
Abstract
Superior mesenteric artery syndrome is a rare manifestation of small bowel obstruction caused by the compressed third part of the duodenum between the superior mesenteric artery and the abdominal aorta. We present the case of an 18-year-old female and presented with symptoms of duodenal outflow obstruction. Upon investigation, her cross-sectional imaging revealed partial obstruction of the distal duodenum at the crossing of superior mesenteric artery forming an acute angle between the superior mesenteric artery and aorta. Failing initial attempts at conservative management, the patient underwent laparotomy and duodenojejunostomy with complete relief of symptoms. Superior mesenteric artery syndrome is a rare but a sinister diagnosis in patients presenting with features of duodenal outflow obstruction. Cross-sectional imaging plays an important role in diagnosis.
Introduction
Superior mesenteric artery (SMA) syndrome is a rare condition that causes compression of the third part of the duodenum in between the SMA and abdominal aorta. It is a rare manifestation with an incidence of around 0.1–0.3%. 1 This condition is mainly seen among young females, especially associated with recent weight loss. Once the conservative management with nutritional optimization fails, surgical intervention such as duodenojejunostomy is the gold standard in management. However, there are other less effective approaches such as the lysis of the ligament of Treitz or jejunostomy. 2 Recent advancements in minimal invasive procedures enable surgeons to perform complex procedures without the necessity to perform a laparotomy. Thus, the current choice of management is laparoscopic duodenojejunostomy. Though it is rare, the mortality rate can still be as high as 33%. 3 The present case highlights the diagnostic challenges and emphasizes the importance of increased awareness of the entity as an atypical cause of proximal intestinal obstruction.
Case presentation
We present a case of an 18-year-old female who was apparently well who presented with multiple episodes of vomiting, upper abdominal pain and constipation 1 year back which was managed conservatively as subacute intestinal obstruction at the local hospital from which she made a full recovery. However, she kept developing three similar episodes over the rest of the year. In-between these episodes, she was completely asymptomatic and did not show symptoms of any food intolerance. In the process of evaluating her symptoms, she was managed at a nutrition clinic and a conservative approach was tried. A psychiatric evaluation was also performed to rule out any psychogenic vomiting. Thus, the cause was isolated to be entirely of organic pathology.
She presented to the surgical clinic with the above history, however, she was asymptomatic at that time. She was thinly built with a body mass index (BMI) of 18.4 kg/m2 on presentation. The remaining examination was unrevealing. Her basic biochemical investigations were normal, and initial imaging from ultrasound did not show any abnormalities.
Further imaging with a contrast enhanced computed tomography (CECT) showed partial obstruction of distal duodenum at the crossing of SMA due to reduced angulation between SMA and aorta. There is also acute angle in the narrowed point of duodenum at the level of SMA due to duodenal and Jejunal redundancy. There was no associated gut malrotation or any masses or filling defects in stomach or duodenum (Figures 1–3).

Axial view of superior mesenteric artery compressing the duodenum (circled).
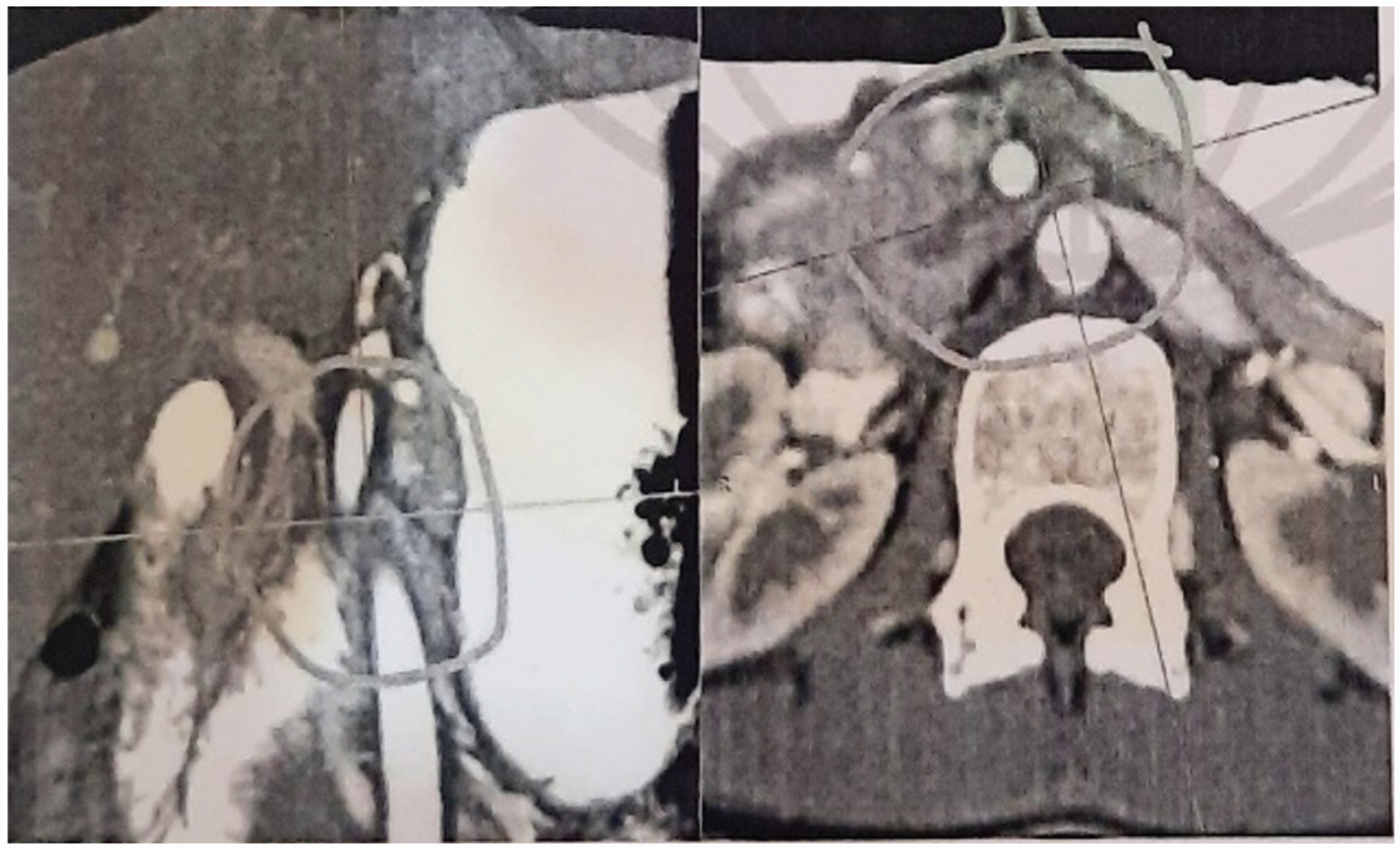
Sagittal and axial views of SMA (circled).

Sagittal view of SMA (origin circled).
Patient underwent an elective laparotomy with upper midline incision and duodenojejunostomy was performed as there were no facilities available for a laparoscopic approach. She had an uneventful recovery with good tolerance of oral intake and was discharged on post-operative day 3. Patient was reviewed in the post-operative clinic in 4 weeks and 6 months’ time, her symptoms had resolved with a significant rise in BMI to 22.3 kg/m2.
Discussion
Carl Freiherr Von Rokitansky, an Australian professor in 1861 described the SMA syndrome anatomically as an autopsy finding. 4 Later in 1927, the exact pathophysiology and management were explained by Willkie. 5 Hence, the SMA syndrome is also known as Wilkie’s syndrome. The normal aortomesenteric angle (AMA) between the SMA and the abdominal aorta is 25–60° at an aortomesenteric distance of about 10–28 mm. 6 Narrowing of this angle to < 25°, and the reduction in the distance < 10 mm would cause compression of the third part of the duodenum. A common cause for SMA syndrome is loss of the mesenteric fat pad or retroperitoneal fat following weight loss. Other congenital causes can be high insertion of ligament of Treitz dislocating the duodenum superiorly or low insertion of SMA. Iatrogenic causes of SMA syndrome are following scoliosis correction surgery due to the correction in height, 7 and total proctocolectomy and ileal J pouch anal anastomosis due to the resulting tension of the mesentery. 8
However, the clinical features manifest when the AMA angle drops below 20°. 5 In the present case, the AMA was 7°, and the aortomesenteric distance was 8 mm (Figure 3), resulting in the symptomatic presentation. SMA syndrome presents as a diagnostic dilemma due to its insidious presentation with non-specific findings and potentially normal basic evaluation. Although rare, it is important to keep an open mind on the possibility of its occurrence specially when associated with recent weight loss. A missed diagnosis can lead to morbidity due to electrolyte imbalance, nutrition deficiency and catabolism, gastric perforation, and peritonitis. 9
The clinical features can be acute or acute on chronic depending on the disease severity. In acute presentation, patient presents with features suggestive of duodenal obstruction similar to the present case. In chronic cases, patients have long-standing vague abdominal pain or recurrent abdominal pain with vomiting. Less number of patients experience gastro-esophageal reflux, abdominal fullness with early satiety.7,10–13 High clinical suspicion would aid the diagnosis along with supportive imaging. Barium studies can be used to demonstrate a proximal obstruction with or without gastric dilation and a delay in transit time with a relief of obstruction in prone, knee-chest or left lateral positioning. 10 However, cross-sectional imaging such a CECT or magnetic resonance angiography is the gold standard in visualizing the extrinsic compression of the duodenum and measurement of the aortomesenteric angle and the distance. In the present case, CECT imaging helped reach the diagnosis. Endoscopic examination can also be performed, which will show a pulsatile extrinsic compression of the duodenum. 9
Management comprises of initial conservative measures such as parenteral nutrition, motility agents, and gastric decompression. Failing conservative management surgery is considered. Duodenojejunostomy is the procedure of choice with a high success rate of around 90%, which was practiced in the present case. 10 The current trend is to resort to laparoscopic duodenojejunostomy, however, due to resource constraints, we could only perform the procedure as a laparotomy.
SMA syndrome is a rare but a potentially life-threatening presentation of proximal bowel obstruction. Although rare, a high index of suspicion should be in mind when patients present with significant weight loss. Cross-sectional imaging such as CECT is of high diagnostic value in these patients. The treatment of choice is duodenojejunostomy, which can achieve a high success rate with symptom relief.
Footnotes
Acknowledgements
None.
Author contributions
PGND and RJ contributed to concept and design of study, acquisition of data, analysis, interpretation of data, drafting the article, and final approval of the version to be published. PGND, RJ, and AW contributed to concept and design of study, revising it critically for important intellectual content, and providing final approval of the version to be published.
Data availability
Upon reasonable request from the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article. Informed written consent was obtained from the patient for publication of the case and related images.