
Abstract
Neurogenic tumors located in the larynx are extremely rare. Among them, schwannoma is a benign encapsulated tumor originating from Schwann cells, which form nerve fiber sheaths in the peripheral nervous system. We herein report a case of a schwannoma arising from a rare subsite of the larynx and review the literature on laryngeal schwannoma. The case involved a woman with a 1-month history of globus pharyngeus and dysphagia without dysphonia. Rigid laryngoscopy and magnetic resonance imaging showed a large submucosal bulge toward the medial wall of the right pyriform fossa, pushing the right false and true vocal cords and aryepiglottic fold inward. A transcervical approach was used to completely excise the tumor without incisional biopsy or preliminary tracheotomy. Histology confirmed a benign schwannoma originating from the right paraglottic space, which was extremely rare. During follow-up, no evidence of recurrence or a residual mass was found. The transcervical approach is a useful and less invasive treatment for laryngeal schwannoma located in the paraglottic space.
Introduction
Benign neurogenic tumors in the larynx are rare and account for only about 0.1% to 1.5% of all benign laryngeal tumors.1,2 Among them, the incidence of laryngeal schwannoma is higher than that of laryngeal neurofibroma. 3 Schwannoma is rare benign nerve sheath tumor arising from Schwann cells and originates from the cranial, sympathetic, and peripheral nerves. 4 Most laryngeal schwannomas are located at the aryepiglottic folds, false vocal cords, and arytenoid cartilages,5,6 whereas few are located at the true vocal cords, epiglottis, subglottis, ventricle, pyriform fossa, post-cricoid area, and interarytenoid region.7,8 Like schwannoma arising from other tissues, laryngeal schwannoma increases in volume over time. 5 As a latently slow-growing submucosal mass, the emerging symptoms of laryngeal schwannoma depend on its size, location, and direction.6,9,10 Patients usually present with multiple symptoms; few patients present with isolated symptoms.5,6 A retrospective case series at the Mayo Clinic 5 and a systematic review 6 revealed that the most common symptoms are dysphonia or hoarseness, followed by dysphagia. Laryngoscopy, enhanced computed tomography (CT), and enhanced magnetic resonance imaging (MRI) are usually applied to explore the size and extent of the lesion and the cellularity of the mass preoperatively. 6 Histopathology is indispensable for postoperative confirmation of the diagnosis of schwannoma. 6 We herein report a case of schwannoma arising from the paraglottic space, a subsite that has rarely been reported.
Case Description
A 55-year-old woman was referred to our otolaryngology department with a 1-month history of globus pharyngeus and dysphagia. Detailed history taking revealed no fever, odynophagia, dysphonia, dyspnea, cough, or bucking. Her remaining medical history was unremarkable. Rigid laryngoscopy showed a large submucosal bulge toward the medial wall of the right pyriform fossa, and the surface of the mass was smooth. The bulging right false vocal cord blocked our visualization of the right true vocal cord. Both true vocal cords could move normally (Figure 1(a) and (b)). Physical examination showed no abnormalities in the appearance of the neck, and no cervical mass was palpable. No unintentional weight loss had occurred, and no related family history was reported.

Laryngoscopic views of the submucosal tumor and resection of the tumor with the transcervical approach. (a, b) Rigid laryngoscopy views of the tumor. (c) Exposure of the mass during surgery and (d) The resected lesion sent for histology. The tumor is indicated by arrows.
CT at another hospital revealed a hypodense, round-to-oval mass measuring 15 × 21 mm in the right paraglottic space approaching the bottom of the right pyriform fossa. The mass had a clear capsule without calcification on the plain scan. After contrast enhancement, the mass exhibited heterogenic density with patchy areas of enhancement and low-density areas without enhancement, and the enhancement displayed gradualness. There was no sign of infiltrative growth or cartilaginous destruction, and there was no obvious enlargement of the lymph nodes in the bilateral neck.
The mass was isodense on T1-weighted MRI (Figure 2) and inhomogeneously hyperintense on T2-weighted MRI (Figure 3(a)–(c)). Diffusion-weighted imaging showed no diffusion restriction. The mass was smooth and had a clear border, and it exhibited regional inhomogeneous enhancement after contrast enhancement (Figure 3(d)–(f)). The right pyriform fossa had become shallower, the right false and true vocal cords and aryepiglottic fold were pushed inward, the right cricothyroid space was slightly widened while the glottic fissure was slightly narrowed, and the subglottic area and cervical esophagus were unobstructed. There were no signs of liquefaction or necrosis.
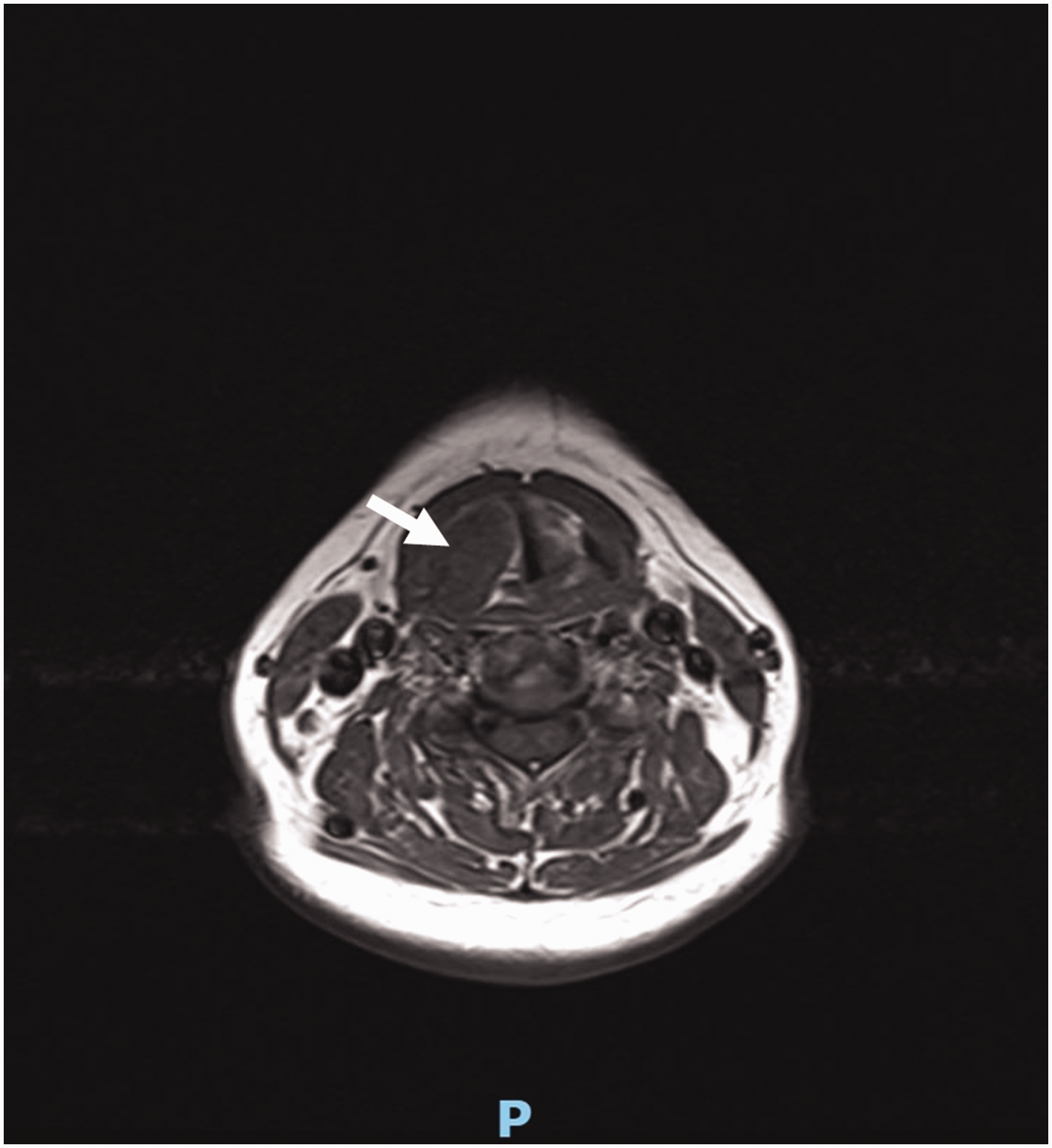
T1-weighted magnetic resonance imaging of the submucosal tumor, which is marked with an arrow.

T2-weighted magnetic resonance imaging of the submucosal tumor in the (a) transverse view and (b, c) coronal views. T1-weighted magnetic resonance imaging of the submucosal tumor after gadolinium injection in the (d) transverse view and (e, f) coronal views. The tumor is indicated by arrows.
After a preoperative discussion, the mass was considered a benign neurogenic tumor in the paraglottic space. Because of the large size of the tumor, a transcervical approach was used to completely excise the tumor (Figure 1(c) and (d)). A longitudinal incision was made in the right neck, and the skin and platysma muscle were cut to raise a platysma myocutaneous flap. After incision of the inferior pharyngeal constrictor, the thyroid cartilage plate was dissociated until the anterior half part was reached. The mass in the paraglottic space was palpated and found to be about 2.0 × 2.5 × 2.0 cm in size, and it was dissociated along the medial side of the thyroid cartilage plate. The mass was then dissociated from its surrounding tissues and radically resected. To avoid potential residual disease and recurrence,1,3 intraoperative incisional biopsy was not performed. Additionally, intraoperative tracheotomy was not performed because of the patient’s good airway condition.
Histological examination confirmed the diagnosis of laryngeal schwannoma with S-100 positivity (Figure 4(a) and (b)). The patient recovered smoothly and had a normal voice after surgery. She was asked to undergo an outpatient clinical follow-up every 3 months. At the 1-year follow-up, laryngoscopy revealed no evidence of recurrence or a residual mass. The patient’s voice quality was preserved, and she experienced no foreign body sensation during swallowing. The patient provided written informed consent for treatment and publication, and all patient details were de-identified. The reporting of this study conforms to the CARE guidelines. 11

Histologic appearance of the excised tumor. (a) Hematoxylin–eosin stain and (b) Positive stain for S-100.
Discussion
Schwannoma is a benign tumor originating from perineural Schwann cells. It is usually well encapsulated and can emanate from somatic or sympathetic nerves anywhere in the body except the optic and olfactory nerves. 6 Head and neck schwannoma accounts for approximately 25% to 45% of all schwannomas, most of which originate from the parapharyngeal spaces.5,6 The incidence of laryngeal schwannoma is extremely low.5,12 The internal branch of the superior laryngeal nerve is the most frequently involved nerve after penetrating the thyrohyoid membrane. 13
To attain the correct diagnosis, laryngoscopy is usually performed to obtain a direct view of the laryngeal schwannoma and potentially gain information on its subsite location, size, shape, scope of involvement, and effects on surrounding tissues, especially the mobility of the true vocal cords. 14 Some patients with pseudo-fixation present with similar symptoms of cricoarytenoid joint fixation, which should be carefully differentiated to avoid administration of inappropriate therapeutic regimens. 15
In addition, enhanced CT and enhanced MRI are generally used for diagnosis. For CT, most laryngeal schwannomas present as round or oval, well-defined, expansionary lesions inside the thyroid cartilage plate without invasion or cartilaginous destruction. Post-enhancement CT images usually show heterogeneous density and mild uneven enhancement within the schwannoma, exhibiting heterogeneous nodular high-density enhancement that is scattered in the low-density area.9,16,17 This might be due to the irregular distribution of remote hemorrhages and calcifications within the schwannoma. 16 Some researchers have reported that CT scans of schwannomas are also characteristic of centrally distributed low-attenuation areas surrounded by a peripheral enhancing ring.6,18 Schwannoma is isointense to slightly hyperintense on T1-weighted MRI and shows inhomogeneous enhancement after gadolinium injection, whereas this benign tumor is hyperintense on T2-weighted MRI.3,19 Moreover, there are no signs of diffusion restriction. 6 The imaging characteristics in our case were consistent with the reported features of laryngeal schwannoma.
Some researchers also use ultrasonography to assist in the diagnosis of head and neck schwannoma,20–22 but the clinical application of such imaging is limited in laryngeal schwannoma.6,17,23
For differential diagnosis, other submucosal lesions such as laryngocele, laryngeal cyst, adenoma, chondroma, mucocele, lipoma, and neurofibroma should be considered. 6 Among these, particular attention should be paid to neurofibroma. Although both types of laryngeal tumors are neurogenic, their source cells are different. Schwannoma originates from perineural Schwann cells, whereas neurofibroma originates from perineural fibrocytes. 1 Although schwannoma grows extrinsically and eccentrically away from the parental nerve fascicles, neurofibroma is typically entwined with the parental nerves. 3 Thus, surgical separation of the schwannoma from the nerve is theoretically possible, but this is not applicable to neurofibroma. 6
The final diagnosis of schwannoma is based on the histological examination findings. Schwannoma has a clear capsule consisting of Antoni A and Antoni B areas. Antoni A areas are cellular regions consisting of compact spindle cell bundles with twisted nuclei arranged in parallel palisades. Fibrillary cell processes with surrounding compact rows of well-aligned nuclei are called Verocay bodies. 3 In contrast, Antoni B areas are edematous regions that are loosely organized with myxomatous and cystic changes and loosely ordered cells and hypocellular regions with large, spaced vessels.13,24 Prominent vessels with thick hyaline walls are typically present. 17 Intense immunoreactivity for S-100 protein, especially in Antoni A areas, serves as the main diagnostic proof of schwannoma3,6 and was exhibited in our case.
Surgical excision is the only effective treatment for laryngeal schwannoma. The approach for excision of laryngeal schwannoma depends on the size and location of the mass. 13 The goal of surgery is complete resection of the tumor, preservation of laryngeal function, and mucosal coverage of the exposed cartilage.6,7
Smaller tumors confined to the glottis or supraglottic region and pedunculated lesions can be excised transorally or endoscopically.10,13 This approach leaves no external incision and ensures better preservation of laryngeal function; however, patients may develop a residual tumor and mucosal injury.7,8,25 Larger tumors, recurrent schwannomas, or tumors located at the pyriform sinus or subglottis must be excised via an external surgical approach.1,6,8 Median thyrotomy, lateral thyrotomy, and transhyoid pharyngotomy are typically used as external approaches.3,6 Yang et al. 8 recently reported the successful resection of a schwannoma in the interarytenoid region using an epiglottic root approach. External approaches guarantee better exposure and clear excision of tumors, but such approaches leave neck scars and a higher possibility of laryngeal function impairments.10,16 Considering that the transcervical approach can provide adequate exposure and better visibility of the paraglottic space with less threat to the voice, 26 this approach was adopted in our case. There is no consensus on the performance of preliminary tracheostomy during surgery for large tumors, 6 and we did not perform this procedure in our patient because of her good airway condition.
Patients who undergo incisional biopsy of laryngeal schwannoma are more likely to develop disease recurrence than those who do not undergo incisional biopsy. 10 Such recurrence might result from the discontinuity of the tumor and the covering mucosa, which would increase the risk of schwannoma relapse. 10 Piecemeal resection is also associated with recurrence. 27 Malignant transformation of schwannoma is very uncommon, and its risk is much lower than that of neurofibroma.3,13,16 Notably, as summarized by Tulli et al., 10 schwannoma with extralaryngeal extension is associated with neurofibromatosis type 2 or schwannomatosis. In such cases, close attentions should be paid to the possibility of hereditary syndrome. 10
We have herein reported a rare case of laryngeal schwannoma that arose from the paraglottic space and was excised using a transcervical approach without incisional biopsy or tracheotomy. Although the incidence of laryngeal schwannomas is rare, otolaryngologists should differentiate them from other benign laryngeal tumors. If the diagnosis of schwannomas is suspected based on the preoperative imaging findings, incisional biopsy should be avoided because total excision and protection of the surrounding structures are vitally important to prevent recurrence and preserve function during follow-up. When a less invasive approach is adopted, a more invasive approach should be considered as a second option in cases of non-ideal surgical exposure or incomplete excision of the tumor during the operation. 10
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221122497 - Supplemental material for Paraglottic space schwannoma: a case report and literature review
Supplemental material, sj-pdf-1-imr-10.1177_03000605221122497 for Paraglottic space schwannoma: a case report and literature review by Hui Chen, Yang Guo, Cai Li and Liang Zhou in Journal of International Medical Research
Footnotes
Author contributions
All authors were involved in the preparation of this manuscript. HC, CL, and LZ participated in the surgery. HC and YG wrote the manuscript. HC, YG, CL, and LZ revised the manuscript. All authors read and approved the final manuscript.
Consent for publication
Written informed consent for publication was obtained from the patient.
Declaration of conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Data availability statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics approval and consent to participate
The study protocol was approved by the Committee on Human Research of the Eye and ENT Hospital of Fudan University, and written consent to participate was obtained from the patient.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Shanghai Sailing Program [grant number: 21YF1405600] and National Natural Science Foundation of China [grant number: 81402237].
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.