not. Similarly, logistic regression models were used to estimate the adjusted OR of in-hospital death between those who received intubation and those who did not. Data were adjusted for age and Charlson comorbidity index based on prior population-level data suggesting an association between advancing age and mortality following COVID-19.16,17 All analyses were performed with SAS 9.4 software (SAS Institute; www.sas.com) and a P-value <0.05 was considered statistically significant.
Results
During the study period, 315 patients were determined to be critically ill due to COVID-19-associated ARDS. The cohort consisted predominately of non-Latino white patients (238/315 [75.6%]) with a slight male predominance (206/315 [65.4%]). Most of the cohort was obese (179/315 [56.8%] had a body mass index >30 kg/m2) and 313 (99.4%) were unvaccinated. The overall in-hospital mortality rate for critically ill patients due to COVID-19 ARDS was 41.9% (95% CI 36%, 47%). On admission, 54 patients (17.1%) were DNI, 159 (50.5%) of the eligible patients never received a recommendation for intubation, and 102 (32.4%) of the patients in the cohort received a recommendation for intubation. Thus, a total of 102 patients were included in the present analyses. Of the 102 patients in whom intubation was recommended, 62 (61%) agreed and 40 (39%) initially refused to be intubated (95% CI 30%, 49%). Of those who initially refused 8 (20%) subsequently agreed to mechanical ventilation. Demographic and clinical data for the study cohort are summarized in Table 1. A flow diagram of study participants and outcomes (discharge disposition) is shown in Figure 1.
Demographic and clinical characteristics of critically ill COVID-19 patients with ARDS, and bivariate analysis by ventilator avoidance (initial refusal versus no initial refusal).

Data presented as mean ± SD, n (%) prevalence or median [interquartile range].
COVID-19, coronavirus disease 2019; ARDS, acute respiratory distress syndrome; LOS, length of stay; BMI, body mass index; CCI, Charlson Comorbidity Index; HFNC, high flow nasal canula; NIPPV, non-invasive positive pressure ventilation; mRS, modified Rankin Scale score; LTAC, long term acute care; NH, nursing home.
aFor patients who received intubation, HFNC and NIPPV were only documented as positive if they received therapy prior to intubation.

Flow diagram of study participant selection and outcomes. LTAC, long term acute care; NH, nursing home; Rehab, rehabilitation unit.
The risk of death was 79.3% (49/62) in those who did not refuse intubation compared with 77.5% (31/40) in those who initially refused (OR 1.1; 95% CI 0.42, 2.9). After adjusting for age and Charlson Comorbidity Index, the risk of death was not significantly different between those who did not initially refuse intubation and those who did initially refuse (OR 1.27; 95% CI 0.47, 3.48). The distribution of 1-year mRS scores was also not significantly different between those who initially agreed to intubation and those who initially refused (P = 1.0; Figure 2). Among the analysis cohort of 102 patients, in whom intubation was recommended, use of mechanical ventilation was not associated with a reduced risk of death (adjusted OR 1.6; 95% CI 0.5, 3.4) or any statistically significant difference in 1-year distribution of mRS score (Figures 3 and 4).
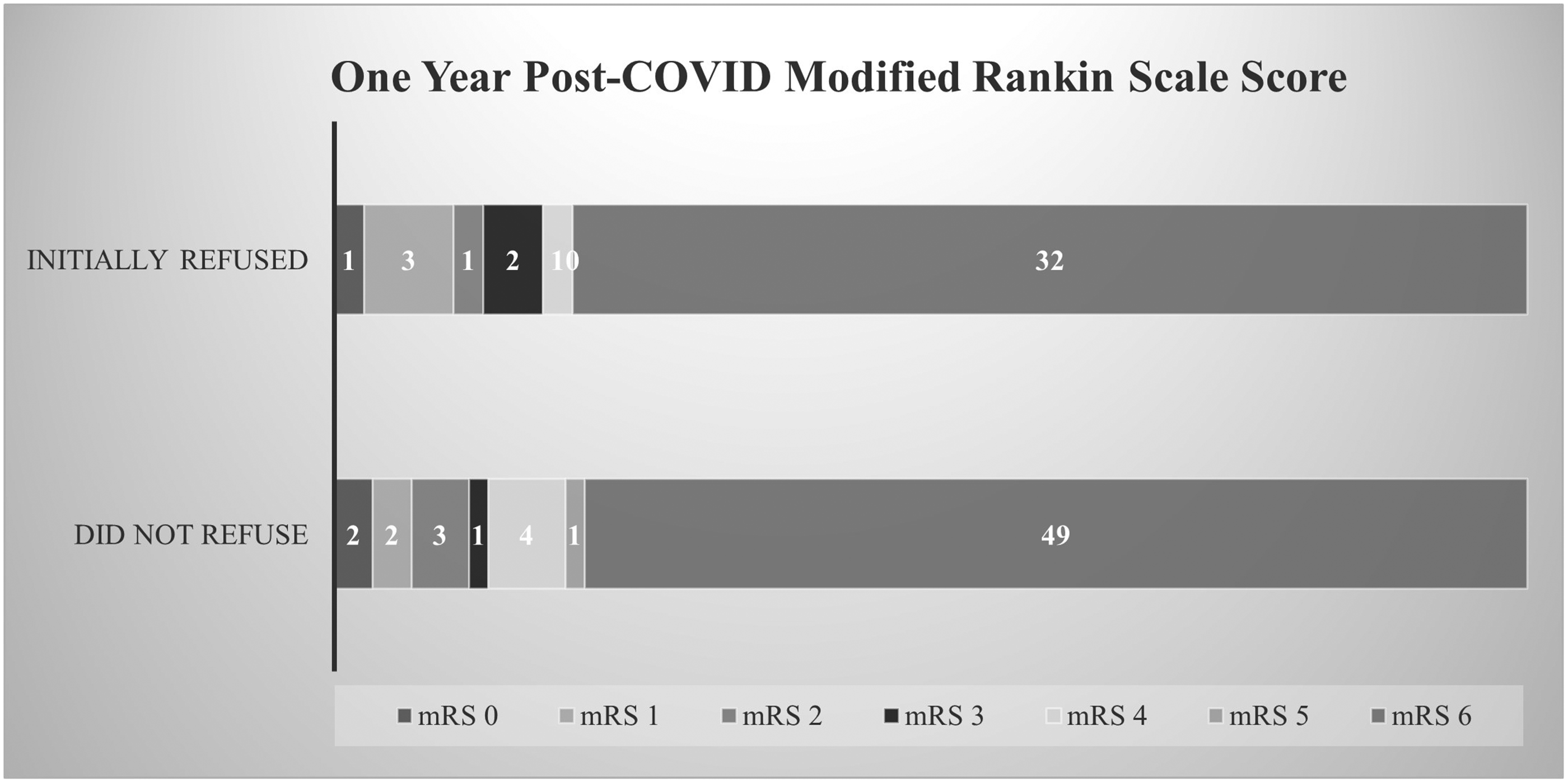
Distribution of 1-year mRS scores in 102 critically ill COVID-19 patients with ARDS dichotomized by initial refusal of intubation. ARDS, acute respiratory distress syndrome; COVID-19, coronavirus disease 2019; mRS, modified Rankin Scale.

Distribution of discharge disposition in 102 critically ill COVID-19 patients with ARDS dichotomized by mechanical ventilation. ARDS, acute respiratory distress syndrome; COVID-19, coronavirus disease 2019; LTAC, long term acute care; NH, nursing home; Rehab, rehabilitation unit.

Distribution of 1-year mRS scores in 102 critically ill COVID-19 patients with ARDS dichotomized by mechanical ventilation. ARDS, acute respiratory distress syndrome; COVID-19, coronavirus disease 2019; mRS, modified Rankin Scale.
Discussion
The present study demonstrated that ventilator avoidance was common, with 39% of patients initially refusing intubation (95% CI 30%, 49%). Initial refusal of intubation, however, was not associated with any difference in mortality or long-term functional outcome. In fact, the risk of death was numerically lower and the risk of discharge home numerically higher in those who initially refused intubation, although the differences were not statistically significant. In analysis using patients treated with mechanical ventilation as the explanatory variable, no statistically significant difference in survival or long-term functional outcome could be demonstrated between the groups.
The lack of association between the initial refusal of intubation and risk of death has multiple potential explanations. First, the stage at which mechanical ventilation was offered may have been too late to make a difference in mortality (selection bias). Despite having ARDS, the majority of patients in the present cohort had received HFNC, NIPPV, or both, prior to any intubation. Early in the pandemic there was enthusiasm for early intubation to avoid emergent intubations and limit spread of the virus. The realization that intubation was not required to limit spread, along with observations that many patients with severe hypoxia did not display increased work of breathing, subsequently lead to recommendations to consider trialling HFNC or NIPPV to conserve mechanical ventilators. However, later intubation has been associated with worse outcomes in other ARDS etiologies, and is one criticism of using scales to predict failure as they may delay intubation.10–14 Notably, the European Respiratory Society and the American Thoracic Society were unable to offer a recommendation on using NIPPV in patients with ‘de novo’ respiratory failure (pneumonia/ARDS), or for ‘viral pandemics’, in a 2017 clinical practice guideline. They did recommend that if NIPPV was selected, it should only be used by experienced teams for a time-limited trial. 14 Though the current literature on timing of intubation in patients specifically with COVID-19 suggests that timing of intubation may not make a difference, data are limited by the arbitrary definitions of early versus late intubation, and by lack of accounting well for disease severity.18,19 Indeed, there is evidence to suggest that a longer duration of hypoxia prior to intubation is associated with increased airway driving pressures, and that delayed intubation may increase mortality risk.10,20 Secondly, though biological plausibility suggests patient selection and timing are essential to demonstrating a benefit to mechanical ventilation, it is possible that mechanical ventilation does not provide a benefit in COVID-19-related ARDS. There are inherent risks of intubation, specifically ventilator-induced lung injury and use of scarce resources during surges. However, there are also risks to delaying intubation, such as silent hypoxia, cardiopulmonary arrest, spontaneous or NIPPV-induced large tidal volumes or barotrauma and atelectatic injury.10–13 Thirdly, the present study lacked precision, as the 95% CI for the OR predicting death (0.42, 2.9) for the primary outcome was wide and included both a clinically meaningful reduction in death and a clinically meaningful increased risk of death. Fourthly, clinical nihilism may have led to a self-fulfilling prophecy during a time of significant health-system burden and limited resources.
The present study also lacked the precision to evaluate differences in 1-year functional outcome in survivors of COVID-19 due to the high in-hospital mortality rate. Though the risk of death in the present ICU cohort was high (42% overall and 78% in those who received mechanical ventilation) it was consistent with other cohorts from early in the pandemic.21–23 Studies of later cohorts have reported mortality rates of 50% or lower in those with COVID-19 who are intubated, which is consistent with the reduction in mortality rate observed over time at The University of Michigan Health West.22,23 Though the present results may be generalizable to other relatively small community health systems that provide the majority of health care in the USA, we should acknowledge other factors that may affect external validity. The present cohort consisted largely of obese, unvaccinated patients during the earlier phase of the pandemic. Additionally, external validity may be affected over time as the pandemic has progressed, medical treatments have advanced, and immunity status of the population has changed.
Conclusion
Ventilator avoidance was common among the present cohort of patients with COVID-19-related ARDS. However, initial refusal of intubation was not associated with any difference in mortality or long-term functional outcomes.
Research Data
sj-pdf-1-imr-10.1177_03000605221135446 - Research Data for Ventilator avoidance among critically ill COVID-19 patients with acute respiratory distress syndrome
Research Data, sj-pdf-1-imr-10.1177_03000605221135446 for Ventilator avoidance among critically ill COVID-19 patients with acute respiratory distress syndrome by Jeffrey J Fletcher, Arielle Aughenbaugh, Catherine Svabek, Peter Y Hahn and Ronald G Grifka in Journal of International Medical Research
Footnotes
Acknowledgements
The authors would like to thank Dr Gabe Pedraza, Dr Eric Feucht, Dr Mark Tieszen and Dr Justin Shurts, and the Intensive Care Service at the University of Michigan Health West, for their dedicated patient care.
Author contribution
JJF, study concept, design, statistical analysis and drafting of the manuscript; AA, study concept and revision of the manuscript; CS, study design, drafting and revision of the manuscript; PYH, drafting and revision of the manuscript; and RGG, drafting and revision of the manuscript.
Data accessibility
Data is available within the article for reproduction.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.