
Abstract
Objectives
The susceptibility to type 2 diabetes mellitus (T2DM) has been linked to blood type. We aimed to characterize the relationships of the ABO and Rhesus blood groups with T2DM.
Methods
Literature searches were performed using the Medline, PubMed, Scopus, Cochrane, EMBASE, and Google Scholar databases to identify studies published up to 31 March 2022. The PRISMA guidelines were used for reporting. Pooled odds ratios (ORs) with 95% confidence intervals (CIs) were obtained using fixed-effects models.
Results
Twenty-six studies of 6870 patients with T2DM and 11,879 controls were identified. Compared with the other ABO groups, people with blood type B were at higher risk of T2DM (OR: 1.30, 95% CI: 1.20–1.41), while group O was associated with a lower risk (OR: 0.92, 95% CI: 0.86–0.98). There were no significant associations of T2DM with blood types A or AB, or Rh factor.
Conclusion
Individuals with blood type B are at higher risk of developing T2DM. Therefore, they should be screened for T2DM on a frequent basis and be made aware of the importance of maintaining a balanced diet and regular exercise for the prevention of obesity and T2DM.
PROSPERO registration number
CRD42022353945.
Keywords
Introduction
Human ABO blood group antigens manifest as various transfusion phenotypes and are glycoconjugate structures that are located on the surface of red blood cells, where they play an important role in cellular physiology and pathology. 1 Although the physiological significance of ABO antigens and the corresponding natural anti-A and anti-B isoagglutinins remains poorly understood, they are known to be important during blood transfusion and cell, tissue, and organ transplantation. 2 The presence or absence of antigens corresponding to specific blood types leads to differences in the blood that have indirect effects on susceptibility to certain infectious3,4 and non-infectious diseases. 5 Previous studies have shown close associations between ABO blood groups and a variety of diseases, including cancer, cardiovascular disease, cognitive disorders, and metabolic disorders, such as hypertension, obesity, dyslipidemia, and diabetes mellitus.1,6
Diabetes mellitus is a metabolic disorder caused by defects in insulin production and/or action and is one of the most common diseases worldwide, being associated with high levels of morbidity and mortality. 7 ABO and Rh blood group phenotypes have been shown to be associated with various disorders, including type 2 diabetes mellitus (T2DM), 2 which may be underpinned by inherited differences in immunoglobulins. 8 A number of contributing factors, including genetic predisposition, and immunological and environmental factors, have significant effects on the pathogenesis and outcomes of T2DM. ABO and Rh blood groups are genetically predetermined; therefore, they may be genetically linked with other diseases with a substantial genetic components, such as DM. 9 T2DM susceptibility genes are located on the human 1q21-q23 chromosome region,10,11 whereas the ABO blood group genes are on chromosome region 9q34.2, which commonly shows variations. 12 Better knowledge of the links between T2DM and the ABO or Rh blood groups may assist with the prevention of T2DM by facilitating the avoidance of potential predisposing factors and help clinicians identify individuals who are susceptible to this disease.
Recent studies have shown that some ABO type antigens are risk factors for T2DM, whereas others have preventive effects. In addition, Rh blood group negativity and positivity have been shown to be protective or risk factors for T2DM in different studies.13–15 Therefore, we aimed to perform a meta-analysis of the results of previous studies to improve knowledge regarding the associations of ABO and Rh blood groups with T2DM.
Methods
Study design and reporting
We performed a systematic review and meta-analysis according to the Preferred Reporting Items for Systematic Review and Meta-Analysis protocol (PRISMA-P 2020 guidelines; Supplementary Table S1). 3 As such, there was no requirement for ethics approval or informed consent for the study. The study protocol for this systematic review and meta-analysis was registered in the International Prospective Register of Systematic Reviews (PROSPERO) with the registration number CRD42022353945.
Eligibility criteria
We included full-text articles that were published in peer-reviewed journals, and the participants in the studies described were of a range of ethnicities and socioeconomic levels. All comparative cross-sectional and case-control studies that contained clearly presented data regarding the ABO and Rh blood groups of patients with T2DM and controls that could be readily extracted. Letters to the editor, reviews, abstracts, simple cross-sectional studies, articles published in languages other than English, and those that did not report ABO and Rh blood type data for both cases and controls, or in which these data were difficult to extract, were excluded.
Information sources and search strategy
For the systematic review, relevant articles were identified by searching for publications regarding the associations of the ABO and Rh blood group antigens with T2DM in the Medline, PubMed, Science Direct, Cochrane, EMBASE, and Google Scholar databases. All the published articles regarding associations of the ABO and Rh blood types with T2DM that were published in English up to 31 March 2022 were included. The Medical Subject Heading and key words, combined using Boolean operators, were used to identify relevant studies. The search terms were “ABO blood group system/genetics” OR “ABO blood group” OR “ABO blood type” OR “Rhesus blood group” OR “Rh factor” AND “diabetes mellitus” OR “type 2 diabetes mellitus” (Supplementary Table S2). Additional studies were identified by screening the reference lists of the relevant articles and contacting appropriate authors and librarians.
Study selection and quality assessment
The retrieved articles were imported into EndNote X7 (Thomson Reuters, Toronto, Canada) to organize them and remove duplicate articles. Studies that conformed with the inclusion and exclusion criteria were selected independently by two reviewers (SG and BB), with disagreements resolved through discussion and with reference to a third reviewer (TA). The quality of reporting and the methodological quality of the included studies were assessed using the Newcastle Ottawa Scale (NOS), 17 a nine-point scale that includes points for the process of selection of the cases and controls (0–4 points), the comparability of the cases and controls (0–2 points), and the identification of the exposure and outcomes for the study participants (0–3 points). A study can be awarded maximums of 4 points for selection, 2 points for comparability, and 3 points for outcome. Quality assessment was independently performed by two authors (MA and YBW), and any disagreement was resolved by discussion. We classified studies as being of poor quality if they scored 0–3 points, fair quality if they scored 4–5 points, and good quality if they scored 6–9 points.
Outcomes of interest
The main outcomes of the study were the associations of ABO and Rh blood groups with T2DM.
Data extraction
Data were extracted by two authors after they reached a consensus regarding conformation with the criteria listed above. The following data were extracted from the included studies: first author name, publication year, study year, country where the participants lived, sample size, and the ABO and Rh blood group distributions among cases (with T2DM) and controls.
Statistical analysis
Statistical analysis of the included studies were performed using Stata 11.0 statistical software (StataCorp, College Station, TX, USA). Pooled odds ratios (ORs) and 95% confidence intervals (CIs) were calculated to quantify the associations of the ABO and Rh blood groups with T2DM. Heterogeneity analysis of the included studies was performed using Higgin’s I2 statistic, to determine whether fixed-effect or random-effect models should be used. A random-effects model would have been used when there was high heterogeneity (I2 ≥ 30% or P ≤ 0.05) and a fixed-effects model was used when there was lower heterogeneity (I2 < 30% or P > 0.05).18,19 Sub-group and sensitivity analyses were not performed because of the absence of significant heterogeneity. Egger’s regression test statistics and visual inspection of funnel plots for symmetry were used to evaluate publication bias.20,21 p < 0.05 was regarded as indicating statistical significance.
Results
Identified studies
A total of 2149 articles were retrieved from the electronic databases and through manual searches. Of these, 818 articles were subsequently removed because they were duplicates. We also excluded 1268 articles that were not relevant on the basis of screening their titles and abstracts. A further 37 articles were excluded because they were reviews, duplicates, letters to the editor, short communications, or studies that did not report the outcomes of interest. Thus, 26 articles were included in the qualitative and quantitative analyses performed in the present study (Figure 1).

Flow chart describing the selection process of the included studies.
Description of the included studies
Twenty-six relevant articles that met the inclusion criteria were included in the meta-analysis. All the selected articles described case–control or comparative cross-sectional studies. These studies included a total of 6870 patients with T2DM and 11,890 controls. Eight of the studies were conducted in India,7,12,13,22–26 three in Pakistan,27–29 three in Iraq,8,30,31 two in Ethiopia,14,32 and two in Malaysia;16,33 and the remaining eight were performed in Qatar, 34 Egypt, 35 Algeria, 36 Saudi Arabia, 37 Nigeria, 38 Turkey, 39 Iran, 40 or Morocco. 41 All of the studies included both male and female patients, except the one performed by Farshori et al., which only included male patients 37 (Table 1). Almost all of the included studies were awarded scores of 6–9 points on the NOS (Supplementary Table S3).
Description of the studies included in the meta-analysis of the relationships of the ABO and Rh blood groups with T2DM.

Abbreviations: NR: not reported; T2DM: type 2 diabetes mellitus; Rh, Rhesus factor.
Associations of the ABO and Rh blood groups with T2DM
The relationship between ABO blood group and T2DM was analyzed by calculating the odds of participants with T2DM having each blood group, compared with the controls, using a fixed-effect model. We found that people with blood type B were at a higher risk of T2DM than those with other types (OR: 1.30, 95% CI: 1.20–1.41) (Figure 2). The results of the heterogeneity testing for the blood group B and non-B groups were I2 = 13.6% and P = 0.266. In contrast, people with blood type O were at a lower risk of T2DM than those with other types (OR: 0.92, 95% CI: 0.86–0.98). There was no significant heterogeneity between the studies with respect to participants with blood group O and those with other groups (I2 = 0.0% and P = 0.520) (Figure 3).

Forest plot of the relationship between blood group B and type 2 diabetes mellitus.

Forest plot of the relationship between blood group O and type 2 diabetes mellitus.
The meta-analysis showed that people with blood group A were no more likely to have T2DM than those with other blood groups (OR = 1.04, 95% CI: 0.97–1.12). There was no significant level of heterogeneity between the studies of participants with blood group A and those with other groups (I2 = 0.0% and P = 0.997) (Figure 4). The results of the heterogeneity test for studies of participants with blood group AB and those with other groups were I2 = 0.0% and P = 0.999, and the meta-analysis showed that having blood group AB did not affect the risk of T2DM (OR = 1.03, 95% CI: 0.92–1.16) (Figure 5). Moreover, there was no significant association between Rh blood group and T2DM (OR = 0.91, 95% CI: 0.78–1.06). The level of heterogeneity among studies of participants who were Rh-positive or Rh-negative was not significant (I2 = 0.0 and P = 0.697) (Figure 6).
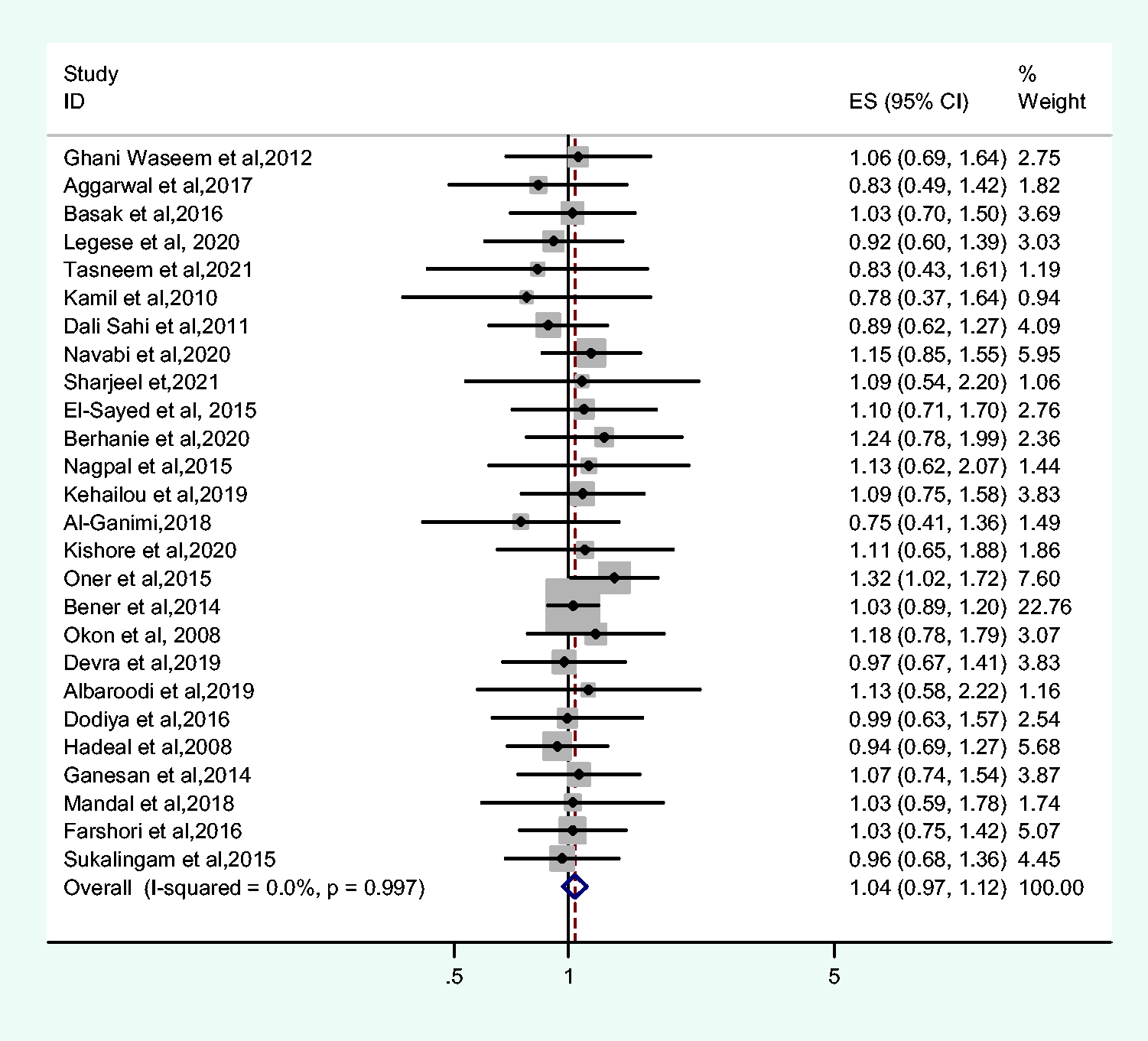
Forest plot of the relationship between blood group A and type 2 diabetes mellitus.

Forest plot of the relationship between blood group AB and type 2 diabetes mellitus.

Forest plot of the relationship between the Rh blood group and type 2 diabetes mellitus.
Publication bias
The included studies of the relationships of blood groups with T2DM were assessed for publication bias by the visual inspection of funnel plots for symmetry and Egger’s test statistic. No asymmetry in the funnel plots for the relationships of the various blood types with T2DM was identified, and Egger’s test showed no significant publication bias for individuals with blood group A versus other groups (P = 0.284), blood group AB versus other groups (P = 0.686), blood group O versus other groups (P = 0.818), and Rh-positive versus Rh-negative (P = 0.072). However, studies that included comparisons of participants with blood group B and other groups showed significant publication bias (P = 0.034) (Table 2 and Figure 7).
Results of Egger’s tests.

Rh, Rhesus factor.

Funnel plot of the included studies assessing the relationships of the ABO and Rh blood groups with type 2 diabetes mellitus.
Discussion
Antigens of the ABO blood group are found on a variety of human cells, including vascular endothelial cells and brain cells, in addition to red blood cells. 1 Links between blood group and a wide range of diseases, including obesity, 42 preeclampsia, 43 gestational diabetes, 44 gastric cancer, and cardiovascular disorders have been identified. 1 In addition, ABO blood group-related susceptibility to various viral infections, including with hepatitis B, influenza viruses, and severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), have been shown in several studies.45,46 However, only some of the previous studies have shown a link between T2DM and ABO blood group: some have shown no link,15,20,47,48 whereas others have shown a positive association.14,33 Therefore, in the present study, we explored the relationships of the ABO and Rh blood groups with T2DM by means of a systematic review and meta-analysis.
In the present study, we found that individuals with blood type B are at higher risk of developing T2DM than those with other blood types (OR: 1.30, 95%CI: 1.20–1.41). This finding is consistent with those of a previous single-center study performed by Legese et al. 14 and a review study performed by Meo et al. 49 Several studies have also shown that blood type B is associated with higher risks of a variety of disorders, including gestational diabetes, 50 gastric and pancreatic cancer 51 , and malarial infection. 52 In addition, people with blood type O were found to be at lower risk of T2DM than those with other blood types (OR: 0.92, 95% CI: 0.86–0.98). Overall, the present findings were consistent with those of some previous studies of the relationship between ABO blood group and T2DM.14,40,49,53 Several previous systematic reviews and meta-analyses have also shown that individuals with blood type O are at lower risk of infection, including with SARS-CoV-2,45,54 and preeclampsia. 43 In contrast, other studies have shown that individuals with blood type O are more likely to develop T2DM 22 and gestational diabetes, 44 Plasmodium falciparum infection, 55 and tuberculosis infection.56,57
The mechanisms underlying the observed associations have been suggested to involve endothelial and pro-inflammatory molecules, and the factor VIII–von Willebrand factor complex, plasma soluble intercellular adhesion molecule 1 (ICAM-1), and tumor necrosis factor receptor 2 (TNF-R2) concentrations are higher in individuals with blood groups other than O.58,59 Insulin resistance is associated with systemic inflammation, and both contribute to the development of T2DM. 60 In addition, the ABO blood group is a genetically determined host factor that influences the composition of the gut microbiota, which has also been shown to affect glucose metabolism, energy balance, and the level of inflammation present. 61
No associations were found of the blood groups A and AB with T2DM (OR = 1.04, 95% CI: 0.97–1.12 and OR = 1.03, 95% CI: 0.92–1.16, respectively) in the present study, consistent with the findings of previous studies performed in western Algeria, 36 India, 62 and Bangladesh, 15 which also showed no associations between the ABO blood groups and T2DM. In contrast, previous studies have shown that individuals with blood group A are more likely to develop T2DM38,40 and to have higher insulin and random blood glucose concentrations. 35 In addition, a study by Salem et al. performed in Egypt showed that blood type A is more common in patients with rheumatic disease. 4
We also found no significant association between Rh blood group and T2DM (OR = 0.91, 95% CI: 0.78–1.06), as previously shown in studies conducted in India, 22 Algeria, 36 and Ethiopia. 14 However, a study by Stern et al. showed a statistically significant association between T2DM and Rh blood type. 63 Similarly, a study performed in Iran 31 showed that Rh-positivity is positively associated with T2DM. In addition, the study by Salem et al. showed that Rh-positivity is more common in patients with rheumatic disease. 4 In contrast, a study conducted in Pakistan 27 showed that Rh-negativity is significantly associated with T2DM. A possible explanation for this is that the Rh blood system may be linked to glucose metabolism, and thereby affect the clinical manifestation of diabetes. Further research is necessary to better understand how specific genes contribute to the regulation of blood glucose concentration and affect susceptibility to T2DM.
The clinical implications of the present findings are that individuals with blood group B are at higher risk of developing T2DM, while those with blood group O are at lower risk. This suggests that individuals with blood group B might be predisposed toward obesity and diabetes mellitus. 16 Thus, numerous factors, including genetic, environmental, and dietary factors, obesity, and a lack of exercise are associated with the development of diabetes mellitus. 37
The present study has both strengths and limitations. The strengths of the study include the identification of relevant articles through a comprehensive data search that permitted the analysis of the relationships between blood groups and T2DM. In addition, the level of heterogeneity of the included studies was low, which implies that the present findings should be accurate. However, the inclusion of articles published only in English may have affected the outcomes. In addition, the use of the ABO blood group to predict the development of T2DM is clearly inadequate on its own, but other relevant risk factors were not considered in the present study. Furthermore, the effect of differences in the distributions of the ABO phenotypes between countries was not considered in the analysis. Finally, the biological mechanism through which the ABO blood group system may influence the prevalence of T2DM has not been elucidated.
Conclusion
The findings of the present study imply that there is a link between T2DM and the ABO blood group system. We have shown that blood type B is linked to a higher risk of T2DM, whereas blood type O is associated with a significantly lower risk. However, we found no connection between the Rh blood group and T2DM. Therefore, individuals with a high risk profile should be screened for T2DM on a frequent basis and should be aware of the importance of a well-balanced diet and regular exercise for the prevention of obesity and T2DM.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221129547 - Supplemental material for Relationships of ABO and Rhesus blood groups with type 2 diabetes mellitus: a systematic review and meta-analysis
Supplemental material, sj-pdf-1-imr-10.1177_03000605221129547 for Relationships of ABO and Rhesus blood groups with type 2 diabetes mellitus: a systematic review and meta-analysis by Solomon Getawa, Biruk Bayleyegn, Melak Aynalem, Yilkal Belete Worku, Tiruneh Adane in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605221129547 - Supplemental material for Relationships of ABO and Rhesus blood groups with type 2 diabetes mellitus: a systematic review and meta-analysis
Supplemental material, sj-pdf-2-imr-10.1177_03000605221129547 for Relationships of ABO and Rhesus blood groups with type 2 diabetes mellitus: a systematic review and meta-analysis by Solomon Getawa, Biruk Bayleyegn, Melak Aynalem, Yilkal Belete Worku, Tiruneh Adane in Journal of International Medical Research
Supplemental Material
sj-pdf-3-imr-10.1177_03000605221129547 - Supplemental material for Relationships of ABO and Rhesus blood groups with type 2 diabetes mellitus: a systematic review and meta-analysis
Supplemental material, sj-pdf-3-imr-10.1177_03000605221129547 for Relationships of ABO and Rhesus blood groups with type 2 diabetes mellitus: a systematic review and meta-analysis by Solomon Getawa, Biruk Bayleyegn, Melak Aynalem, Yilkal Belete Worku, Tiruneh Adane in Journal of International Medical Research
Footnotes
Acknowledgements
We would like to acknowledge the contributions of all the authors of the included studies.
Author contributions
All the authors contributed to the literature search, manuscript drafting, statistical analysis, and quality assessment. The authors all participated in the revision of the paper, gave their approval for its submission, and agree to be accountable for all aspects of the work.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.