
Abstract
Eosinophilic angiocentric fibrosis (EAF) is a rare chronic benign disorder of unknown etiology and is characterized by submucosal thickening and fibrosis in the upper respiratory tract. In this report, we describe a case of EAF in the nasal cavity of a woman who underwent elective surgery for division of adhesions and has had no recurrence during 2 years of postoperative follow-up. A review of the literature on the clinical manifestations of EAF, sites of lesions, management, and outcomes identified 48 articles that included 72 cases. A summary of these reports is presented, including our present case. The most common anatomic site involved was the nose (77.8%), the most common manifestation was nasal obstruction (66.7%), and the most common treatment modality was surgical resection (83.3%). After surgery, 36% of patients remained free of EAF. The most common pharmacologic agent used was a corticosteroid (38.9%).
Keywords
Introduction
Eosinophilic angiocentric fibrosis (EAF) is a non-malignant inflammatory disease that reportedly can affect almost any area of the face, including the nose, 1 orbits, eyelids, 2 larynx, 3 and subglottis. 4 There have also been occasional reports of lower respiratory tract involvement with airway narrowing.5,6 In 2011, Deshpande et al classified EAF as part of the spectrum of immunoglobulin (Ig)G4-related systemic diseases and observed that it was characterized by a tendency to form tumefactive lesions in the affected organ. 5
The term “eosinophilic angiocentric fibrosis” was coined in 1985 when Roberts and McCann published their initial description of three cases. 7 They described EAF as a mucosal lesion that is accompanied by thickening of the submucosal connective tissues. The disease starts as a focal perivascular subepithelial exudate of eosinophils with a collection of plasma cells and lymphocytes without fibrinoid necrosis. These foci form widespread areas of perivascular fibrosis with marked angiocentric rotation. This process leads to thickening and turbidity of the mucosa, which becomes adherent to the underlying structures. As the fibrosis progresses, the lymphoblastic component recedes but the eosinophils remain. The fibrosis does not resolve, and the resulting stenosis requires surgical resection. Noting that these lesions occurred in the upper respiratory tract, Roberts and McCann described this disorder as “upper respiratory eosinophilic angiocentric fibrosis” to cover its main features.
The histopathologic characteristics of EAF include a dense fibrotic stroma with a perivascular “onion skin-like” whorling pattern and a dense inflammatory infiltrate consisting of lymphocytes, plasma cells, eosinophils, and some neutrophils. Modest acute neutrophilic inflammation with focal endothelial proliferation, 1 a collagen bundle winding around the vessels in an onion-skin pattern, and eosinophils, lymphocytes, and plasma cells 2 may be present.
This report describes a case of EAF in the nasal cavity in a woman who underwent elective surgery for division of adhesions and has had no recurrence during 2 years of postoperative follow-up. a review of the literature on the clinical manifestations of EAF, sites of lesions, management, and outcomes is presented. This report provides an opportunity to discuss clinically relevant issues and raise awareness of EAF as a disease entity.
Case report
A woman in her early 60 s was referred to our center with a complaint of nasal obstruction and postnasal drip. She had a history of hypertension, for which she was on treatment. Four years earlier, she had undergone antrostomy for nasal obstruction. At that time, the histopathologic diagnosis was mild mucositis, and she made a symptomatic recovery. A recent clinical examination had revealed obstruction of the right nares and deviation of the nasal septum to the right. Further clinical examinations, including a complete blood count, C-reactive protein, antinuclear autoantibodies, antineutrophil cytoplasmic antibodies (ANCA), and peripheral antineutrophil cytoplasmic antibodies (p-ANCA), were in the normal range (Table 1). A chest radiograph was normal. Magnetic resonance imaging (MRI) of the paranasal sinuses revealed relative thickening of the anterior portion of the nasal septum extending anterolaterally and involvement of the nasal cartilages with extension up to the subcutaneous tissue (measuring approximately 2.6 × 1.8 cm) (Figure 1). Fungal granuloma was suggested as a differential diagnosis on MRI. She underwent elective surgery for division of adhesions.
Results of blood and tissue examinations in a patient with eosinophilic angiocentric fibrosis.

*Some values and normal ranges shown in the table are expressed in the conventional units measured by the devices and laboratory kits used at our institution.
ACE, angiotensin-converting enzyme; ANA, anti-nuclear antibodies; C-ANCA, anti-PR3 antibody; ESR, erythrocyte sedimentation rate; IHC, immunohistochemistry; LDH, lactate dehydrogenase; P-ANCA, anti-myeloperoxidase antibody; PT, prothrombin time; PTT, partial thromboplastin time; RBC, red blood cells; TSH, thyroid-stimulating hormone; WBC, white blood cells.
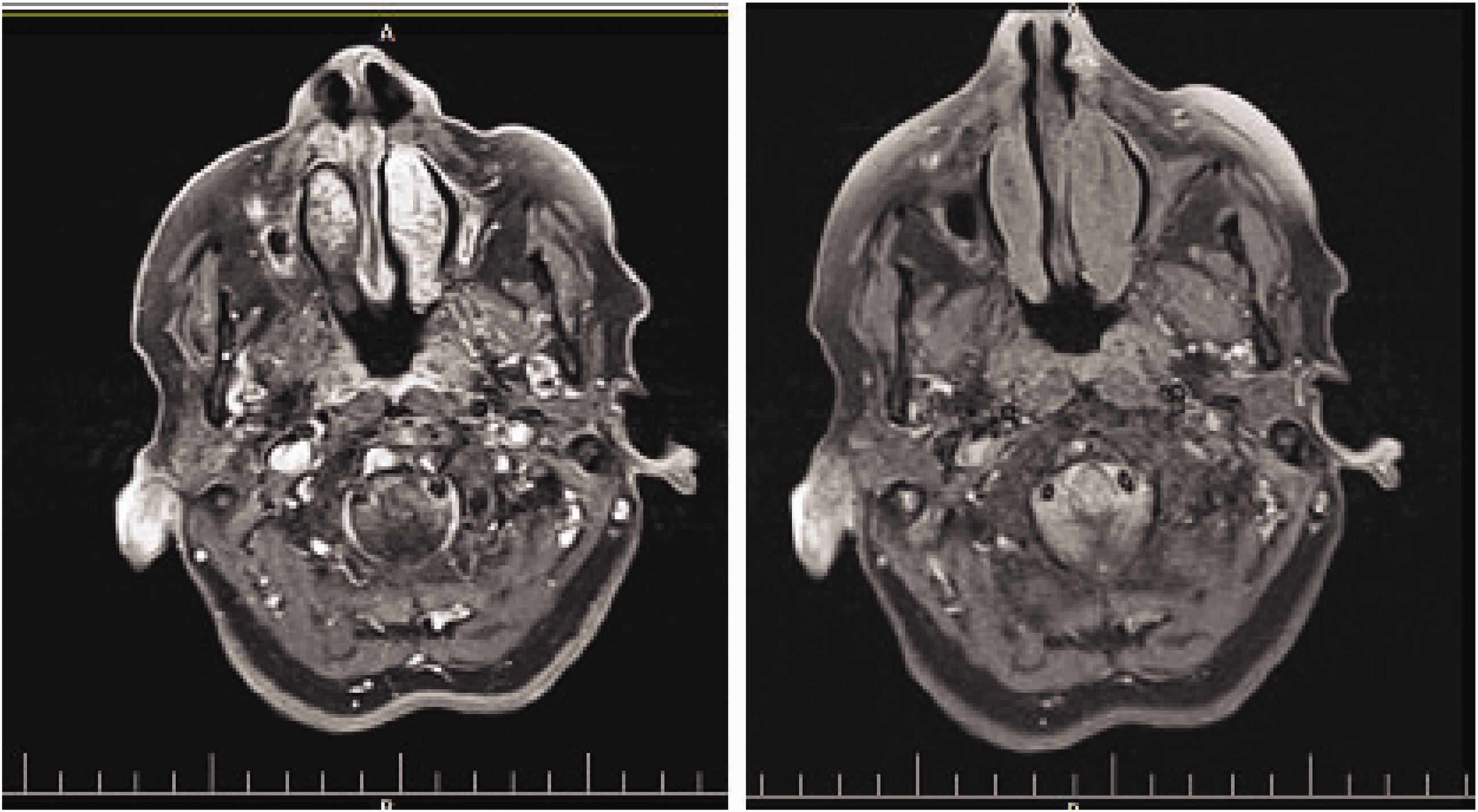
Axial T1-weighted images of the nasal cavity with and without contrast.
Histologic examination of resected small tissue fragments revealed perivascular whorling of bland collagen fibers (onion skin-like appearance) with resulting obliteration of the vessel lumens (characteristic of the fibrotic stage of EAF) (Figure 2a). Some eosinophils were noted within the fibrosis. There were fragments of normal mucosa, overlain by respiratory-type epithelium, which included a moderate chronic inflammatory cell infiltrate. Although a small number of eosinophils and neutrophils traversed the vessel walls, there was no evidence of fibrinoid necrosis or vasculitis. No giant cells, necrosis, or granuloma formation were present. Trichrome staining highlighted collagen whorls around vessels (Figure 2c). Specific stains for fungi, bacteria, and acid-fast bacilli were negative. In an immunohistochemical study, vimentin was strongly and diffusely positive in fibrotic areas of spindle cells and collagen bundles. These perivascular fibrotic areas were nonreactive with smooth muscle actin (Figure 2d) and CD34.

Histopathologic photomicrograph showing (a) fibrocollagenous tissue with perivascular infiltration of eosinophils accompanied by extensive areas of perivascular fibrosis (arrow) showing a characteristic angiocentric whorling with an onion skin-like pattern (hematoxylin and eosin staining, ×40 objective). (b) Masson trichrome staining shows perivascular fibrosis in the typical concentric pattern (×40 objective). (c) Diffuse positive staining for vimentin on immunohistochemistry (×40 objective) and (d) Negative staining for smooth muscle actin on immunohistochemistry (×40 objective).
Discussion
The PubMed database was searched for all case reports on EAF published from inception in 1983 to 1 August 2022. All reports published in English that included the keywords “eosinophilic angiocentric fibrosis” OR “EAF” were extracted. The search yielded 47 eligible reports that included 71 cases of EAF.
The most commonly involved site was the nose (77.8%), the most common clinical manifestation was nasal obstruction (66.7%), and the most common management modality was surgical resection (83.3%). After surgery, 36% of patients were free of EAF without recurrence. The most common pharmacologic agent used was a corticosteroid (38.9%). The clinical manifestations, sites of lesions, management, and outcomes are summarized in Table 2.
Summary of cases of eosinophilic angiocentric fibrosis reported to date in the literature.

F, female; FD, free of disease; M, male; PD, persistent disease; NA, not available.
EAF is a rare lesion of the sinonasal or upper respiratory tract, most commonly presenting with prolonged obstructive symptoms, a recurrent sinus mass, thickening of the mucosa, and deformity of the nose because of destruction of cartilage. A definitive diagnosis of EAF relies on histopathologic findings that include inflammation, infiltration of eosinophils, fibrotic bundles around the arteries, and an onion skin-like pattern with fibrotic stroma, usually without any signs of malignancy.5,9–12
Our case was a woman in her early 60 s who had a 7-year history of a progressive nasal sinus mass. During this time, the mass had progressed to the frontal lobe and affected her vision. Furthermore, there was destruction of the nasal septum and appearance of the saddle nose deformity. EAF was diagnosed based on histopathologic, immunologic, and MRI findings
The symptoms of EAF are very vague in the early stages, the most common being nasal obstruction, epistaxis, respiratory problems, epiphora, proptosis, decreased sense of smell, and allergies to substances such as wool, plants, and carpet fluff. The disease is diagnosed radiologically by computed tomography or MRI. Soft tissue swelling, sinus opacification, thinning of the surrounding bone, turbidity of the nasal cavity and sinuses with or without bone erosion, sclerosis, and focal bone destruction are noted in radiographic reports. 10
Histopathologic findings depend on the stage of the disease. Although there is no clear boundary between early and late lesions, the early stage is characterized by inflammatory eosinophil-rich vascular fibrotic lesions, and the late stage by dense perivascular (onion skin-like) fibrosis with fewer inflammatory cells. The biopsy can distinguish between the early and later stages of the disease. 9
The differential diagnosis of EAF includes neoplasms and non-infectious granulomatous diseases, such as Wegener's granulomatosis, eosinophilic granulomatosis with polyangiitis (Churg–Strauss syndrome or allergic granulomatosis), granuloma faciale (GF), and Kimura disease. 13
The histopathologic findings of Wegener’s granulomatosis include granulomatous vasculitis, geographic necrosis, and a positive C-ANCA test. 14 Churg–Strauss syndrome is characterized by eosinophilic vasculitis, fibrinoid necrosis with granuloma, and a positive P-ANCA test. 15 In Kimura disease, dense lymph masses with prominent germinal centers are dominant, and although fibrosis is present, it lacks the typical angiocentric rotation pattern characteristic of EAF. 16 GF is a benign skin disease of unknown cause that is severely limited by plaques and skin nodules tending to the facial area but mucosal involvement is also possible. 17 EAF is also referred to as an extracutaneous GF lesion. 18 Histopathologic examination of GF shows diffuse infiltration of eosinophils, neutrophils, and lymphoid cells at the surface. The primary lesion shows vasculitis, and although fibrosis exists, it is neither prominent nor concentrated in layers. 17
Immunoglobulin (Ig)G4-related diseases, like EAF, are a complex of inflammatory diseases that affect various organs, including the pancreas, lungs, kidneys, and salivary glands. 19 IgG4 increases in only 50% of patients. Elevated plasma cell concentrations associated with IgG4 and an IgG4 to IgG ratio of >0.4 support a diagnosis of EAF. 5
Immunohistochemistry and flow cytometry examinations can aid in the clarity of lesion components, although most are not necessary for EAF. Flow cytometry usually shows no unusual T-cell populations, plasma cells are polyclonal, and infiltrating cells are a combination of neutrophils, histiocytes, and eosinophils. On immunohistochemistry, vimentin is positive, smooth muscle actin is negative or may be positive in a small number of cells, S100 is negative, and diagnostic bacterial, acid-fast, and fungal staining tests are all negative. 9
The treatments used for EAF to date include surgery (endoscopic sinus surgery, lateral rhinotomy, open rhinoplasty, septoplasty, curettage, and lesion excision), corticosteroids (systemic and/or intralesional), and immunosuppressive agents (azathioprine, dapsone, clofazimine, tacrolimus, hydroxychloroquine) either alone or in combination. However, in some cases, the disease has not been completely cured and has relapsed. 20
EAF of the sinonasal tract is a benign but progressive disease. Surgery is helpful in patients with obstructive symptoms. Recurrence is rare but typically occurs at the site of the primary lesion. Therefore, EAF is considered to be a progressive disease. The disease may progress in some patients, even with corticosteroid therapy. Therefore, close follow up is essential.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
The research protocol obtained ethical approval from and was performed under the supervision of the review board of Kermanshah University of Medical Sciences. This report is presented in accordance with the CARE guidelines. 8 Written and verbal informed consent was obtained from the patient. The ethical standards relevant to patient confidentiality were observed at all times.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.