
Abstract
Adenofibroma is an extremely rare benign biphasic tumour composed of glandular and fibrous tissues. It occurs more often in the endometrium but it can also occur in the cervix and extrauterine sites. This case report describes a 39-year-old asymptomatic woman with cervical adenofibroma. The patient was treated successfully with surgical removal of the tumour. As adenofibromas are very rare, the report is presented with a brief review of the literature.
Introduction
Cervical adenofibroma was first described by Abell in 1971 as a form of mixed mesodermal tumour. 1 It is a rare tumour that accounts for only 10% of uterine adenofibromas, 2 with most neoplasms arising in the endometrium. 3 When this tumour occurs in the cervix, it usually presents first with abnormal vaginal bleeding. 3 It can occur at any age, but it is most commonly found in perimenopausal or menopausal women. 3 There are no typical preoperative clinical or sonographic characteristics that strongly suggest this diagnosis. 4 Therefore, it is mainly diagnosed by pathological examination of a biopsy sample. Cervical adenofibroma needs a differential diagnosis with adenosarcoma, adenomyoma and carcinosarcoma. 5 This case report describes an asymptomatic patient with cervical adenofibroma.
Case report
In July 2021, a 39-year-old married woman was undergoing a routine physical examination at a local hospital when they observed myoma-like tissue in the cervical orifice that was protruding outward. The local hospital suggested a diagnosis of ‘submucosal myoma of uterus’ and referred the patient to the Guangdong Provincial People' s Hospital Ganzhou Hospital (Ganzhou Municipal Hospital), Ganzhou, Jiangxi Province, China for further diagnosis and treatment. Endovaginal ultrasound revealed a hypoechoic area on the left anterior wall of the uterus that was 43 mm at its maximum diameter. There are two hypoechoic areas in the posterior wall of the uterus, which had maximum diameters of approximately 29 mm and 13 mm. Hysteroscopy observed myoma-like tissue from the outer mouth of the cervix to the cervical tube, with a size of approximately 3.0 × 3.5 cm. The pedicle was located near the inner mouth of the right anterior wall of the cervical tube. The pedicle was wide, the anterior wall of the uterine cavity protruded slightly inward, the openings of both fallopian tubes were visible and the endometrium was thin. Based on the above examination, it is preliminarily considered to be a hysteromyoma and cervical submucosal myoma, so hysteroscopic cervical submucosal myoma resection plus laparoscopic hysteromyoma removal was planned. After hysteroscopic treatment, the cervical tumour was removed. The tumour was located at the cervical orifice and the pedicle was located at the right anterior wall of the cervix, so the pedicle was twisted to break it. During hysteromyoma removal under laparoscopy, a myoma-like nodule protrusion with a size of approximately 4.0 × 5.0 cm was observed on the left side of the lower section of the anterior wall of the uterine fundus and a myoma-like nodule protrusion with a size of approximately 3.0 × 4.0 cm was observed near the uterus on the posterior wall of the uterus. These two myoma-like protrusions were completely removed. Surgical specimens were sent for pathological examination.
Histopathological examination of the cervical mass showed lobulated or papillary growth. It was mainly composed of endometrioid glands or cervical mucinous glands and fibrous stroma. The gland was similar to proliferative endometrium, the gland tube was small, the cells are arranged in monolayers and pseudostratified, and the cells had no obvious abnormity. The surrounding stroma was rich and evenly distributed. The cells were round, oval or spindle shaped; and no atypia or mitosis was observed (Figure 1). The final pathological diagnosis was cervical adenofibroma. This case has been reported according to the CARE guidelines. 6 Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
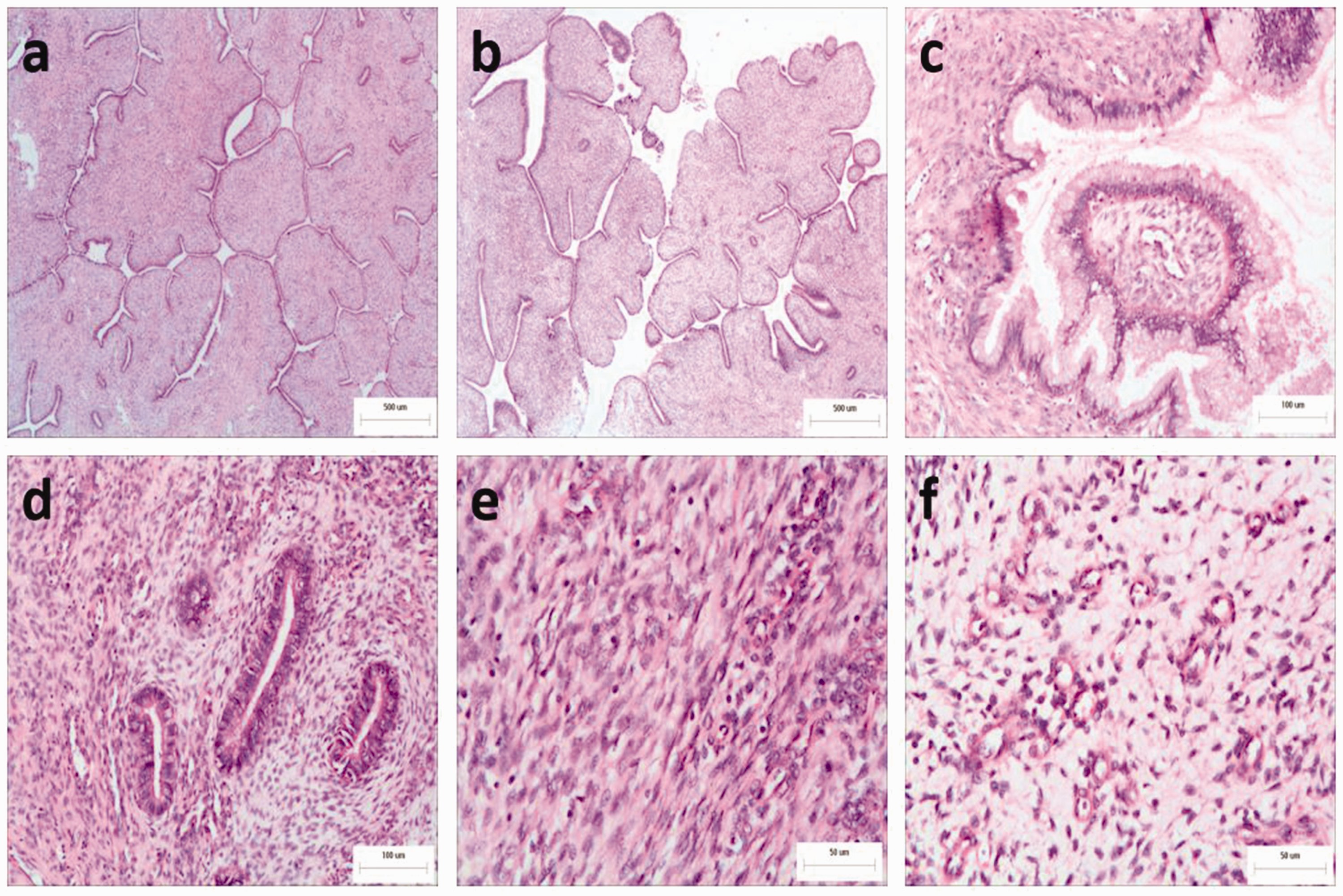
Representative photomicrographs of sections from a cervical mass removed from a 39-year-old woman in whom a routine physical examination observed myoma-like tissue in the cervical orifice: (a) lobulated structure (haematoxylin & eosin [H&E], scale bar 500 µm); (b) papillary structure (H&E, scale bar 500 µm); (c) cervical mucinous glands (H&E, scale bar 100 µm); (d) endometrioid glands (H&E, scale bar 100 µm); (e) the surrounding stroma was rich and evenly distributed. The cells were round, oval or spindle shaped. There was no atypia or mitosis observed (H&E, scale bar 50 µm); (f) some tumours area had loose stroma, mucus degeneration and abundant blood vessels (H&E, scale bar 50 µm). The colour version of this figure is available at: http://imr.sagepub.com.
Discussion
Adenofibroma of the cervix is a rare benign mullerian mixed tumour, which contains both benign epithelium and benign mesenchymal tissue. Patients with cervical adenofibroma are often elderly women in whom the disease mainly manifests as abnormal uterine bleeding or postmenopausal bleeding. 7 This current case report describes a 39-year-old woman without any clinical symptoms. As it is difficult to identify this disease based on clinical manifestations, a pathological examination is essential to make a clear diagnosis.
The incidence rate of cervical adenofibroma is very low and the origin of this tumour remains controversial. At present, some researchers believe that it represents an endometriosis with extreme smooth muscle metaplasia. 7 Others believe that it originates from the Müllerian duct. 5 A previous report described a case of cervical adenofibroma with endometriosis. 8
Physical examination can be normal in patients, such as that described herein for the current case, with patients only showing cervical polypoid tumours. In terms of the pathology of the adenofibroma tumour, it must be differentiated from cervical polyps, adenomyomas, adenosarcomas and carcinosarcomas. The histopathological morphology of cervical polyps is characterized by glands that have mucinous columnar epithelium with loose and oedematous stroma. 9 The pathological morphology of adenomyoma is characterized by the tumour stroma being smooth muscle. 10 The pathological features of carcinosarcoma are malignant epithelium and malignant mesenchymal tissue. 11 Cervical adenosarcoma and adenofibroma share very similar histomorphology and the two differ mainly in the stroma. 12 Adenosarcoma is diagnosed if the stroma shows atypia, increased periglandular stromal cells, invasiveness and mitotic figures ≥4/10 high-power fields. 13 Therefore, it is particularly important to distinguish between cervical adenofibroma and adenosarcoma.
Although adenofibroma is a benign tumour, it has been shown to invade the myometrium and pelvic veins, relapse and even metastasize.5,7 Therefore, hysterectomy is the first choice for the treatment of adenofibroma. In addition, because adenofibroma mainly occurs in the perimenopausal or postmenopausal periods, total hysterectomy is feasible and it can ensure complete resection of the tumour. However, for young women that want to reproduce, extensive local hysterectomy through surgical hysteroscopy can be an alternative to hysterectomy, provided that the integrity of the resection is verified and long-term follow-up can be carried out.
In conclusion, although cervical adenofibroma is very rare, if a cervical tumour is found, it should be differentiated from cervical adenofibroma regardless of the clinical symptoms. In addition, more detailed histopathological studies are needed to distinguish between cervical adenofibroma and adenosarcoma.