
Abstract
Objective
The primary goals of this research were to analyze the relationship between ABO blood types and the severity of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and investigate the effect of vaccination in Iraq.
Methods
Data and outcomes were gathered from the medical records of 200 patients. Patients were categorized by blood group and vaccination status in the analysis.
Results
In total, 200 hospitalized patients (125 men and 75 women) with confirmed SARS-CoV-2 infection and blood group (ABO) and clinical data were enrolled. Of the 200 patients, 155 (77.5%) were vaccinated against SARS-CoV-2. The results illustrated that 25 patients died, which might have been attributable to a lack of vaccination or older age. Our analysis revealed that blood group O individuals were much less likely to be infected by SARS-CoV-2 than non-O subjects, whereas blood group A individuals carried a higher risk of infection.
Conclusions
Our findings illustrated that immunization significantly reduces COVID-19 risk across all age groups, but there has been an increase in the number of cases because of decreased vaccine efficacy in older patients and persons with comorbidities. However, 45% vaccination coverage lowered the outbreak’s peak.
Keywords
Introduction
In December 2019, a pneumonia outbreak occurred in Wuhan, China and rapidly spread globally. The World Health Organization termed the illness coronavirus disease 2019 (COVID-19), which is caused by the beta-coronavirus severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). 1 The extensive spread of COVID-19 occurred through human-to-human transmission, which occurred among symptomatic patients as well as asymptomatic and pre-symptomatic infected people. 2 Fever, cough, fatigue, anorexia, myalgia, and diarrhea are the most common symptoms of COVID-19 in humans. In the week following the onset of symptoms, the condition frequently worsens from mild to severe illness.3,4
Some epidemiological and clinical variables of a community have been demonstrated to influence the risk of COVID-19 and increase the risk of severe illness. Age, sex, and several chronic disorders including heart disease and diabetes are the main risk variables.5,6 Although elderly patients are predisposed to COVID-19, multiple risk factors have been identified. In addition, cases of severe infection have been reported in healthy people. 7 However, the biological indicators predictive of the occurrence of COVID-19 or its progression have not been identified. 8 Meanwhile, several elements (host, viral, and environmental factors) were proposed to explain the COVID-19 clinical phenotype. 9 In light of these findings, investigations assessing the relationships of blood groups, SARS-CoV-1, Plasmodium falciparum, Helicobacter pylori, Norwalk virus, hepatitis B virus, and Neisseria gonorrhoeae with COVID-19 susceptibility and severity have been conducted. 8
Carbohydrate epitopes on the surface of human cells comprise the ABO blood groups discovered by Landsteiner. The trisaccharide moieties GalNAc1–3-(Fuc1,2)-Gal- and Gal1–3-(Fuc1,2)-Gal- are determinants of antigenicity for the A and B blood groups, respectively, whereas Fuc1,2-Gal- is the antigenic determinant for blood group O. Although blood groups are inherited genetically, environmental variables can affect which blood groups present in a population are passed to the next generation. ABO blood groups have been linked to the susceptibility to viral infection. For example, the susceptibility to Norwalk virus and hepatitis B infection has been linked to the blood type. 10 It was also discovered that people with blood group O were less likely to contract the SARS coronavirus. 11 Therefore, the association of COVID-19 susceptibility with ABO blood groups was explored in this study.
Materials and methods
Data collection
The data of the clinical study were obtained from Al Karama Teaching Hospital (Baghdad, Iraq) to investigate the relationship between blood groups and COVID-19. Patients with a confirmed diagnosis of COVID-19 by quantitative reverse transcription polymerase chain reaction (RT-qPCR) using nasopharynx swab samples who had clinical and blood group (ABO and AB) data were eligible for enrollment. The study was approved by the ethics committee of Dijlah University College (approval date: February 2022), and the requirement for informed consent was waived. A blood test was used for both the clinical and laboratory investigations. The patients’ case report forms were used to collect information as well as blood group, sex, age, hospital ward, and disease outcome data. In this study, we followed the relevant EQUATOR guidelines for reporting observational studies, and all patient details were de-identified. 12
The patients were divided into groups by blood group, age, vaccination status, and hospital ward to assess their relationships with the outcomes of COVID-19 (recovered or dead).
Results and Discussion
Data were collected from 200 patients, including 125 men and 75 women.
Regarding the association between vaccine reactogenicity and ABO blood groups, it was observed that people with blood group A have a higher risk of COVID-19, whereas those with blood group O have a lower risk of contracting the virus. 13 However, the study revealed no link of vaccine reactogenicity with ABO blood groups for either available vaccine. However, people with various ABO blood groups exhibit varying degrees of reactogenicity to immunization by RNA vaccines developed by Pfizer and Sinopharm. 14 Individuals with blood group A experienced more severe adverse effects than those with blood group O, and the extent of reactogenicity appeared to be linked to the blood group, as presented in Table 1 and Figure 1.
Sex, age, blood group, and vaccination status of the cohort.

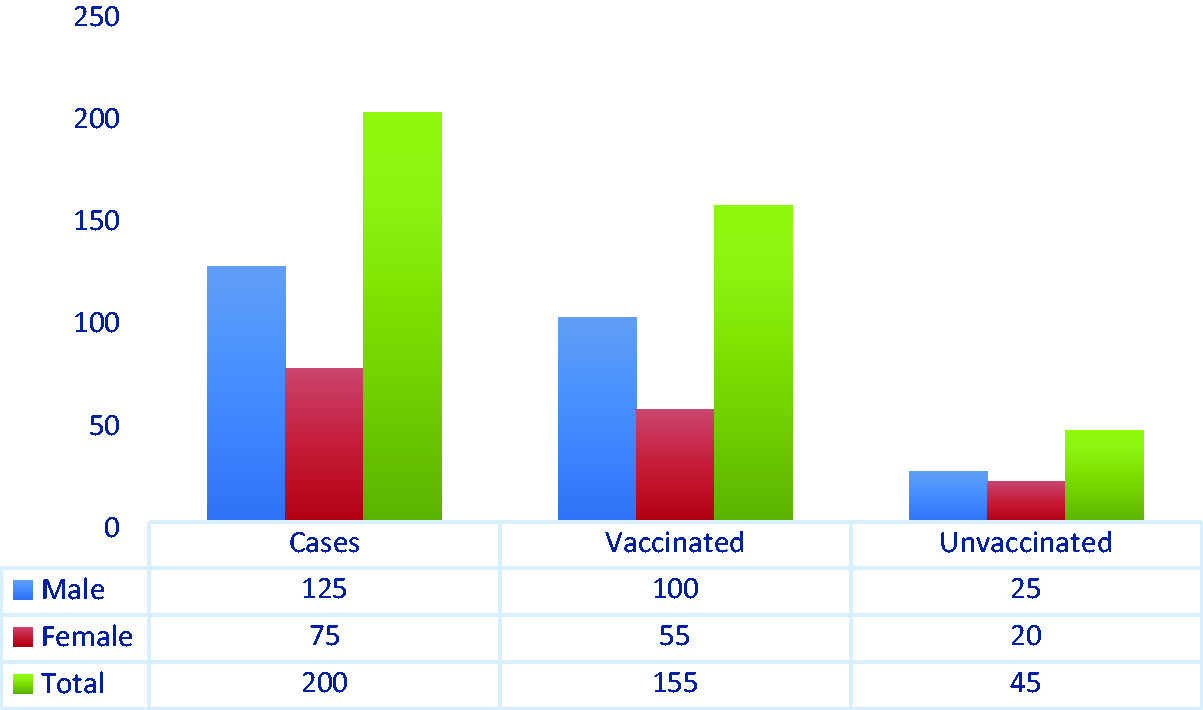
Vaccinated and unvaccinated patients with coronavirus disease 2019.
The frequencies of blood types in the vaccinated and unvaccinated groups are presented in Table 1 and Figure 2.
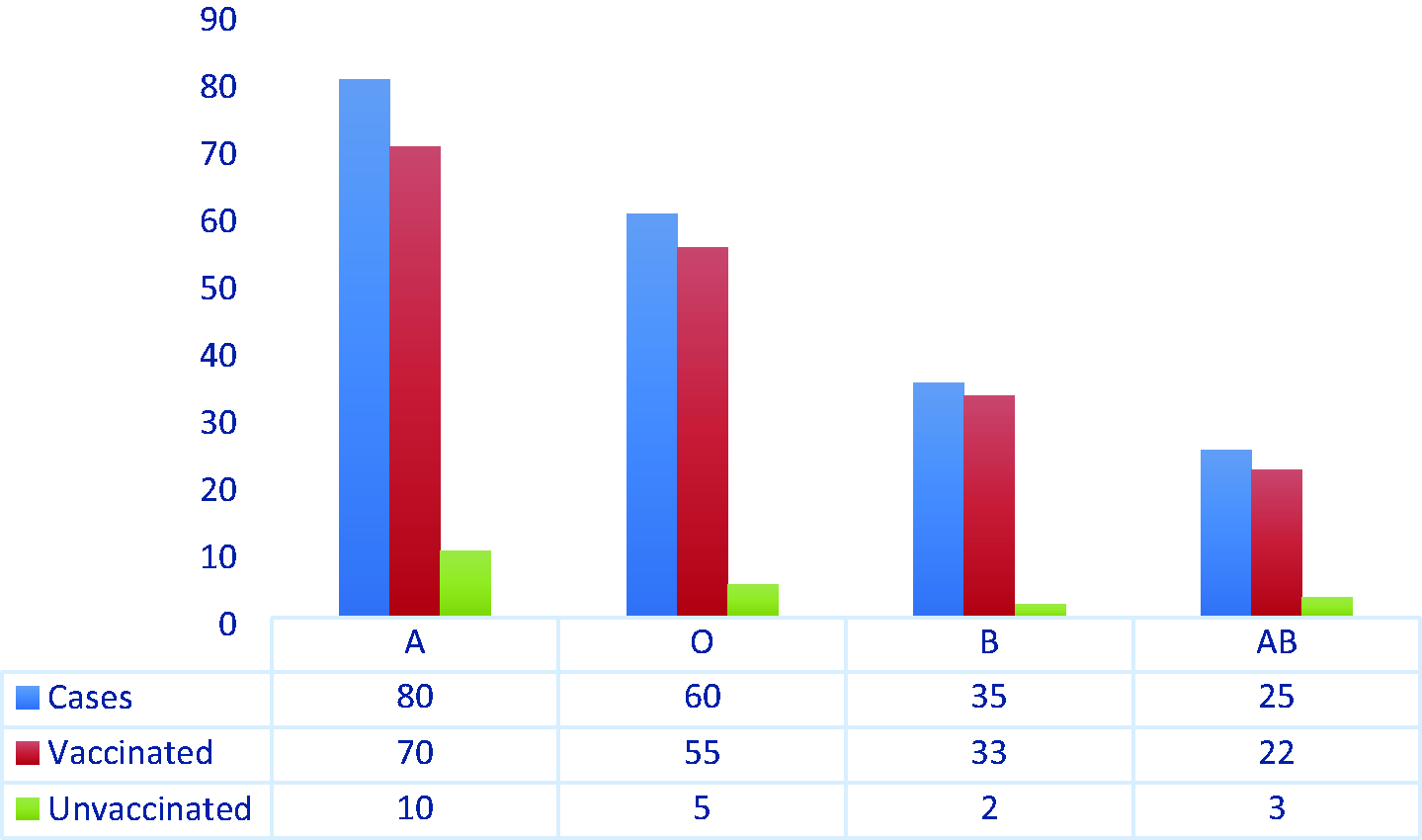
Distribution of blood groups among patients with coronavirus disease 2019.
Age and sex
The results suggest that blood groups are linked to the clinical outcomes of COVID-19. Meanwhile, the results revealed no major relationship between sex and the outcome of COVID-19 results. The results identified a substantial relationship between age and the outcome of COVID-19, as the risk of death was higher among older patients (Figure 3). This discovery is perhaps unsurprising given that elderly people have higher rates of diabetes, heart disease, hypertension, and chronic pain, which are comorbidities of respiratory disease and disorders that are related to a weakened immune system. 15 In addition, there was a strong link between the ward of hospitalization and disease outcome. Specifically, the probability of mortality was higher among patients admitted to the ICU, CCU, and emergency ward. In addition, we noticed that patients who did not have chronic diseases stayed in the hospital to receive treatment. Specifically, some patients were hospitalized for 1 to 3 days, whereas others stayed for 1 to 2 weeks. Meanwhile, patients who were hospitalized for 1 to 2 months were admitted to the ICU because they did not receive treatment in the first few days of infection. For patients with concomitant chronic diseases, the duration of hospitalization typically ranged from 1 to 2 months, although some patients who died had a shorter hospital stay (Table 1).
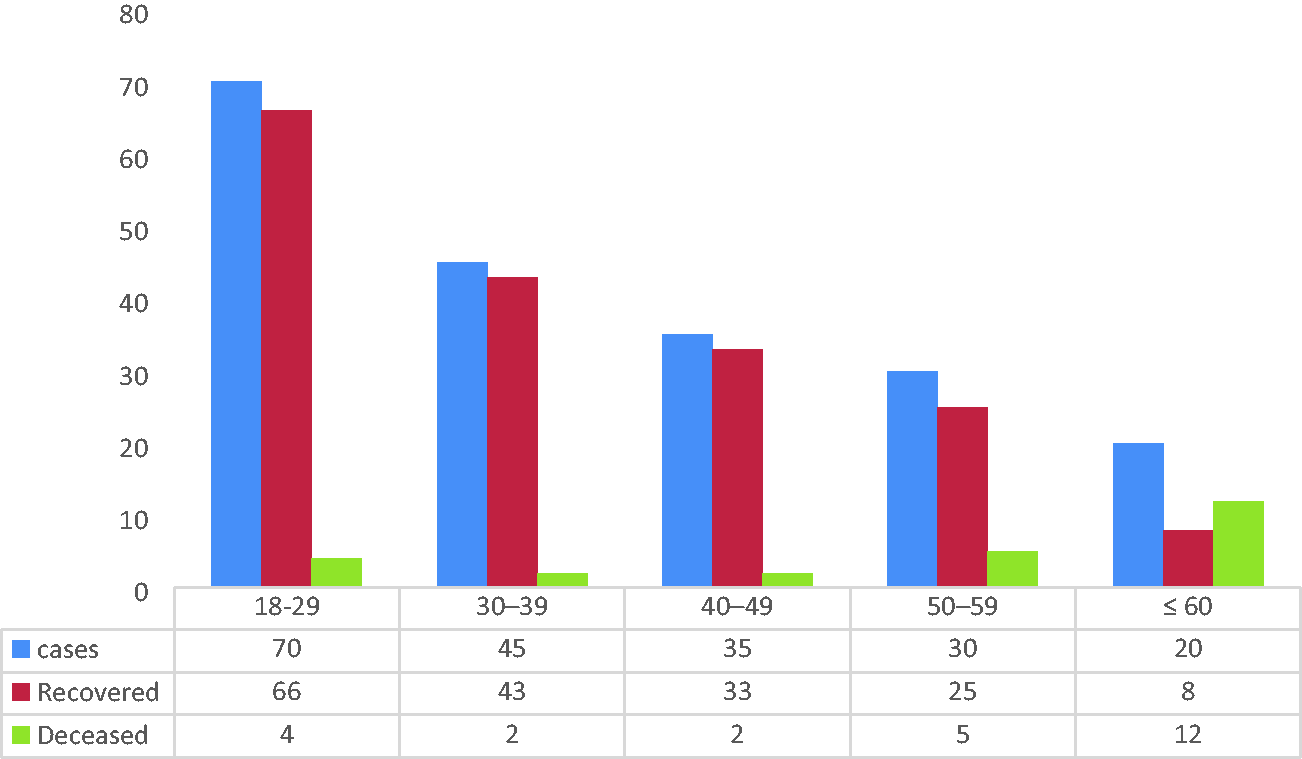
Outcomes (recovery or death) among patients with coronavirus disease 2019 categorized by age.
As presented in Figure 3, 200 samples were obtained from COVID-19–infected patients.
Clinical symptoms with blood groups
The discovery of risk variables linked to SARS-CoV-2 infection and outcomes has become a research priority because of the severity of the disease, which is usually unanticipated. Following the earliest findings in the literature on the link between COVID-19 and ABO blood groups, a number of studies investigated whether ABO blood groups were linked to the risk of COVID-19, the severity of the disease, and the risk of disease-related mortality. 16
At the beginning of the infection, fever, dry cough, dyspnea, lethargy, myalgia/arthralgia, and cold are the most common symptoms. Less common symptoms include earache, hemoptysis, headache, nausea or vomiting, chest discomfort, diarrhea, loss of taste, sputum production, and loss of smell.
Compared with individuals without diabetes, patients with diabetes had higher white blood cell, neutrophil, and lymphocyte counts and higher C-reactive protein and blood urea nitrogen levels. They also had lower red blood cell counts and hemoglobin levels.
Excluding pharyngeal exudate, which was most frequently observed among patients with blood group A, clinical symptoms were more frequently observed in blood group O patients than in those with blood group A or B. Only patients with blood group O experienced hemoptysis, jaundice, abnormal lung auscultation, and hepatomegaly, indicating that anti-A antibodies from patients with blood group O are more protective than those from patients with blood group B. The predominant immunoglobulin isotypes of anti-A antibodies are IgG in blood group O and IgM in blood group B. 17
The results of our study are consistent with those of the study conducted by Gerard et al., who found that subjects with anti-A antibodies (blood groups O and B) were significantly underrepresented in COVID-19 compared with patients with blood groups A and AB (P < 0.001), A (P < 0.001), or AB (P = 0.032). They then examined whether there was a difference in anti-A antibodies between groups O and B. The prevalence of group O carriage was significantly lower among patients with COVID-19 (P < 0.001), whereas the prevalence of group B carriers was significantly higher (P < 0.001), indicating that anti-A antibody from blood group O carriers is more protective than anti-A antibody from blood group B carriers. 18
Another study in Iraq revealed that when compared with patients with other blood groups, patients with blood group A had the highest rate of COVID-19, whereas the COVID-19 rate was lowest among blood group O carriers. Meanwhile, Ad’hiah and colleagues reported that blood group A might be associated with an increased risk of COVID-19, particularly among men. 19
In addition, several studies found that people with blood group O have a lower risk of COVID-19, whereas people with non-O blood groups, particularly group A, have a higher risk. In a French study involving 998 samples collected from blood donors, the seroprevalence rate of SARS-CoV-2 neutralizing antibodies was lower among group O donors than among non-O donors. 20
The results of other studies as reviewed by Sapha et al. indicated that individuals with blood group A have higher risks of SARS-CoV-2 infection and severe outcomes, whereas people with blood group O are protected against the infection to some extent. One main hypothesis to explain these findings is that people in blood groups O and B have naturally occurring anti-A antibodies that might act as a partial defense against SARS-CoV-2 virions because of differences in the nature of these anti-A antibodies. 21 A useful application of this theory would be in convalescent plasma therapy, in which donors with higher titers of natural antibodies based on blood group could be selectively recruited to optimize treatment. 22
Although there were no significant variations in age or sex among the blood groups, the majority of patients with blood type A were older than 60 years. Consequently, the rates of comorbidities were higher among blood group A patients than among non-A patients. Diabetes mellitus and hypertension were the most frequent comorbidities among blood group A patients. Furthermore, patients with blood group A who tested positive for COVID-19 had higher risks of chronic renal disease and diabetes mellitus. Cough, shortness of breath, and headache were substantially more common among COVID-19–positive individuals with blood group A than in their counterparts with blood type B. Patients with blood groups A and O more frequently experienced body aches than those with other blood groups.
It should be noted that some prior studies contradicted our results. In a study by Zietz et al., non-O patients had a slightly higher prevalence of infection. When compared with group O, the risk of intubation was lower for group A and higher for groups AB and B, whereas the risk of death was higher for group AB and lower for groups A and B. 23 Meanwhile, some studies revealed no link between ABO blood groups and the susceptibility to SARS-CoV-2 infection.24–26
The disparity among studies could be attributed to differences in sample sizes, ABO heterogeneity among populations or geographical areas, differences in genetic backgrounds, and differences in viral strain. Variation in blood group phenotypes across countries, as well as genetic differences, might influence the heterogeneity of COVID-19 clinical phenotypes.
The findings of such studies could lead to individuals at a higher risk of severe infection being vaccinated earlier or being monitored and treated more closely. These findings suggest that blood groups can influence the susceptibility to SARS-CoV-2 infection and the clinical course of COVID-19.
The prevalence of blood group phenotypes in both the recovered and deceased patients is presented in Figure 4 and Table 2.
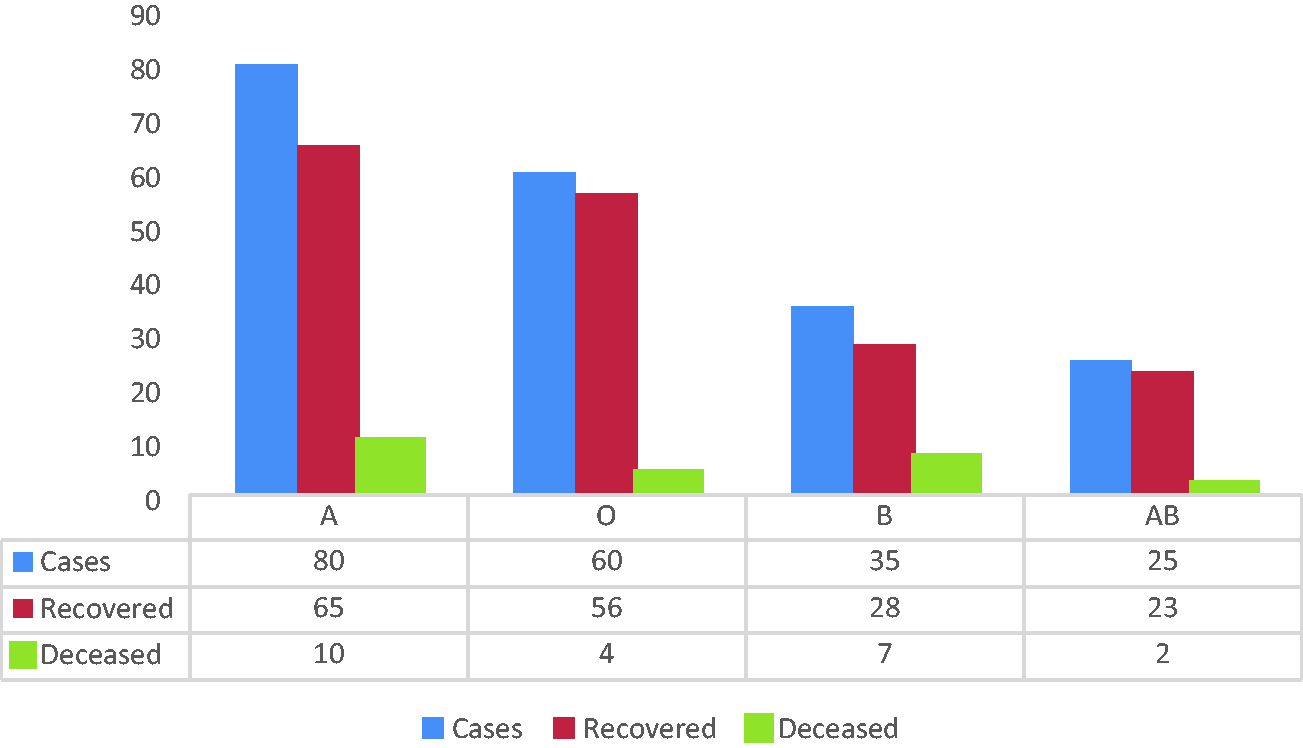
Blood group distribution among patients with COVID-19 according to the vaccination status.
Recovered and deceased patients categorized by sex, age, and blood group.

Associations of ABO blood groups with COVID-19 outcomes
The relationship among ABO blood groups and COVID-19 can be explained by a number of mechanisms. Anti-A antibodies, the generation of SARS-CoV-2 glycan antigens, the impact of genetics, coagulation system polymorphisms, and ABO gene mutations have all been hypothesized to influence the link between ABO blood groups and COVID-19 susceptibility. Glycosyltransferases A and B were demonstrated to affect glycosylation in a variety of respiratory epithelial cells. Anti-A antibodies, which are normally present in people with blood group O or B, might affect the interaction of the SARS-CoV-2 S protein with its membrane receptor angiotensin-converting enzyme 2 (ACE2) receptor. 27
The present study found that blood group O decreased the risk of critical and severe outcomes compared with blood group A. Anti-A antibodies found in group O people inhibit binding to antigens similar to those found on the SARS-CoV-2 envelope. Anti-A antibodies in group O people bind to the SARS-CoV-2 S protein, limiting the interaction of the SARS-CoV-2 S protein with the ACE2 receptor, potentially preventing viral entry into the lung epithelium (Figure 5). Any protection against infection or disease severity provided by the blood group status is only partial. Furthermore, the mechanism of these protective effects has not been fully clarified.

Interference with severe acute respiratory syndrome coronavirus 2 adhesion to host cells caused by blood groups.
Associations of blood group O with COVID-19 outcomes
In patients with COVID-19, blood group O is linked to a lower likelihood of severe outcomes. Blood group O individuals have higher von Willebrand and VIII factor levels, resulting in a lower risk of cardiovascular disease. 28 COVID-19 coagulopathy and vasculopathy traits have been revealed to play a significant role in the onset of acute respiratory distress syndrome. Consequently, it is believed that the lower risk of illness development in patients with blood group O was attributable to this occurrence. 29 Furthermore, blood group O carriers have reduced levels of ACE, which converts angiotensin I to angiotensin II. Given that angiotensin II can encourage inflammatory responses and increase blood pressure, the lower ACE levels in group O carriers could explain the lower risk of severe symptoms. 30
Associations of blood groups A and B with COVID-19 outcomes
Our data illustrated people with blood group A are most vulnerable to COVID-19. Blood group A was linked to higher rates of mechanical ventilation and death than the other blood groups.
By binding to A and/or B antigens expressed on the viral envelope, anti-A and/or anti-B antibodies operate as virus-neutralizing antibodies, preventing target cell contagion. Human anti-A antibody binds to the SARS-CoV-2 S protein, which can block the interaction of the virus with the ACE2 receptor, thereby blocking its access to the lung epithelium. The increase in ACE1 levels because of ABH gene polymorphisms found in people with non-O blood types increases the predisposition to cardiovascular problems, and such patients account for the majority of severe cases of COVID-19.31,32
The most common immunoglobulin isotype of anti-A antibodies in blood group O is IgG, whereas IgM, which is prevalent found in blood group B, plays an important role clinically because anti-A antibodies from individuals with blood groups O and B have different properties. A useful application of this approach might be applied to convalescent plasma therapy, in which donors with greater natural antibody titers based on the blood group might be preferentially selected to improve treatment outcomes. 33
Conclusion
According to the study results, the COVID-19 rate among patients in this study decreased in the order of A > O >B > AB. The study also found that patients with blood group A might be more susceptible to COVID-19. Conversely, the risk of COVID-19 was lower among patients with blood group O. However, mounting data suggest that ABO blood groups contribute to disease biology at the biochemical and physiological levels, and it has already been recognized to contribute to the severity of COVID-19. Furthermore, the association between vaccination reactogenicity and ABO blood groups was investigated in this study. This relationship remains uncertain, and more research is needed. Meanwhile, the proposed mechanisms are only hypotheses. The small sample size of this study represents a limitation, and further research with a large cohort is needed to validate the findings. The study found that the majority of patients who arrived at the hospital had already received the vaccine, and various age groups were represented. Our results indicated that vaccination resulted in a large reduction of COVID-19 risk across all age categories, but there has been an increase in the number of cases because of lower vaccine effectiveness in older patients and individuals with comorbidities. Conversely, immunization with 45% coverage reduced the peak of the outbreak and resulted in a daily incidence of less than 1% from the beginning of vaccination.