
Abstract
Herpes zoster is not common in multiple myeloma (MM) patients treated with lenalidomide-based regimens. We report an MM patient in his late 60s who received lenalidomide as maintenance treatment and whose condition was complicated with refractory postherpetic neuralgia. The patient received antiviral treatment and analgesia immediately after the diagnosis of herpes zoster. Two months later, the patient received acupuncture, radiofrequency treatment, and even spinal cord stimulation, which failed to relieve the pain. Consequently, we performed high-resolution magnetic resonance imaging of the cervical and thoracic nerves. Then, stellate ganglion block, left C5/C6/C7/C8 nerve root block, and left thoracic 1, 2 paravertebral nerve block were performed with the assistance of real-time ultrasound. The pain was immediately relieved after treatment; however, the symptoms reappeared 2 days later. At 5 months after treatment, the patient still experienced severe pain. We suggest that MM patients complicated with postherpetic neuralgia are refractory to treatment. Starting nerve block therapy, pulsed radiofrequency, and other interventional therapies as early as possible could be a more optimal treatment plan for these patients.
Keywords
Introduction
Herpes zoster (HZ) results from the presence of latent varicella zoster virus in ganglia. Postherpetic neuralgia (PHN) is the most common complication of HZ and occurs in 15% to 40% of HZ patients. It is defined as pain persisting for at least 3 months after the appearance of rash. 1 The primary pathophysiological mechanism is a neuronal lesion that affects somatosensory processing in the peripheral and central nervous systems. The pain can be constant or intermittent and is characterized by spontaneous or evoked burning, stabbing, or throbbing. In PHN, abnormal sensory symptoms such as hyperalgesia, allodynia, sensory loss, and pruritus are also common. 1 These symptoms can sometimes last for many years, thus severely interfering with sleep, disturbing the patient’s mood, and negatively affecting their quality of life. Patients with advanced age, immune insufficiency, immunosuppressive agents, or tumor are at high risk of developing HZ. 1
Multiple myeloma (MM) is a B-cell neoplasm characterized by the uncontrolled, destructive growth of plasma cells in the bone marrow. 2 In addition to the standard combination of prednisone, melphalan, and autologous stem cell transplantation, novel agents, including immunomodulatory drugs (thalidomide, lenalidomide) and proteasome inhibitors (bortezomib, carfilzomib), are the mainstay of therapy for MM. Because of the low rate of adverse reactions, lenalidomide has become the first-line drug for short-term and long-term treatment of MM. 3 Viral infection is a common complication of MM, and HZ has been considered a later complication after autologous stem cell transplantation or proteasome inhibitor treatment in MM patients. 4 However, HZ is not common in patients treated with lenalidomide-based regimens.
Herein, we report the clinical and neuropathic features, treatment, and prognosis of an older adult patient with MM who received lenalidomide for maintenance treatment and was complicated with refractory PHN. This report will provide a reference for hematologists and pain physicians to actively prevent and treat PHN.
Case presentation
Institutional review board/ethics committee approval for this report was obtained from the Institutional Review Board of the Tongji Hospital at Tongji Medical College, Huazhong University of Science and Technology (TJ-IR20210951). The reporting of this study conforms to the CARE guidelines. 5 Written informed consent for publication of the details of this case report was obtained from the patient. All patient details were also de-identified.
Our patient was a man in his late 60s who suffered from MM for 8 years and was given oral lenalidomide maintenance treatment for 2 years. His condition was complicated with HZ 8 months prior, after which he was diagnosed with PHN. He reported spontaneous intermittent acupuncture-like pain (numerical rating scale score 8–9; numerical rating scale: 0–10, where 0 indicates no pain and 10 indicates the most severe pain imaginable) when visiting our clinic. The patient had difficulty falling asleep at night, and his quality of life was markedly affected, which is why he consulted our clinic. The physical examination revealed clusters of herpes scars on the left back and left upper extremity along with allodynia and numbness. Allodynia mainly occurred on the left back and upper left arm where herpes scars were located, while the numbness mainly occurred in the skin innervated by the median and ulnar nerves (Figure 1). His hand muscle strength was grade 4.

Sensory test of skin with herpes scars. (a) Allodynia mainly occurred in the left back and left upper arm where herpes scars were located and (b) Numbness was mainly distributed in the skin innervated by the median and ulnar nerves. The blue dotted box shows the area affected by allodynia; the green dotted box shows the area affected by numbness.
After obtaining consent for treatment from the patient, he received antiviral treatment (valaciclovir, 0.3 g, bid for 10 days) after the diagnosis of HZ and at the same time took pregabalin (150 mg, bid), tramadol sustained-release tablets (1 tablet, qd), paracetamol and oxycodone (1 tablet, twice a day), and methylcobalamin (0.5 mg, once a day). Two months later, the pain persisted. Subsequently, the patient received acupuncture, radiofrequency treatment, and even spinal cord stimulation, none of which could effectively relieve the pain.
Therefore, we performed high-resolution magnetic resonance imaging (MRI) of the cervical and thoracic nerves to determine the degree and location of neuropathy before treatment. The left C5/C6/C7/C8 dorsal root ganglia and nerve roots were obviously swollen, and the median nerve was degenerated. Meanwhile, the ulnar nerve and radial nerve were also atrophied, but the left thoracic dorsal root ganglia were not markedly altered (Figure 2).
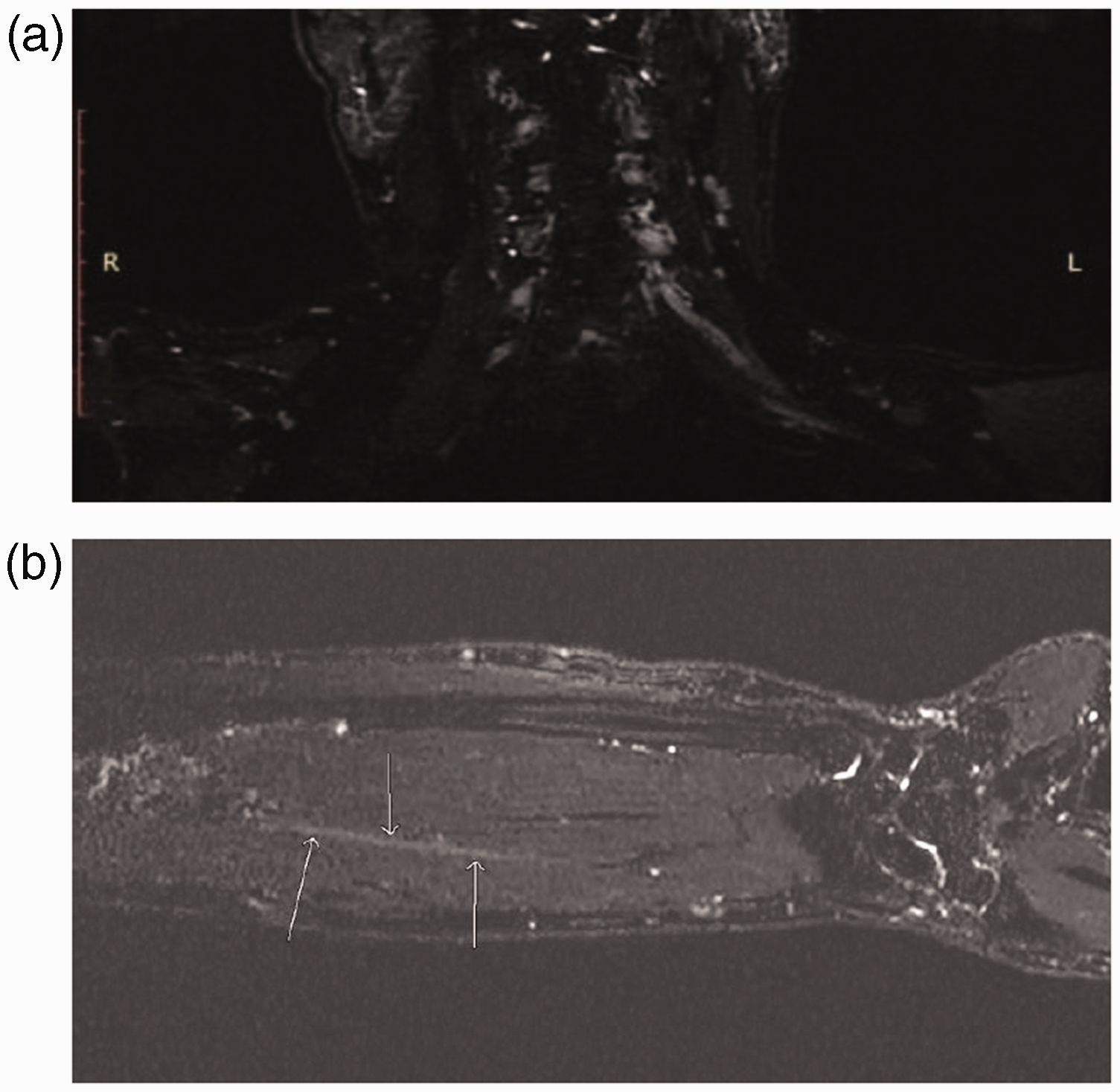
High-resolution magnetic resonance imaging of the cervical nerves. (a) The left C5/C6/C7/C8 dorsal root ganglia were substantially enlarged, and the corresponding nerve roots were obviously swollen and (b) The median nerve was degenerated; the arrows indicate the median nerve.
After careful discussion, a therapeutic strategy of blocking the sensory and sympathetic nerves was adopted. According to the MRI results and herpes dermatome, stellate ganglion block, left C5/C6/C7/C8 nerve root block, and left thoracic 1, 2 paravertebral nerve block were performed with the assistance of real-time ultrasound.
The pain was immediately relieved after treatment; however, the symptoms relapsed 2 days later. After 1 week, the same treatment was repeated, and the pain relief lasted for 2 days. Given the patient's neuropathy and the poor effect of local treatment, the nerve block treatment was stopped, and medication was continued.
One week and 1 month after treatment, the patient was treated with medication, and no substantial pain relief was observed. At the 3-month follow-up, the patient underwent repeat acupuncture treatment at another hospital, which did not improve the pain. Five months after treatment, the patient still experienced severe pain.
Discussion
Despite substantial progress in understanding the mechanisms and therapy of PHN, treatment of PHN is still difficult. Interviews have shown that up to 50% of patients with PHN are refractory to management. The varying degree of damage to the afferent transmission system is the core pathological mechanism underlying PHN, which leads to various sensory symptoms. 1
Because MM is a hematological malignancy with clonal plasma cell proliferation, MM-related neurological complications are relatively common; however, their pathophysiology is not clear. They can be caused by tumor tissue compression or direct infiltration of nerve tissue, leading to nerve damage. Chemotherapy-induced peripheral neuropathy is more common than MM-related neuropathy. However, peripheral neuropathy induced by bortezomib and thalidomide, which has been examined in many studies, has an incidence of more than 50%. 6 The pathological mechanism may be related to both genetic factors and dose-dependent neurotoxicity. Functional and pathological changes are most pronounced in unmyelinated peripheral sensory axons and to a lesser extent in dorsal roots and dorsal root ganglion cells. Chemotherapy-induced peripheral neuropathy usually presents as length-dependent axonal peripheral neuropathy (the longest axons are the earliest and the most severely affected), with long-term neuropathic pain. Demyelination of motor nerves has also been reported. 2 Although the incidence of lenalidomide-induced peripheral neuropathy is very low, it can still cause neurotoxicity. The degree of neuropathy is related to the accumulated dose. A previous study revealed that myeloma patients receiving long-term lenalidomide therapy developed sensory neuropathy; however, the neuropathy was usually subclinical or mild, with grade 1 peripheral neuropathy among patients with 2 years of lenalidomide therapy. 3
In this case, the patient presented with pain and numbness in the left upper extremity and decreased muscle strength in the left hand, which was associated with the brachial plexus. Our MRI results also confirmed this change. The cause of the patient’s nerve damage and whether it was related to MM were unclear. Further investigation into the patient’s history revealed that the patient presented with mild numbness in both hands without upper extremity pain several months prior to HZ onset. MRI results showed a mild cervical disc herniation, which might have caused the numbness in both hands. However, the patient had no history of neck and shoulder pain and no obvious symptoms of nerve compression on MRI (Figure 3). The above symptoms could not be well explained by cervical disc herniation. Meanwhile, the patient denied a history of diabetes. According to the findings, it was not possible to rule out MM-related neuropathy. However, because the MRI results showed no tumor invasion near the spinal cord, nerve roots, or ganglia, it was considered that lenalidomide was related to the numbness in the patient’s hands, excluding neuropathy directly caused by MM.

Magnetic resonance imaging of the cervical spine. (a) A mild cervical disc herniation at C3/4, C4/5, C5/6, and C6/7 and (b) No obvious symptoms of nerve compression were observed.
A recent study reported that peripheral neuropathy, caused by lenalidomide in 18% to 24% of cases, mainly presented with numbness and tingling of the hands and feet, all similar to the symptoms in the present case. 7 Therefore, we speculated that the patient suffered from peripheral neuropathy before the onset of HZ, which was then further aggravated by HZ. The MRI results, which revealed degeneration of the median nerve and atrophy of the ulnar and radial nerves, further supported this conclusion. Nonetheless, the left C5/C6/C7/C8 dorsal root ganglia and nerve roots were obviously swollen. A previous study indicated that MM-related peripheral neuropathy is difficult to diagnose and treat in clinical practice and that definite treatment is currently lacking. 8 In addition, there is no standard treatment for PHN, which means the treatment of MM-related peripheral neuropathy combined with PHN is difficult. Therefore, treatment with 400 mg acyclovir has been suggested to prevent HZ in MM patients receiving chemotherapy. 9 Pregabalin and gabapentin are also used to prevent peripheral neuropathy in MM patients. 10 However, there are no evidence-based therapies to prevent chemotherapy-induced peripheral neuropathy. Varicella zoster virus vaccine has been documented to reduce the incidence of HZ and PHN in MM patients. 11 Therefore, the vaccine may be a cost-effective therapy for MM patients.
After reviewing the entire course of the disease, we found that the patient was treated with medication only for the first 2 months after HZ onset, which may be considered conservative for this type of patient. Many studies have shown that early use of nerve block therapy and pulsed radiofrequency can reduce pain in patients with HZ and reduce the incidence of PHN.11–14 Kim et al recommended applying nerve block during the acute phase of HZ to prevent PHN. 15 However, because of the self-healing nature, some patients and doctors do not actively intervene in treating the acute phase of HZ. Therefore, it has been suggested that PHN should be defined as pain persisting for more than 1 month after the onset of rash, and this should be treated by more active intervention. Furthermore, the patient in this report is a man in his late 60s, and advanced age has been shown to be a high-risk factor for PHN. Therefore, interventional treatment of the patient as soon as possible may have been an appropriate choice. Nevertheless, because of the lack of relevant reports, prospective clinical studies involving hematology, dermatology, and pain departments are needed.
In conclusion, peripheral neuropathy in MM patients complicated with HZ and treated with lenalidomide tends to exhibit increased severity and complications. Starting nerve block therapy, pulsed radiofrequency, and other drug-based interventional therapies as early as possible may be an appropriate treatment plan for these patients. Additionally, preventive varicella zoster virus vaccination of MM patients should be advocated to reduce the incidence of HZ and PHN.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221123882 - Supplemental material for Refractory postherpetic neuralgia in a multiple myeloma patient with lenalidomide maintenance therapy: a case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605221123882 for Refractory postherpetic neuralgia in a multiple myeloma patient with lenalidomide maintenance therapy: a case report by Xueqin Cao, Gang Wu, Bo Jiao and Xianwei Zhang in Journal of International Medical Research
Footnotes
Author contributions
Xueqin Cao and Xianwei Zhang designed the research; Xueqin Cao and Gang Wu collected and analyzed the data and wrote the manuscript; Bo Jiao contributed to data collection and critically reviewed the paper.
Declaration of conflicting interest
The authors have no conflicts of interest to disclose.
Funding
The authors declare that this case has received no financial support.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.