
Abstract
An extraintestinal fistula is a rare complication after appendectomy. To our knowledge, this study is the first to report a case of sigmoid abdominal wall fistula after appendectomy in a 45-year-old male patient who underwent appendectomy due to acute appendicitis. Purulent discharge was noted at the abdominal wall incision wound for more than 1 year postoperatively. The patient's clinical manifestation, medical history, physical examination, and auxiliary examination all suggested the formation of an abdominal sinus. After exploratory laparotomy at the Digestive Disease Hospital, Affiliated Hospital of Zunyi Medical University, a diagnosis of sigmoid abdominal wall fistula was confirmed, and the fistula was cured after complete fistula resection. The reporting of this rare and atypical case may provide useful reference information for diagnosing and treating future cases of enterocutaneous fistula.
Keywords
Introduction
Acute appendicitis is the most common acute abdomen observed in clinics, with a reported lifetime risk of 7–8%. 1 Characterised by metastatic right lower abdominal pain, nausea, vomiting, and fever, severe cases of acute appendicitis may be accompanied by complications, such as perforation and peritonitis. Current standard treatment for appendicitis is an appendicectomy, which may be performed as an open or laparoscopic procedure. 2 Common complications following appendectomy include abdominal abscess, bleeding, incision infection, small intestinal obstruction, hernia, and stump appendicitis. Intestinal fistula is a rare complication after appendectomy, with a high incidence in the cecum. 3 The development of an intestinal fistula in the sigmoid colon is generally deemed impossible due to its distant anatomical position, resulting in a lack of diagnosis and treatment for this situation. Here, the rare case of sigmoid abdominal wall fistula after appendectomy is reported.
Case report
A 45-year-old male patient was admitted to the Digestive Disease Hospital, Affiliated Hospital of Zunyi Medical University, Guizhou, China, in May 2019, due to persistent purulent discharge at an abdominal wall incision wound for over 1 year following appendectomy.
The patient had previously undergone ‘open appendectomy’ at a local hospital in March 2018, because of ‘right lower abdominal pain for 1 day’. During the operation, the lower sigmoid colon was found to be thickened and adhered to the ileocaecal region and abdominal wall. While these adhesions were separated, the sigmoid lesions were not treated. Histopathology of appendectomy specimens suggested simple (acute) appendicitis. Postoperatively, the incision healed poorly, with white secretions and no faeces or intestinal fluid. No sigmoid mucosal lesion was detected by enteroscopy. The wound exhibited a breaking-healing-breaking characteristic during clothing change and treatment with antibiotics.
The patient was then admitted to a large tertiary hospital in January 2019. Physical examination revealed a 6-cm operational scar in the lower abdomen and a 4 × 4-cm sized mass could be palpated at the incision. The mass was hard, with mild tenderness and secretion, but without palpable fluctuation, and was not associated with rebound pain and muscle tension. Bacterial culture of the secretions showed extended-spectrum β-lactamase-producing bacteria. Gastrointestinal radiography revealed an abdominal wall abscess with sinus formation; and lower abdominal computed tomography and B-mode ultrasound showed right anterior and lower abdominal wall infection and abscess formation. Enteroscopy showed no abnormality, and ‘wound opening iodophor gauze drainage’ was performed. The infection was treated with cefuroxime plus metronidazole anti-infectives and the purulent discharge was significantly reduced. The patient was then discharged from the hospital.
The patient was admitted to the Digestive Disease Hospital, Affiliated Hospital of Zunyi Medical University in May 2019, and was noted to have a history of allergies to eggs and egg products. Physical examination showed that he was 167-cm tall (weight, 85 kg), and revealed a surgical scar (sized approximately 6 cm) on the right side of the umbilical cord, with a circular sinus orifice of approximately 0.5 cm in diameter in the middle of the scar. A small amount of white pus could be observed at the sinus orifice, but there was no surrounding redness or swelling; the skin temperature was not high, and there was no sense of fluctuation. Laboratory examination results were within normal ranges, and revealed the following: white blood cell count, 10.42 × 109/L; and lymphocyte count, 3.33 × 109/L. Magnetic resonance imaging showed a right lower abdominal sinus formation; the sigmoid colon and adjacent small intestinal wall thickening, oedema, and abdominal wall sinus internal orifice were unclear (Figure 1). Additionally, sinus retrograde imaging revealed a right lower abdominal sinus, sized 67 mm (Figure 2), and enteroscopy showed no organic lesions in the terminal ileum or colorectal mucosa (Figure 3). In June 2019, after eliminating any related surgical contraindications, the patient underwent exploratory laparotomy plus release of complex intestinal adhesion, plus resection of the abdominal sinus, plus partial resection of the sigmoid colon. During the operation, the abdominal sinus was found to communicate with the sigmoid colon (Figure 4), with straight forceps able to enter the sigmoid colon along the sinus. Postoperative pathology reports revealed that tissue submitted for examination showed acute and chronic inflammation with granulation and tissue hyperplasia. Postoperative diagnosis was: (1) abdominal fistula of the sigmoid colon; and (2) confirmation of appendectomy as a surgery. The patient’s general postoperative condition resulted in discharge at the end of June 2019. During 1 year of follow-up, there was no sigmoid fistula recurrence.

Representative abdominal magnetic resonance image from a 45-year-old male patient with persistent purulent discharge for over 1 year following appendectomy. Arrow indicates the unclear boundary between the internal orifice of the sinus and the sigmoid colon.
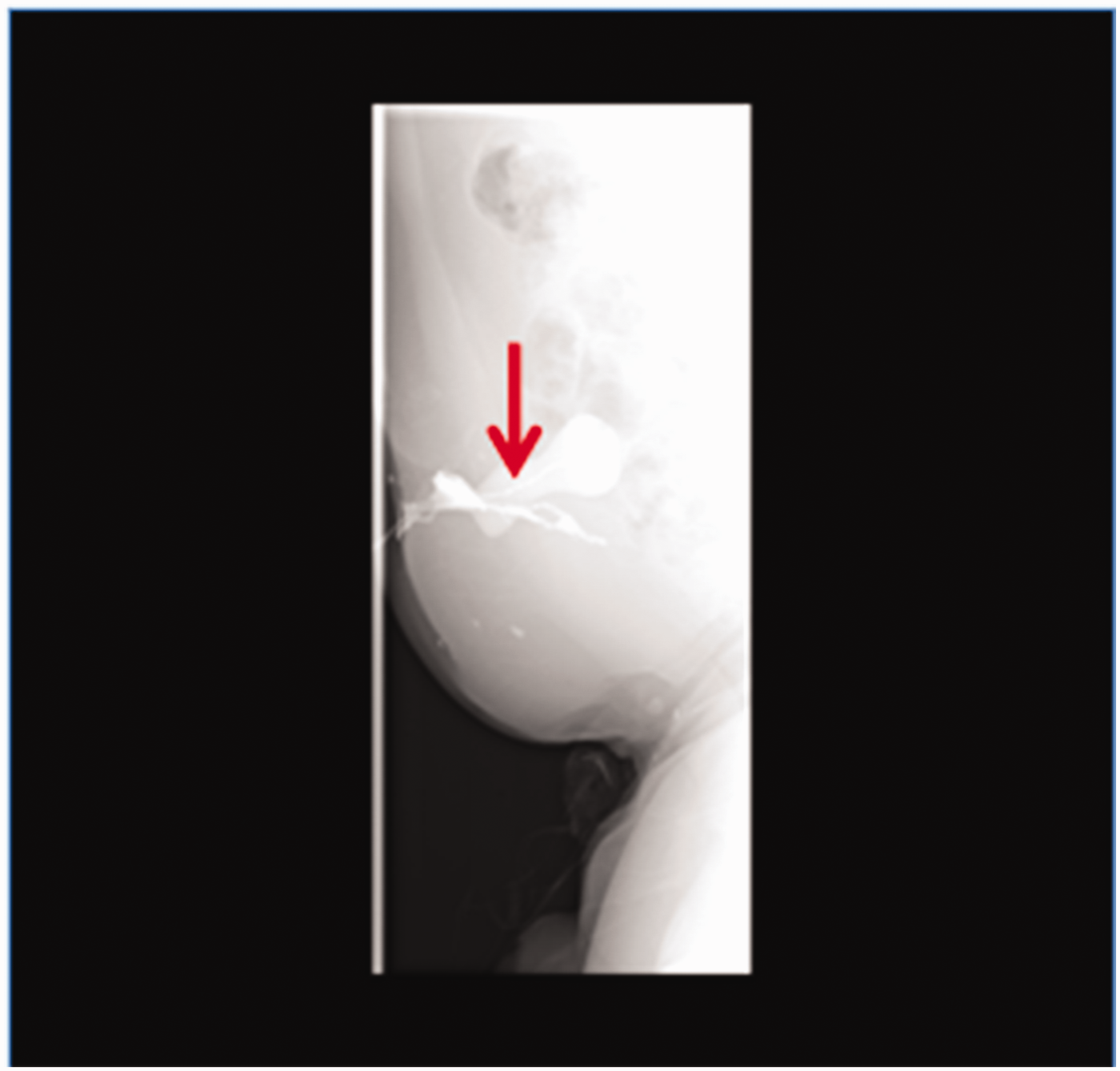
Representative sinus retrograde image from a 45-year-old male patient with persistent purulent discharge for over 1 year following appendectomy, showing a right lower abdominal sinus (arrow) sized approximately 67 mm.
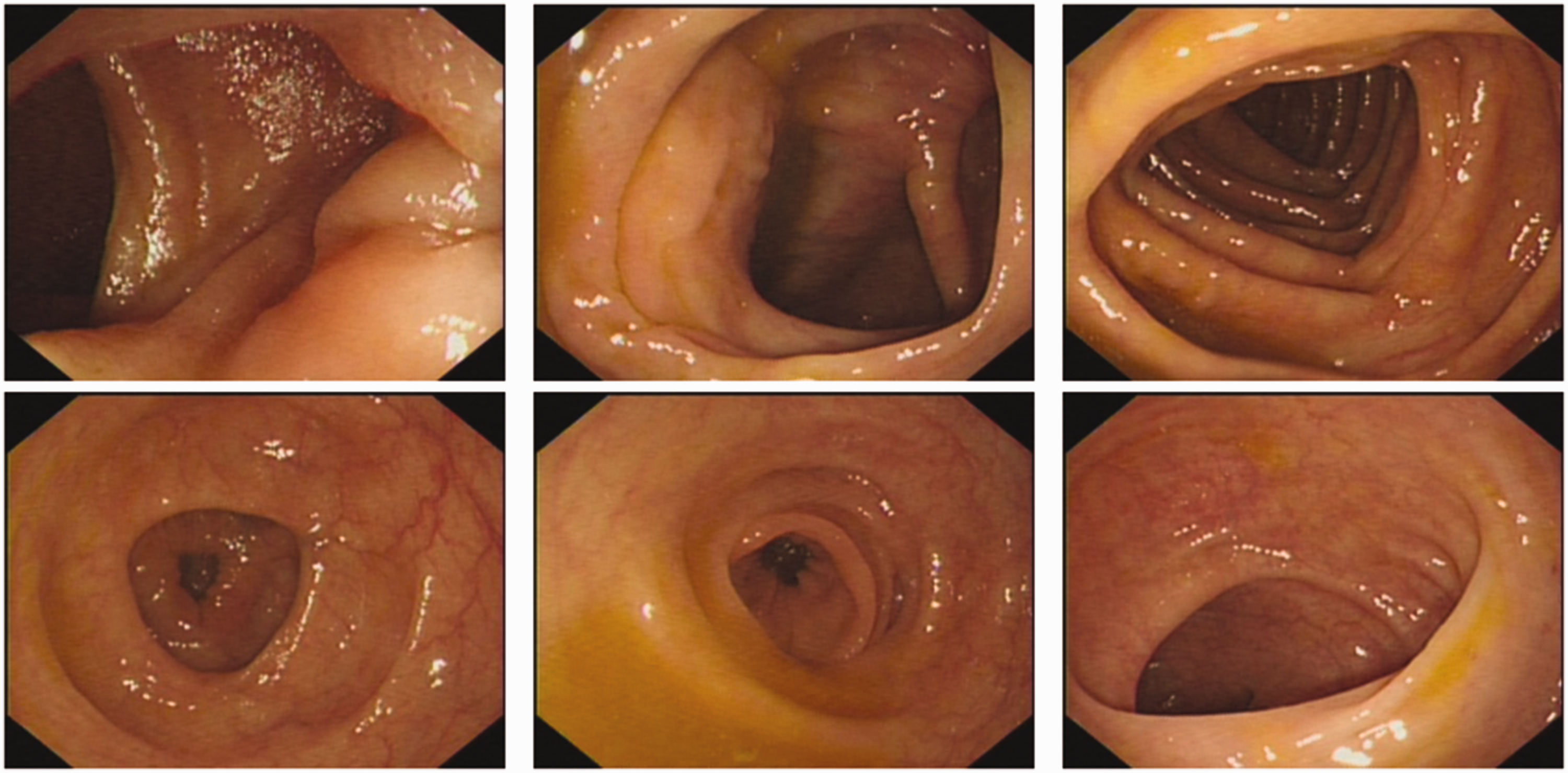
Representative enteroscopy images from a 45-year-old male patient with persistent purulent discharge for over 1 year following appendectomy, showing no organic lesions in the terminal ileum and colorectal mucosa.

Representative intraoperative images from a 45-year-old male patient with persistent purulent discharge for over 1 year following appendectomy, showing an abdominal sinus communicating with the sigmoid colon (arrows).
Ethics approval for this study was provided by the Affiliated Hospital of Zunyi Medical University and written informed consent was obtained from the patient to undergo the procedures described in this report and for report publication. The case report complies with CARE guidelines (https://www.equator-network.org/reporting-guidelines/care). 4
Discussion
Acute appendicitis is a common abdominal lesion that needs early surgical treatment after a definite diagnosis. The short-term complications of appendectomy include abdominal abscess, bleeding, and incision infection, while the long-term complications include small intestinal obstruction, hernia, and stump appendicitis. 5 Intestinal fistula refers to abnormal communication between the gastrointestinal tract and skin, which is often complicated by intraperitoneal sepsis. 6 Intestinal fistulas following appendectomy are uncommon. A search of the published literature revealed that an external fistula caused by appendectomy may include appendiceal faecal fistula and, more rarely, external pancreatic fistulas. 7 However, to the best of our knowledge, no case of sigmoid abdominal wall fistula after appendectomy has been reported previously.
The patient described in the present case underwent enteroscopy many times without any report of sigmoid mucosal injury. In other words, the physician did not detect the internal orifice of the fistula. At the same time, due to admission to different hospitals, the patient and their family could not recall the precise history of sigmoid colon lesions, or relevant auxiliary examinations and tests that indicated sinus formation and atypical clinical symptoms. Since such cases are rarely reported, it is difficult for doctors to treat this rare condition. In the present case, the attending doctor considered factors other than intestinal fistula, such as infection, insufficient use of antibiotics, inadequate drainage, allergic constitution, and obesity, which may have caused difficulties in wound healing and abdominal sinus formation. Only limited measures, such as dressing change, drainage, and antibiotic treatment, were taken, and as the fistula persisted and the incision was difficult to heal, the patient rotated through several hospitals for over a year.
The preoperative clinical manifestations, medical history, and examination of the present patient all suggested the formation of abdominal sinus, however, the lesion was confirmed as a sigmoid fistula only after intraoperative exploration, delaying disease treatment and increasing the associated pain. Therefore, in clinical settings following an appendectomy, if a fistula is not detected by enteroscopy but an incision does not heal after a long time, or forms a sinus, then attention should be paid to the formation of intestinal fistula and the rare situation of sigmoid abdominal wall fistula should be considered. The fistula occurred in the present case probably due to intragenic injury to the sigmoid colon during adhesiolysis at the time of open appendectomy. Hence, such complications may be avoided by meticulous dissection during a difficult appendectomy. Notably, an underlying malignancy, Crohn's disease, tuberculosis, or atypical mycobacterial infection might lead to postoperative sinus or fistula formation, 3 and these diagnoses should be ruled out in such cases. In the present case, these diagnoses could be ruled out on the basis of pathological results and other case data. Conversely, enterocutaneous fistula was suspected but could not be diagnosed before the second surgery due to the limitations of the investigations. Hence, instead of waiting for more than 1 year for a wound to heal, surgical exploration of the wound with or without laparotomy should be performed by expert surgeons if a wound fails to heal within 2–3 months. In addition, although the patient was finally diagnosed with sigmoid abdominal wall fistula after exploratory laparotomy at the Affiliated Hospital of Zunyi Medical University, laparotomy has some disadvantages, such as great trauma, high risk, and high cost. Therefore, the authors believe that simultaneous sinus exploration may represent a better option for patients undergoing enteroscopy, which is more conducive to atypical fistula detection, and this approach requires coordination among the various hospital departments. Finally, for this type of rare and atypical intestinal fistula, surgical resection remains the optimal treatment.
Footnotes
Acknowledgements
Author contributions
All authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Doctoral Research Startup Fund of the Affiliated Hospital of Zunyi Medical University (ZC220200604).