
Abstract
In recent years, the more widespread availability of biological drugs with specific mechanisms of action has led to significant breakthroughs in the management of severe asthma. Over time, numerous randomised clinical trials have been conducted to evaluate the efficacy and safety of these biologics and define the eligibility criteria of patients suitable for various therapeutic options. These studies were conducted under controlled conditions not always applicable to real life. For this and other reasons, real-world evidence and pragmatic studies are required to provide useful information on the effectiveness of biological drugs and their safety, even in the long term. Because differences in outcomes have sometimes emerged between clinical trials and real-life studies, it is important to clarify the causes of these discrepancies and define the significance of the results of studies conducted in the course of daily clinical practice. Thus, a scientific debate is ongoing, and no consensus has been reached. The purpose of this narrative review is to analyse the differences between randomised trials and real-world evidence studies, focusing on their roles in guiding clinicians among different therapeutic options and understanding the reasons for the large discrepancies often found in the results obtained.
Introduction
In recent years, the more widespread availability of biological drugs with specific mechanisms of action (MoAs) directed at the underlying mechanisms of the disease has led to significant breakthroughs in the management of severe asthma (SA). These biologics include anti-human immunoglobulin E (IgE), anti-interleukin (IL)-5 or its receptor present on the surface of eosinophils, and anti-IL-4/IL-13.1,2 Over time, numerous randomised clinical trials (RCTs) have been conducted to evaluate the efficacy and safety of these biologics and define the eligibility criteria of patients suitable for various therapeutic options. However, these studies were conducted under controlled conditions (established by strict patient selection criteria) not always applicable to real life.3,4 For this and other reasons, real-world evidence (RWE) and pragmatic studies are required to provide useful information on the effectiveness of biological drugs and their safety, even in the long term. These studies are also important because they play an essential role in the post-marketing surveillance phase.
Because differences in outcomes have sometimes emerged between RCTs and RWE studies, it is important to clarify the causes of these discrepancies and define the significance of the results of studies conducted in the course of daily clinical practice. Thus, a scientific debate is ongoing, and no consensus has been reached in this regard; this requires attention in light of the growing importance of RWE studies and real-world data (RWD) from a regulatory perspective and in healthcare decisions. 5 The US Food and Drug Administration (FDA) is increasingly adopting RWD and RWE to monitor safety and post-market adverse events as well as make regulatory decisions. Moreover, the scientific community can use RWD to define guidelines and other decision-support tools for clinical practice. 6 Manufacturers of drugs and other medical products use RWD and RWE to support clinical trial projects for the development of new and innovative therapeutic approaches. Furthermore, the European Medicines Agency (EMA) also considers RWE studies to be increasingly important; hence, it is developing the Data Analysis and Real World Interrogation Network to allow the use of RWD on a continental European scale and define the real value of such data for regulatory development and the authorisation of medicines by 2025. This network will allow health data from across the European Union to be accessed and analysed, and it is expected to be launched in 2022. 7
The purpose of this narrative review is to analyse the differences between RCTs and RWE studies, focusing on their roles in guiding clinicians among different therapeutic options and understanding the reasons for the large discrepancies often found in the results obtained. Another aim of the review is to highlight how the complementary use of RCTs and real-life studies is crucial in defining the effectiveness and efficacy of biologics for severe refractory asthma.
Methods
Study selection and data source
We conducted a review of English-language literature relating to clinical trials and RWE studies on biologics for SA published from database inception to July 2022. The main biomedical bibliographic databases were searched: MEDLINE (PubMed), EMBASE, and SCOPUS. The search terms used were ‘biological’, ‘monoclonal antibodies’, ‘biomarkers’, ‘severe asthma’, ‘clinical trials’, ‘real-life’, ‘real-world’, ‘efficacy’, ‘effectiveness’, ‘exacerbations’, and ‘comparison’.
Role of biomarkers in asthma phenotyping and endotyping
Asthma is an extremely heterogeneous disease in terms of severity, clinical manifestations, and inflammation type. These factors determine the response to treatment and long-term outcomes. The characterisation of asthma based on phenotypes and endotypes allows us to more precisely determine the mechanisms underlying the disease; hence, the role of biomarkers is crucial. 8
Endotypes include the pathological mechanisms underlying the disease, whereas phenotypes represent the clinical manifestations. 9 Based on the classification by endotypes, asthma can be categorised into type 2 (T2) and non-T2, although there is evidence of other subtypes linked to the structural components of the inflammasome and mixed subtypes 1, 2, and 17.10,11 Phenotypes mainly include the patient characteristics (such as age, sex, and ethnicity), morphophysiological features of the airways, response to drugs, and related clinical outcomes. 10 The increasing knowledge of endotypes and phenotypes has enabled a better understanding of asthma and the possibility of applying a personalised approach to therapies. Most of the biologics currently available for the treatment of SA act on different targets of T2 inflammation by targeting the allergy-associated molecules IgE and interleukins involved in T2 inflammation (IL-5, IL-4, IL-13, and thymic stromal lymphopoietin).11,12 T2 biomarkers are the only biomarkers currently usable as asthma biomarkers in clinical practice. Although these molecules do not have predictive capabilities, they can be very useful in the management of biological drugs. The most appropriate biologic for each patient should be selected based on clinical characteristics such as the presence of atopy, sputum eosinophil count, blood eosinophil count (BEC), fractional concentration of exhaled nitric oxide (FeNO), and any comorbidities (chronic sinusitis with nasal polyps (CRSwNP), atopic dermatitis, obesity, and urticaria). 13
IgE is the major immunoglobulin involved in allergic responses and parasitic infections.14–16 Its synthesis can occur via the T-helper 2 cell-driven process of class change. A close relationship between specific IgE and asthma may not be easy to determine because allergic sensitisation can involve several allergens with different clinical effects on the patient. 11 Additionally, inflammation sustained by IgE, as in occupational exposure to irritants, can occur in patients with asthma regardless of the presence of atopy. 17 These factors can influence how IgE is generated and its use as a biomarker. Because IgE-targeted therapy was the first biotherapy studied for use in asthma, IgE is the first specific biomarker for a biological drug that acts on the immediate hypersensitivity reaction by preventing the release of vasoactive mediators, transcription of cytokines, and synthesis of leukotrienes and prostaglandins. 18
Sputum eosinophilia (≥3%) is a reliable criterion that indicates eosinophilic inflammation of the airways. The BEC is a simple-to-obtain biomarker that accurately represents eosinophilic inflammation when elevated (≥300 cells/μL). 17 However, there is no correlation between the BEC and sputum eosinophil count, and the measurement of eosinophils in sputum is not commonly performed in clinical practice because it is unreliable and difficult to obtain. 17
An elevated BEC is associated with an increased risk of asthma exacerbations and poor control.19–21 Furthermore, the BEC can predict the response to inhaled corticosteroids (ICS) and anti-IL-5 therapy. 22 In addition, a high BEC is often related to a lower forced expiratory volume in 1 second (FEV1) in patients with asthma.23–25
The FeNO (a biomarker generated by nitric oxide synthesis after IL-13 stimulation) is used to assess T2 airway inflammation because it is non-invasive, simple to perform, and standardised.26–28 An elevated FeNO is related to airway eosinophilia, response to systemic or inhaled corticosteroids, and prediction of asthma exacerbations. 29 Moreover, the FeNO plays a key role in lung physiology; it acts as a bronchodilator and inflammatory mediator and is produced by the airway epithelium by nitric oxide synthase during the conversion of the amino acid L-arginine to L-citrulline during T2 inflammation. 30 An FeNO of <25 parts per billion (ppb) is considered normal in adult patients, whereas an FeNO of >50 ppb is high. An elevated FeNO is associated with bronchial hyperreactivity and the risk of asthma exacerbations.31–33 Previous studies have shown that a high FeNO (≥50 ppb) is correlated with asthma symptoms and asthma-related emergency room visits and can predict the response to ICS. 33 Interestingly, the combined presence of an elevated FeNO and elevated BEC is associated with significantly higher rates of severe exacerbation, suggesting that the combined measurement of these two biomarkers may help identify individuals at higher risk for exacerbations.34,35 Although there are many other biomarkers (such as eosinophil cationic protein, periostin, and serum eosinophil-derived neurotoxin), their current application is largely experimental and they are not yet routinely usable in clinical practice. 35
Biologic strategies for asthma: What clinical trials say
Five biological agents currently have FDA- and EMA-approved indications for the treatment of SA with allergic (omalizumab), eosinophilic (mepolizumab, reslizumab and benralizumab), and mixed atopic-eosinophilic phenotypes (high T2) or oral corticosteroid (OCS)-dependent asthma (dupilumab). 36 Recent clinical studies demonstrated that these agents are effective and have a similar safety profile; however, the agents were not identical in the inclusion criteria, study protocols, and measured outcomes (annualised exacerbation rates, FEV1, standardised asthma symptom scores, and the ability to reduce or wean systemic steroids). The results of the RCTs were then reanalysed and reinterpreted by patient subgroups, demonstrating enhanced responses. This has led to a rapidly growing body of literature on biological therapies for asthma; hence, it is necessary to have an in-depth understanding of biological therapies to make non-simple comparisons and considerations between various pharmacological options. Because of the large number of studies conducted on this subject, we will report only those deemed the most important and significant for therapy.
Omalizumab
Omalizumab is a recombinant humanised IgG1 anti-IgE monoclonal antibody (mAb) that binds to free-circulating IgE, preventing its binding to receptors on mast cells and basophils and blocking the release of histamine and other mediators.37,38 It is an adjunct treatment for patients over 6 years of age with moderate to severe allergic asthma (SAA) in the United States and SAA in Europe and for patients with at least one sensitisation to perennial aeroallergens and a serum IgE level of 30 to 1300 IU/mL in the United States and 30 to 1500 IU/mL in Europe. The dose is individualised and depends on the body weight and serum IgE level, ranging from 150 mg every 4 weeks (q4w) to 375 mg every 2 weeks (q2w). 38 Omalizumab is also indicated for the treatment of chronic spontaneous urticaria refractory to antihistamines, with a single recommended dose of 300 mg q4w. 39 Because this biologic has been available for clinical use for decades, a large body of evidence supports its efficacy and safety. For more than 2 years, numerous clinical trials have been conducted or are ongoing to evaluate the safety and efficacy of omalizumab for treatment of persistent SA. A double-blind, randomised phase II study conducted in 1999 involved 317 patients with moderate to severe uncontrolled asthma and a predicted mean FEV1 of 71%. 40 The results showed a significant reduction in asthma symptoms (47% and 49% in patients treated with low and high doses, respectively, compared with 24% in the placebo arm), with a simultaneous improvement in quality of life (QoL). The OCS dosage was halved in 78% of the patients treated with a high dose of omalizumab and in 57% in the low-dose arm compared with 33% in the placebo group. Furthermore, the ICS dosage was reduced by approximately 50% in 51% of patients in the high-dose group and in 49% of the low-dose patients compared with 38% in the control group. The promising results obtained from this study initiated the phase III clinical trials programme.39,41 These trials were randomised, double-blind, parallel-group, placebo-controlled, multicentre studies involving adolescent and adult patients with moderate to uncontrolled SAA. The design of the phase III studies was similar to that of the phase II study, but the drug was administered subcutaneously (unlike the intravenous administration used in the phase II study) at an individually adjusted dose based on body weight and the total serum IgE level at baseline. The results of these trials substantially confirmed the results of the phase II study. An RCT called INNOVATE, probably the most important phase III study of omalizumab, was conducted in 2005 and involved 419 patients with SAA. 42 Omalizumab was also effective in this study, leading to a 44% reduction in the rate of emergency visits and a 50% reduction in the rate of severe exacerbations. A subsequent pooled analysis of seven clinical studies involving 4308 patients revealed that patients undergoing treatment with omalizumab had a 38.3% reduction in the rate of exacerbations and a 47% reduction in emergency hospital visits compared with patients receiving placebo. 43 The same analysis showed that hospital admissions were reduced by 51% and emergency room visits by 60%. The QoL of patients with asthma, measured with the Asthma Quality of Life Questionnaire, was also significantly improved compared with the placebo group. Another pooled analysis highlighted a further important finding that omalizumab therapy significantly reduces the need for OCS bursts. 44 In a 32-week study of 400 patients treated with omalizumab add-on to optimised asthma therapy (OAT), the persistence of the anti-IgE response was assessed based on the physician’s Global Evaluation of Treatment Effectiveness rating. 45 Patients with OAT showed less persistence of response (18/28 (64.3%)) than those in the omalizumab group. Meanwhile, excellent and good Global Evaluation of Treatment Effectiveness ratings in the omalizumab arm were correlated with improvement in the rates of exacerbation (P < 0.001), severe exacerbations (P = 0.023), hospitalisations (P = 0.003), and the overall asthma control questionnaire score (P < 0.001). A subsequent subgroup analysis showed that the change in the mean OCS dose of patients treated with omalizumab at the end of 32 weeks of observation was significantly greater than that of patients in the OAT group (−45.0% vs. 18.3%, P = 0.002). 46 In addition, 62.7% of patients in the omalizumab group had reduced or stopped the use of OCS compared with 30.4% in the OAT arm (Table 1).
Evidence from clinical trials and real-life studies of omalizumab.
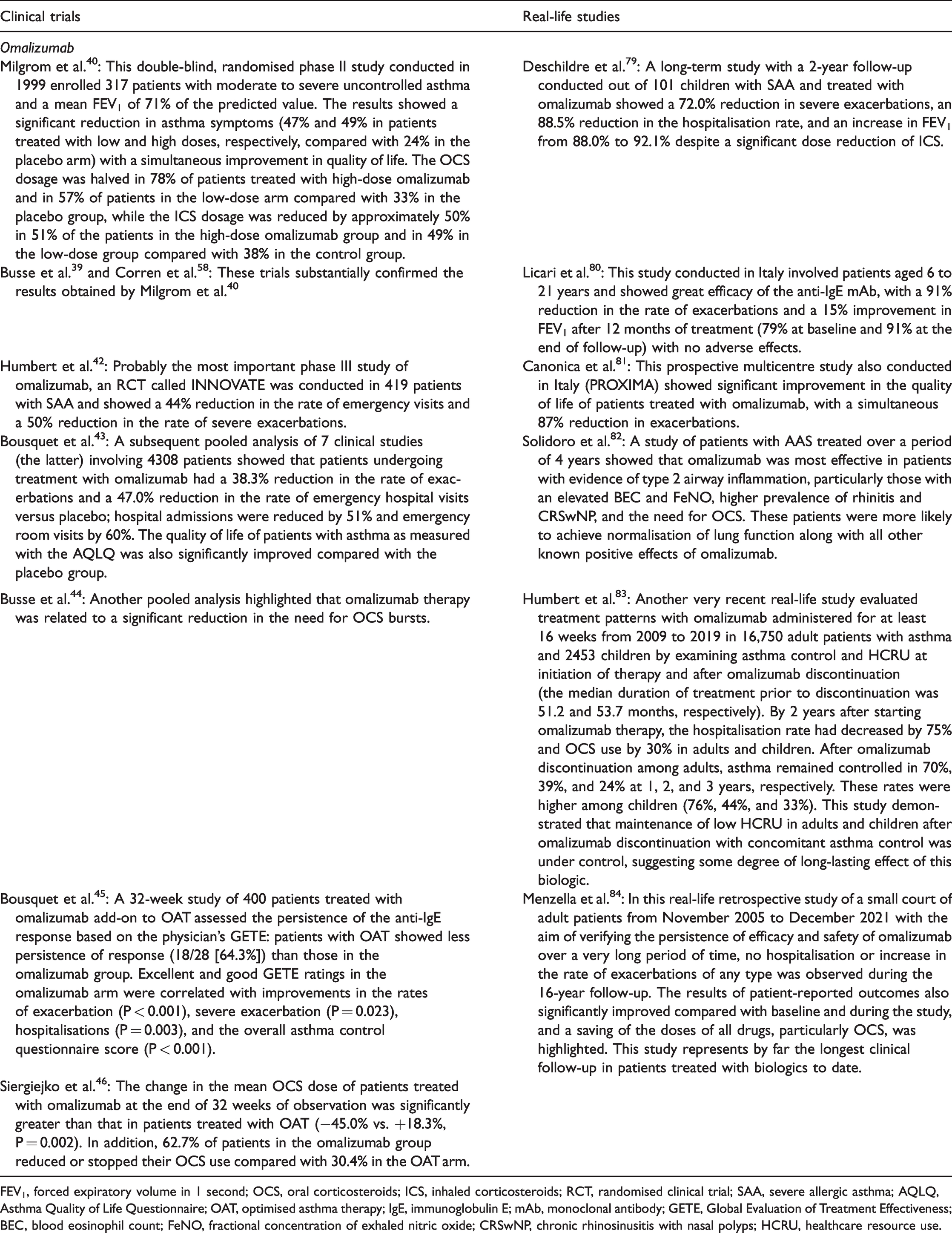
FEV1, forced expiratory volume in 1 second; OCS, oral corticosteroids; ICS, inhaled corticosteroids; RCT, randomised clinical trial; SAA, severe allergic asthma; AQLQ, Asthma Quality of Life Questionnaire; OAT, optimised asthma therapy; IgE, immunoglobulin E; mAb, monoclonal antibody; GETE, Global Evaluation of Treatment Effectiveness; BEC, blood eosinophil count; FeNO, fractional concentration of exhaled nitric oxide; CRSwNP, chronic rhinosinusitis with nasal polyps; HCRU, healthcare resource use.
Mepolizumab
Mepolizumab, an IgG1k mAb, was the first anti-IL-5 mAb approved for severe eosinophilic asthma (SEA). The results of early studies of this agent were unsatisfactory because of improper identification of potential responses; this mainly occurred because the baseline level of eosinophilic airway inflammation was not considered the most important criterion, leading to significant doubts regarding the real efficacy of this compound.47,48 However, positive results were achieved after anti-IL-5 mAb was administered to patients with SEA, leading to the phases II and III development programme. Numerous RCTs have indeed confirmed its efficacy in terms of reduction in asthma exacerbations, OCS-sparing effect, improvement in lung function, and increase in health-related QoL.49,50 The approved dosage of mepolizumab was chosen based on evidence from clinical trials of the dose interval efficacy and safety with mepolizumab in SA (DREAM), 49 as an adjunct treatment in patients with SA (MENSA), 50 and as a steroid-sparing agent (SIRIUS). 51 These RCTs demonstrated that 100 mg of mepolizumab administered subcutaneously had greater efficacy in patients with a BEC of greater than 150 to 300 cells/µL. Subsequent extension studies (COSMOS, 52 COLUMBA, 53 and COSMEX 54 ) confirmed the favourable long-term safety and tolerability profile of mepolizumab for up to 4.8 years (Table 2).
Evidence from clinical trials and real-life studies of mepolizumab.
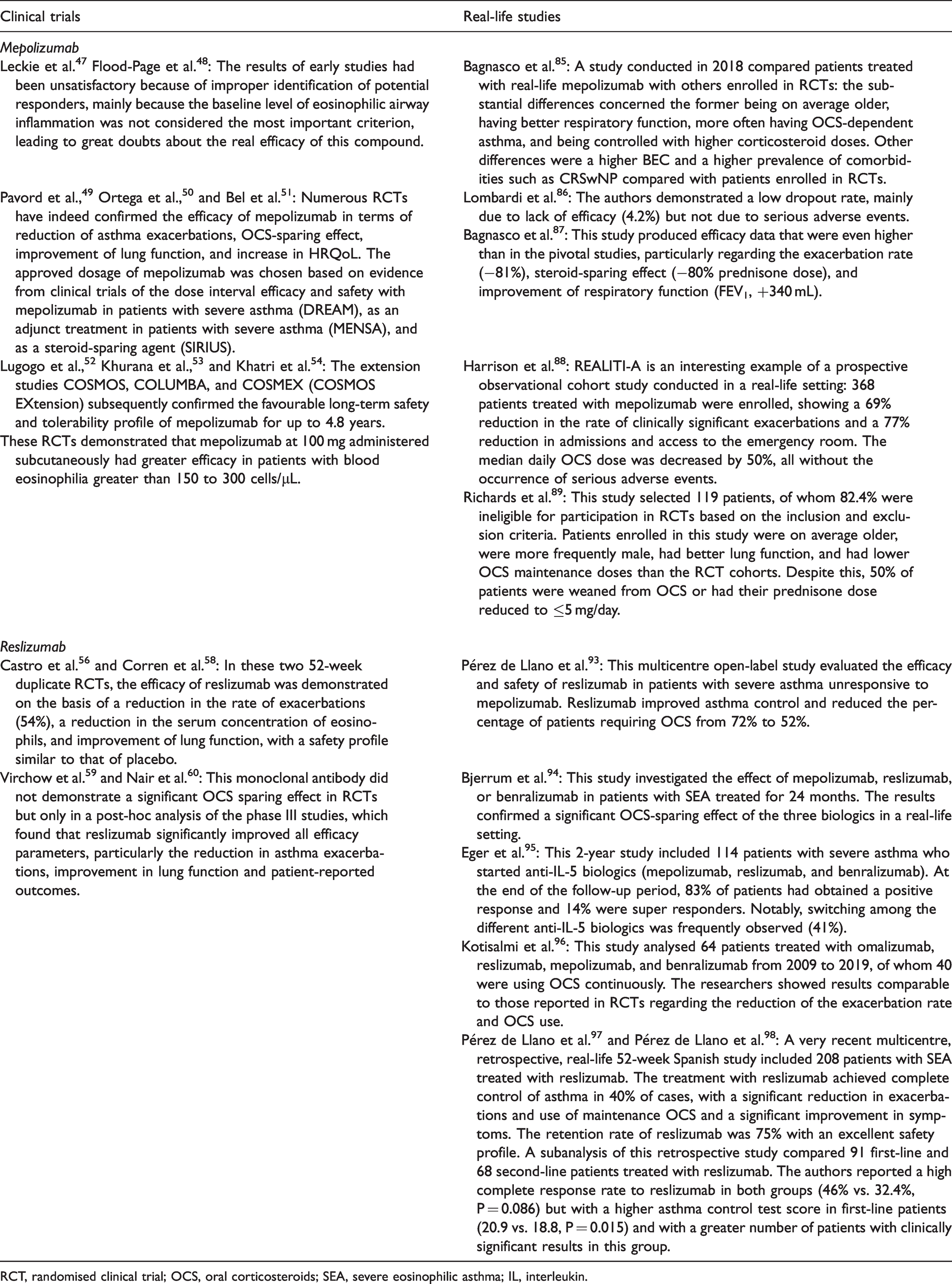
RCT, randomised clinical trial; OCS, oral corticosteroids; HRQoL, health-related quality of life; CRSwNP, chronic rhinosinusitis with nasal polyps; FEV1, forced expiratory volume in 1 second; BEC, blood eosinophil count.
Reslizumab
Reslizumab is a recombinant humanised IgG4 mAb to circulating IL-5. This mAb is administered intravenously at a dose based on the patient’s body weight (3 mg/kg) and is approved in many countries for the treatment of patients with SEA who have eosinophilia (≥400 eosinophils/μL). 55 Its efficacy was demonstrated by RCTs based on the reduction in the rate of exacerbations, serum concentration of eosinophils, and improvement in lung function. 56 In two 52-week duplicate RCTs, reslizumab reduced the rate of asthma exacerbations by 54% and had a safety profile similar to that of placebo.57,58 Unfortunately, it did not show a significant OCS-sparing effect in the RCTs but in a post-hoc analysis of the phase III studies. 59 The post-hoc analysis of these studies revealed that reslizumab significantly improved all efficacy parameters, particularly the reduction in asthma exacerbations, improvement in lung function, and patient-reported outcomes (Table 3). 60
Evidence from clinical trials and real-life studies of reslizumab.

RCT, randomised clinical trial; OCS, oral corticosteroids; SEA, severe eosinophilic asthma; IL, interleukin.
Benralizumab
Benralizumab is an IgG1 mAb that targets the α subunit of the IL-5 receptor, which activates a unique mechanism of antibody-mediated cellular cytotoxicity that leads to profound depletion of eosinophils and their precursors in blood and tissues through a completely different mechanism. 61 Benralizumab was developed for the treatment of SEA through several RCTs that confirmed its indisputable efficacy in terms of reducing asthma exacerbations and improving lung function, QoL, and overall asthma control.62,63 The phase III ZONDA study also showed a significant OCS-sparing effect as indicated by the 50% reduction in the median final OCS dose with respect to baseline. 64 Patients who had been enrolled in and completed the three main RCTs62–64 were then included in the phase III randomised extension study BORA. 65 The main objective of this 56-week trial was to evaluate the long-term efficacy and safety of benralizumab, with results indicating that its safety profile and tolerability were comparable to those of previous studies. The long-term open-label MELTEMI extension study confirmed the efficacy and safety of benralizumab for up to 5 consecutive years of treatment in patients with SEA. 66 In light of the growing need to establish an OCS tapering protocol, and given the significant efficacy of benralizumab in this sense, the PONENTE study was conducted. This study was an open-label multicentre trial of benralizumab in patients with severe steroid-dependent asthma. 67 The primary endpoint was to determine how quickly and safely the OCS dose could be reduced to a physiological level of ≤5 mg/day of prednisone or the equivalent. Another objective was to define the management of adrenal insufficiency and how to scale the OCS dose if adrenal insufficiency was present using a precise OCS dose-reduction algorithm. In the majority of patients (62.2%), it was possible to stop the OCS dose, and in 80.6% of the patients, the OCS could be discontinued or at least reduced to a daily dosage of <5 mg in the case of adrenal insufficiency. The study provided important practical information on the management of OCS tapering in patients with asthma treated with biologics and will be followed by further investigations in the near future (Table 4).
Evidence from clinical trials and real-life studies of benralizumab.
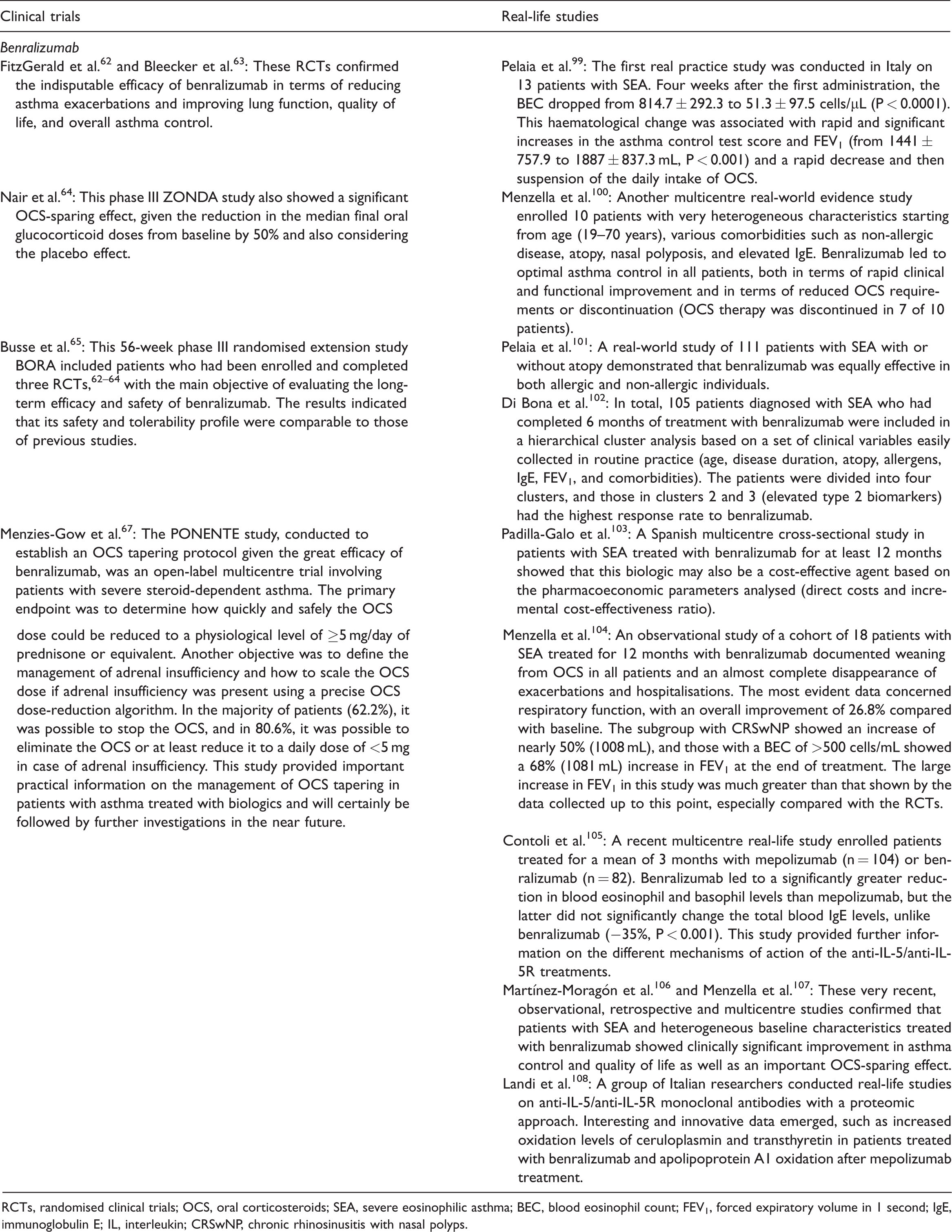
RCTs, randomised clinical trials; OCS, oral corticosteroids; SEA, severe eosinophilic asthma; BEC, blood eosinophil count; FEV1, forced expiratory volume in 1 second; IgE, immunoglobulin E; IL, interleukin; CRSwNP, chronic rhinosinusitis with nasal polyps.
Dupilumab
Dupilumab is a fully human IgG4 mAb that binds to the IL-4 receptor alpha subunit (IL-4Rα), shared by both IL-4 and IL-13 receptor complexes, to simultaneously block the signalling pathway of IL-4 and IL-13. 68 IL-4 and IL-13 play important roles in the induction and maintenance of T2 inflammation and in the pathogenesis of asthma and other atopic diseases, such as CRSwNP and atopic dermatitis. 69 The efficacy and safety of the subcutaneous administration of dupilumab for the treatment of moderate to severe asthma was primarily demonstrated by three clinical studies. The first was a phase IIa proof-of-concept study in adult patients with eosinophilic asthma (BEC of >300 cells/µL and sputum eosinophil concentration of >3%), 70 the second was a 6-month international multicentre phase IIb dose-ranging study, 71 and the third was a phase III RCT. 72 The second and third studies involved patients aged 12 years or older. In these studies, dupilumab was demonstrated to be effective in reducing the rate of exacerbations and improving asthma control compared with placebo. Furthermore, it improved lung function and decreased the FeNO. One notable aspect is that the dose-ranging study showed superior results for patients receiving dupilumab q2w compared with patients receiving dupilumab q4w, with no obvious differences between those treated with 200 mg q2w and those treated with 300 mg q2w. A subgroup analysis showed better results, especially for patients with ≥300 eosinophils/μL, although the drug was valid in the other two patient groups with a lesser effect. For example, FEV1 increased by approximately 400 mL among patients in the first group compared with patients in the group with lower blood eosinophilia. 71 A 52-week phase III RCT (LIBERTY ASTHMA QUEST) further confirmed the efficacy of dupilumab by showing a significant reduction in SA exacerbations, improved lung function, and better asthma control, especially in patients with higher biomarkers of T2 inflammation (BEC of >300 cells/µL and FeNO of >25 ppb). 72 A second pivotal phase III study (LIBERTY ASTHMA VENTURE) involving patients with severe steroid-dependent asthma revealed that treatment with 300 mg q2w reduced the rate of severe exacerbations and increased FEV1; in particular, it reduced the mean daily OCS dose by 70% compared with 42% in the placebo group. 73 In this study, transient eosinophilia was observed in approximately 14% of patients treated with dupilumab. The BEC thereafter returned to the baseline level before the end of the treatment period, and no patient had clinically relevant adverse events. 73 Subsequently, the open-label TRAVERSE extension study was conducted to evaluate the long-term safety and efficacy of dupilumab for an overall follow-up period of 148 weeks. The BEC returned to the baseline level by week 96, confirming that the increase was transient and without evidence of significant and superior adverse events compared with the parent studies. 74 Even in RCTs of CRSwNP and atopic dermatitis, small and transient increases in the BEC were observed compared with baseline, with a subsequent decrease similar to or below the baseline level at the end of the observation period.75–77 Conjunctivitis is another common adverse event that occurs predominantly in 3% to 14% of patients with atopic dermatitis treated with dupilumab compared with <1% to 8% of patients in the placebo group in phase III trials (Table 5). 78
Evidence from clinical trials and real-life studies of dupilumab.
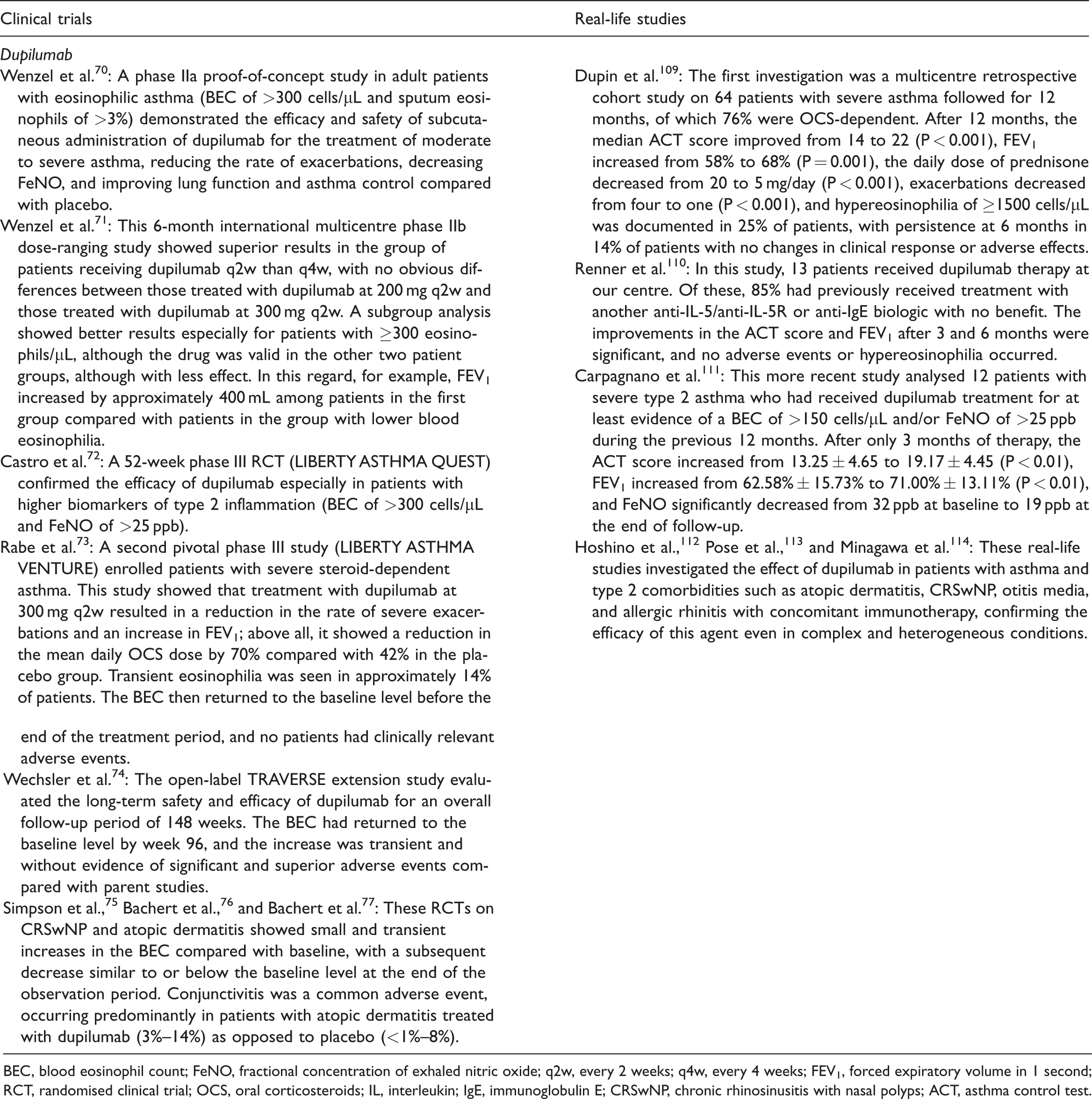
BEC, blood eosinophil count; FeNO, fractional concentration of exhaled nitric oxide; q2w, every 2 weeks; q4w, every 4 weeks; FEV1, forced expiratory volume in 1 second; RCT, randomised clinical trial; OCS, oral corticosteroids; IL, interleukin; IgE, immunoglobulin E; CRSwNP, chronic rhinosinusitis with nasal polyps; ACT, asthma control test.
Real-life studies: Translating evidence of clinical trials into practice
Since the approval of omalizumab for the treatment of moderate asthma to SAA in the United States in 2003 and for the treatment of SAA in Europe in late 2005, numerous studies have been conducted in real-life settings to evaluate the effectiveness and safety of omalizumab and, in subsequent years, all other biologics. Over time, this type of study has shown great heterogeneity regarding the patients enrolled and the conditions and duration of the treatments, which are much greater than those in RCTs. Hence, different data were obtained to compare controlled studies, significantly enhancing the knowledge about the MoAs of the different options and improving their use in clinical practice precisely because the patients examined were closer to the real treatment conditions. Although RWE studies have several advantages, they also have some limitations that must always be taken into consideration.
Omalizumab
Several RWE studies of omalizumab have been conducted. However, we will discuss only those deemed most interesting because it is impossible to report all the studies here. A long-term study with a 2-year follow-up involving 101 children with SAA treated with omalizumab showed a 72% reduction in severe exacerbations and an 88.5% reduction in the hospitalisation rate. At the same time, an increase in FEV1 from 88.0% to 92.1% was documented despite a significant ICS dose reduction. 79 Another RWE study of patients aged 6 to 21 years in Italy revealed the significant effectiveness of the anti-IgE mAb, with a 91% reduction in the rate of exacerbations and 15% improvement in FEV1 after 12 months of treatment (79% at baseline and 91% at the end of follow-up) with no adverse effects. 80 A prospective multicentre study also conducted in Italy (PROXIMA) showed a significant improvement in the QoL of patients treated with omalizumab, with a simultaneous 87% reduction in exacerbations. 81 Furthermore, a study of patients with SAA treated for a period of 4 years showed that omalizumab was most effective in patients with evidence of T2 airway inflammation, and particularly those with an elevated BEC and FeNO and a higher prevalence of rhinitis, CRSwNP, and the need for OCS. 82 These patients were more likely to achieve lung function normalisation along with all other known positive effects of omalizumab.
Another very recent real-life study evaluated treatment patterns with omalizumab administered to 16,750 adult patients with asthma and 2453 children for at least 16 weeks from 2009 to 2019 by examining asthma control and healthcare resource use at the initiation of therapy and after omalizumab discontinuation. 83 The median duration of treatment prior to discontinuation was 51.2 and 53.7 months, respectively. Two years after starting the omalizumab therapy, the hospitalisation rate had decreased by 75% and OCS use by 30% in both adults and children. After omalizumab discontinuation among the adults, asthma was controlled by 70%, 39%, and 24% at 1, 2, and 3 years, respectively. These rates were higher among children (76%, 44%, and 33%, respectively). This study demonstrated successful maintenance of low healthcare resource use in adults and children after omalizumab discontinuation with concomitant asthma control, suggesting some degree of a long-lasting effect of this biologic. Another real-life retrospective study was conducted on a small cohort of adult patients from November 2005 to December 2021 to verify the persistence of the effectiveness and safety of omalizumab over a very long period. No hospitalisation or exacerbations of any type were observed during the 16-year follow-up. The patient-reported outcomes also significantly improved compared with baseline, and lowered doses of all drugs, especially OCS, were achieved during the study. This study represents by far the longest clinical follow-up in patients treated with biologics to date (Table 1). 84
Mepolizumab
Numerous RWE studies of mepolizumab have not only confirmed RCTs of mepolizumab but have sometimes surpassed them. A study conducted in 2018 compared patients treated with mepolizumab in the real-life setting with others enrolled in RCTs. 85 The substantial differences were that patients in the real-life setting were, on average, older; had better respiratory function; had OCS-dependent asthma; and maintained asthma control with higher corticosteroid doses. Other differences were a higher BEC and a higher prevalence of comorbidities, such as CRSwNP, compared with patients enrolled in RCTs. The same Italian research group mentioned previously also conducted two other interesting multicentre studies on the safety and effectiveness of mepolizumab in a real-life setting. In the first study, the authors demonstrated a low dropout rate, mainly due to lack of efficacy (4.2%) but not due to serious adverse events. 86 The results of the second study were superior to the pivotal trials, particularly regarding the exacerbation rate (−81%), steroid-sparing effect (−80% prednisone dose), and improvement of respiratory function (FEV1 +340 mL). 87 REALITI-A is an interesting example of a prospective observational cohort study conducted in a real-life setting. 88 The study involved 368 patients treated with mepolizumab, and a 69% reduction in the rate of clinically significant exacerbations and a 77% reduction in admissions and access to the emergency room were observed. Moreover, the median daily OCS dose decreased by 50% without the occurrence of serious adverse events. Another RWE study recruited 119 patients, 82.4% of whom were ineligible for inclusion in RCTs based on the inclusion and exclusion criteria. Patients enrolled in this study were on average older, were more frequently male, had better lung function, and had lower OCS maintenance doses than the RCT cohorts. Despite this, 50% of patients were weaned from OCS or had their prednisone dose reduced to ≤5 mg/day. 89 Other real-life studies have confirmed the high effectiveness of mepolizumab regardless of the presence of comorbidities and baseline BEC in comparison to other therapeutic options, including bronchial thermoplasty (Table 2).90–92
Reslizumab
Fewer studies have focused on reslizumab than on the above-mentioned agents because reslizumab is organic and not marketed in all countries. A multicentre open-label study evaluated the effectiveness and safety of reslizumab in patients with SA unresponsive to mepolizumab. 93 Reslizumab improved asthma control and reduced the percentage of patients requiring OCS from 72% to 52%. Several comparative studies were then conducted between anti-IL-5/anti-IL-5R and anti-IgE treatments. One study investigated the effects of mepolizumab, reslizumab, or benralizumab in patients with SEA treated for 24 months. The results confirmed a significant OCS-sparing effect of the three biologics in a real-life setting. 94
In a 2-year study, 114 patients with SA who started anti-IL-5 biologics (mepolizumab, reslizumab, and benralizumab) were evaluated. 95 At the end of the follow-up period, 83% of the patients had a positive response, with 14% being super responders. One notable aspect is that switching between the different anti-IL-5 biologics was frequently observed (41%). Another real-life study evaluated 64 patients treated with omalizumab, reslizumab, mepolizumab, and benralizumab from 2009 to 2019, and 40 of these patients used OCS continuously. 96 Researchers have shown results comparable to those reported in RCTs regarding the reduction in the exacerbation rate and OCS use. A very recent multicentre, retrospective, real-life 52-week Spanish study included 208 patients with SEA treated with reslizumab. 97 Complete control of asthma was achieved in 40% of the patients, with a significant reduction in exacerbations and use of maintenance OCS and a significant improvement in symptoms. The retention rate of reslizumab was 75%, and the safety profile was excellent. A subanalysis of this retrospective study compared 91 patients undergoing first-line treatment with reslizumab and 68 patients undergoing second-line treatment. 98 The authors reported a high complete response rate to reslizumab in both groups (46.0% vs. 32.4%, P = 0.086), but with a higher asthma control test (ACT) score in the patients undergoing first-line treatment (20.9 vs. 18.8, P = 0.015) and more patients with clinically significant results in this group (Table 3).
Benralizumab
Benralizumab is an anti-IL-5R mAb that has been available since 2019, and many RWE studies conducted over a short period of time have confirmed the great interest aroused by this biological with a peculiar MoA. The first real-practice study on benralizumab was conducted in Italy and involved 13 patients with SEA. 99 Four weeks after the first administration, the BEC dropped from 814.7 ± 292.3 to 51.3 ± 97.5 cells/μL (P < 0.0001). This haematological change was associated with rapid and significant increases in the ACT score and FEV1 (from 1441 ± 757.9 to 1887 ± 837.3 mL; P < 0.001) and a rapid decrease and suspension of the daily intake of OCS. Another multicentre RWE study enrolled 10 patients aged 19 to 70 years with very heterogeneous characteristics and various comorbidities such as non-allergic disease, atopy, nasal polyposis, and elevated IgE. 100 Overall, benralizumab led to optimal asthma control in all patients, both in terms of rapid clinical and functional improvement and in terms of reduced systemic steroid requirements or discontinuation (OCS therapy was discontinued in 7 of 10 patients). A subsequent real-world study of 111 patients with SEA, with or without atopy, demonstrated that benralizumab was equally effective in both allergic and non-allergic individuals. 101 Furthermore, to study the response of benralizumab in patients with different phenotypes from the perspective of precision medicine, 105 patients diagnosed with SEA who had completed 6 months of treatment with benralizumab were included in a hierarchical cluster analysis based on a set of clinical variables easily collected in routine practice (age, disease duration, atopy, allergens, IgE, FEV1, and comorbidities). 102 The patients were divided into four clusters, and the patients in clusters 2 and 3 (elevated T2 biomarkers) had the highest response rate to benralizumab. A Spanish multicentre cross-sectional study of patients with SEA treated with benralizumab for at least 12 months revealed that this biologic may also be a cost-effective agent based on the pharmacoeconomic parameters analysed (i.e., direct costs and incremental cost-effectiveness ratio). 103 In an observational study involving a cohort of 18 patients with SEA treated with benralizumab for 12 months, the investigators documented the weaning of all patients from OCS, resulting in an almost complete disappearance of exacerbations and hospitalisations. 104 The most evident data were associated with respiratory function, with an overall improvement of 26.8% compared with baseline. At the end of treatment, the patient subgroup with CRSwNP showed an increase in FEV1 of approximately 50% (1008 mL), and patients with a BEC of >500 cells/mL showed an increase in FEV1 of 68% (1081 mL). The large increase in FEV1 in this study was much greater than the data collected up to this point, especially compared with RCTs. A recent multicentre real-life study enrolled patients treated with either mepolizumab (n = 104) or benralizumab (n = 82) for a mean of 3 months. 105 Benralizumab led to a significantly greater reduction in the BEC and basophil count than did mepolizumab, but the latter did not significantly change the total blood IgE concentration, unlike benralizumab (−35%, P < 0.001). This study provided further information on the different MoAs of anti-IL-5/IL-5R treatments. Other very recent observational studies, retrospective studies, and multicentre studies confirmed that patients with SEA and heterogeneous baseline characteristics treated with benralizumab showed clinically significant improvement in asthma control, QoL, and OCS-sparing effect.106,107 To identify new biomarkers with potentially predictive characteristics, a group of Italian researchers conducted real-life studies on anti-IL-5/anti-IL-5R mAbs using a proteomic approach. They found interesting and innovative data, such as increased oxidation levels of ceruloplasmin and transthyretin in patients treated with benralizumab and apolipoprotein A1 oxidation after mepolizumab treatment (Table 4). 108
Dupilumab
Dupilumab is chronologically the last biologic introduced for the treatment of asthma. Although the drug is arousing significant interest, few studies to date have been conducted in a real-life context, and some doubts regarding its safety profile still need to be clarified. The first investigation was a multicentre retrospective cohort study of 64 patients with SA, 76% of whom were OCS-dependent, who were followed up for 12 months. 109 At 12 months (end of treatment), the median ACT score improved from 14 to 22 (P < 0.001), FEV1 increased from 58% to 68% (P = 0.001), and the daily dose of prednisone dropped from 20 to 5 mg/day (P < 0.001). In addition, the number of exacerbations decreased from four to one (P < 0.001). Furthermore, hypereosinophilia (BEC of ≥1500 cells/µL) was documented in 25% of the patients, with persistence in 14% of the patients at 6 months and no changes in the clinical response or adverse effects. In another RWE study, 13 patients received dupilumab therapy at our center. 110 Of these patients, 85% had previously received treatment with another anti-IL-5/anti-IL-5R or anti-IgE biologic with no benefit. The improvements in the ACT score and FEV1 after 3 and 6 months were significant, and no patients developed adverse events or hypereosinophilia. A more recent study involved 12 patients with severe T2 asthma with a BEC of >150 cells/mL and/or FeNO of >25 ppb who had received dupilumab treatment. 111 After 3 months of therapy, the ACT score increased from 13.25 ± 4.65 to 19.17 ± 4.45 (P < 0.01), the FEV1 ranged from 62.58% ± 15.73% to 71.00% ± 13.11% (P < 0.01), and the FeNO significantly decreased from 32 ppb at baseline to 19 ppb at the end of follow-up. This study demonstrated more rapid improvement in asthma symptoms, FEV1, and FeNO compared with randomised trials at only 3 months from treatment onset. Other real-life studies have investigated the effect of dupilumab in patients with asthma and T2 comorbidities, such as atopic dermatitis, CRSwNP, otitis media, and allergic rhinitis with concomitant immunotherapy, confirming the effectiveness of this agent even in complex and heterogeneous conditions (Table 5).112–114
Advantages and disadvantages of real-world studies compared with clinical trials
The advent of precision or personalised medicine has led to the increasingly rapid development of biologics and their use in SA. There has been a longstanding debate on the importance of real-life studies and the interpretation of their results, which are often very different to obtain from clinical trials. Approval of new drugs always requires positive data on the efficacy–safety ratio: the extent to which the benefit is greater than a hypothetical harm is defined by RCTs. 115 Following the market launch of a new drug, its impact in clinical practice needs to be assessed. The ‘efficacy–effectiveness gap’ concept describes any discrepancies and provides complementary data on efficacy and efficacy. RWE studies are therefore crucial to obtaining this important information and how the drug works in practice (effectiveness). 116 Despite the already large and rapidly growing body of evidence on the efficacy of biologics, there is still a lack of detailed information on how mAbs are used in clinical practice. Specifically, there are still no reliable data on the number of patients who continue, interrupt, and switch from an initial biological to another option. RWE studies can help to answer these and other questions. In this context, great support is also provided by national and regional registries for SA, which is important because such support is considerably limited by the lack of information sharing between the registries. This situation has improved since the establishment of large databases, such as the International Severe Asthma Registry (http://isaregistries.org/) and the CHRONICLE study (United States).117,118 The huge amount of data provided by these programmes is fundamental and will be even more so in the near future, given the growing complexity of the asthma treatment landscape due to the number of mAbs available and the absence of head-to-head studies. These data are also useful in supporting decision-making in difficult situations, such as when a single patient is eligible for more than one biological option. The most important aspect of RCTs is that they are designed with great rigidity and solidity (with the presence of a control group and randomised patient selection) to accurately demonstrate that the studied drug provides positive clinical results. The rules for transitioning from proof-of-concept phase I or phase II studies to larger phase III studies are very strict, and they guide the development up to the registration of the drug for the defined indication. RCTs are needed to define the target population of a drug and its final indication with the highest precision. After the pivotal studies, secondary and pooled analyses are used to evaluate patient subgroups to identify the best responders and other specific conditions. Despite their central role in drug development, clinical trials suffer from some notable limitations (Figure 1). The most evident is that patients are selected according to restrictive inclusion and exclusion criteria, which leads to select groups that do not always reflect the patients who are indeed eligible for a biologic, with heterogeneous characteristics considered exclusion criteria for pivotal studies (e.g., smoking habit, advanced age, comorbidities, and previous treatments). The rigidity of clinical protocols increases adherence to therapies, 119 which does not occur at this level in real practice, leading to an impact on asthma control that must be considered regardless of the effectiveness of the investigated agent. 120 Another limitation of clinical studies is the duration, which generally does not exceed 52 weeks except in extension studies, in which the duration may even reach 96 weeks (as in the recent TRAVERSE study on dupilumab). In any case, these relatively short follow-up durations reduce the chances of not only highlighting the long-term adverse effects but also demonstrating the sustained efficacy of the investigated biological from the perspectives of both the clinical response and respiratory function or other parameters (Figure 1). These limits can be overcome by real-life studies, which certainly have important weaknesses but can often provide more realistic information because of the possibility of examining patients with characteristics that are considerably more heterogeneous than those of RCTs and are therefore much closer to clinical practice. The duration of real-life studies is highly variable and leads to follow-up periods that are often immensely longer than those of clinical trials, even reaching up to 16 years of observation, as in the recent study on omalizumab discussed above. 84 This allows us to overcome the duration-related limitations of RCTs. RWE studies evaluate patients who do not meet the inclusion criteria for clinical trials and would often be excluded because of characteristics such as young or advanced age, ethnicity, habits such as tobacco smoking, and comorbidities. Because of the presence of some characteristics such as CRSwNP associated with high dependence on OCS and T2 biomarkers, some of these studies have shown better results than RCTs in terms of asthma control, improvement in respiratory function, and OCS-sparing effect.82,104 Other advantages of real-life studies are the possibility of obtaining data on the clinical profile of potential responders and non-responders to biologics, causes of dropout, and causes of therapeutic switches/shifts (Figure 1). Dropout and therapy changes are often due to inaccurate patient selection or the absence of predictive biomarkers. In this regard, we have seen that some RWE studies are beginning to provide interesting evidence.99–108 In the context of national and international registries and large databases, RWE studies can go beyond one of their most significant limitations, which is the low number of patients examined.117,118 Big data obtained from networks and registers will also allow us to define alternative treatment schemes and dosages, but it is currently necessary to refer to those available.

Pros and cons of clinical trials and real-life studies.
Only two mAbs (omalizumab and mepolizumab) are currently approved for SA in children aged 6 years and older. There is no indication for dupilumab yet, but the data are being published. Numerous paediatric data are available for omalizumab but not mepolizumab, for which extrapolation from adult studies constitutes the bulk of our information. In general, there are fewer studies involving children, and the extrapolation of the data from adult studies does not assume that the data completely overlap. 119 For these reasons, RWE studies will also be able to support research in this area, with the added benefit of evaluating long-term effectiveness and safety.
The main limitation of RWE studies is the lack of randomisation. This reduces the internal validity of the data and, sometimes, the quality of the data collected. Because these studies often have a retrospective design, they may be intrinsically subject to distortions such as sampling bias, recall bias, incomplete data, and variations in disease management.120–122 Several statistical approaches have been developed to correct these different biases, even if the above-mentioned structural limitations prevent the accuracy and reliability of the data in RWE studies from being comparable to those obtained in RCTs owing to the superior methodological rigour of RCTs. 123 The application of tools such as the Grading of Recommendations Assessment, Development and Evaluation (GRADE) can increase the level of quality that should ideally be achieved in real-life experiences and RCTs. The GRADE working group developed this system to assess the certainty of the evidence of the effects and the strength of the recommendations. The system uses consolidated methods that support the use of evidence in healthcare decision-making. 124 Other comparative tools have recently been introduced to support the quality of observational studies on asthma, such as the Real Life Evidence Assessment Tool (RELEVANT) and the Cochrane Risk of Bias in Non-Randomised Studies of Interventions (ROBINS-I).125,126 These tools improve the identification of sufficiently strong evidence (with a lower risk of bias) to raise the level of evidence of RWE and pragmatic studies. To bridge the gap between RCTs and RWD, a technique called ‘target trial emulation’ was introduced to mitigate the limitations of real-life studies.127–129 This system uses observational data under the conditions in which they are applied. When it is not possible to emulate a placebo-controlled study in the target trial, patients who meet the inclusion criteria for the corresponding clinical trial are selected and assigned to the trial strategies consistent with their baseline data, modifying them based on the appearance of any distortions. The target trial approach can be especially advantageous for improving the quality of big data.118,119
Conclusion
Based on the discussions presented herein, the often different but complementary results between clinical studies and real-life experiences confirm the need for both types of studies. It is desirable that both types of studies be conducted with the greatest possible rigour to obtain high-quality data that can provide valuable information for clinicians in an increasingly complex and varied scenario due to the rapidly increasing availability of therapeutic options and the enormous amount of information available. As discussed, the gap between clinical and real-life studies is becoming narrower because of the greater methodological rigour with which the former are often conducted and the techniques that raise the quality of the data and evidence provided by them. In light of the increasing importance of RWE studies in healthcare decisions, having in-depth knowledge of this almost endless field and understanding the advantages and limitations of both kinds of studies can support clinicians in the difficult management of patients with severe refractory asthma. This takes on even greater importance given the availability of multiple therapeutic options and the lack of direct head-to-head comparisons, resulting in an ever-increasing effort in identifying the right biologic for the right patient.
Footnotes
Author contributions
FM conceptualised and planned the article and wrote the first draft of the manuscript. AB, MF, AF, LC, CD, and ST contributed to, reviewed, and edited the manuscript. MR contributed to, reviewed, and revised the final work. All the authors read and approved the final version.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FM received research funding as the principal investigator from AstraZeneca, Chiesi Farmaceutici, Novartis, and Sanofi and fees as speaker/lecturer from AstraZeneca, Chiesi Farmaceutici, GlaxoSmithKline, Novartis, and Sanofi. The other authors declare that they have no conflicts of interest.
Ethics
Ethics approval was not required because of the nature of this study (narrative review).
Funding
This manuscript received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.