
Abstract
Objective
This study reviewed the current evidence on the clinical characteristics and outcome of acute pancreatitis (AP) following spinal surgery.
Methods
A systematic search was performed to identify English articles published through May 2020 in PubMed, Scopus, EMBASE, Latin American & Caribbean Health Sciences Literature, and Cochrane Library. Data on clinical characteristics, risk factors, and outcomes were analyzed.
Results
Eleven papers (including six case reports) were included, with 306 patients (incidence, 23.0%) developing AP after spinal surgery (mean age, 14.2 years). Of the studies that specified symptoms (55 patients), abdominal pain (43.6%), nausea and vomiting (32.7%), and abdominal distension (7.27%) were most prevalent. The mean duration from surgery to symptom onset was 6.15 days (range, 1–7). The most common complications of AP were glucose intolerance (25%), peritonitis (2%), pseudocyst formation (2%), and fluid collection (2%) were most prevalent. Prolonged fasting time (13.6%), intraoperative blood loss (9.09%), gastroesophageal reflux disease (9.1%), age >14 years (9.1%), and low BMI (9.1%) were most commonly associated with AP. Two deaths (0.6%) were reported.
Conclusion
AP remains an important complication of spinal surgery because of its morbidity and mortality. Avoiding major risk factors can reduce the incidence of AP following spinal surgery.
Keywords
Introduction
Acute pancreatitis is a known postoperative complication of many abdominal and extra-abdominal surgeries.1–5 Postoperative pancreatitis is associated with a higher risk of local and systemic complications as well as high morbidity and mortality rates. 6 The severity of pancreatitis ranges from mild to severe, with increasing mortality observed in patients with severe pancreatitis, necrotizing pancreatitis, and multiorgan failure. 7 In patients with postoperative pancreatitis, the mortality rate has been reported to be as high as 50%. 1 Although the incidence of postoperative pancreatitis is low, routinely monitoring with clinical and biochemical parameters can facilitate early diagnosis and treatment, especially among patients undergoing surgeries with a known high risk of pancreatitis. 8
A diagnosis of acute pancreatitis is considered if a patient satisfies at least two of the following criteria: clinical features including abdominal pain, nausea, and vomiting; biochemical features including serum lipase levels three times above the upper limit of normal; and characteristic findings in imaging including computed tomography (CT) or magnetic resonance imaging (MRI). 9
The pathogenesis of pancreatitis following spinal surgery is attributed to multiple factors such as splanchnic hypoperfusion caused by intraoperative hemodynamic instability,8,10 mechanical compression caused by spinal correction mainly in individuals with lower body mass index (BMI), pancreatic ischemia caused by lower intraoperative mean arterial pressures,8,11 and depressed trypsin inhibitor activity leading to reduced immunity to autodigestion postoperatively. 2 It has been observed that patients with neurofibromatosis type 1, Marfan syndrome, and cerebral palsy are at higher risk of developing acute pancreatitis following spinal surgery, although the exact mechanism of the higher risk among these patients is poorly understood. 8
The available literature on acute pancreatitis following spinal surgery is limited. Therefore, we conducted this systematic review to describe the clinical characteristics, risk factors, and outcomes of acute pancreatitis among patients undergoing spinal surgeries.
Methods
A systematic review of all studies on pancreatitis following spinal surgeries, including prospective and retrospective cohort analysis and experimental studies, was performed. Because of the limited number of studies, we decided to include case reports in this review. Studies describing patients meeting at least two of the three criteria of acute pancreatitis after any spinal surgery were eligible. As a systematic review, ethics committee approval and patient consent were not required.
The primary objective was to describe the clinical characteristics, risk factors, and outcomes of acute pancreatitis following spinal surgeries. We also aimed to describe attempted treatment modalities and their outcomes when relevant. The methodology of this review followed the PRISMA recommendations. 12
Search strategy
All articles published before May 2020 were searched electronically using PubMed/Medline, Scopus, EMBASE, Cochrane Central Register of Controlled Trials (CENTRAL), and Latin American & Caribbean Health Sciences Literature (LILACS) without any restrictions regarding language or the publication status. Keywords related to acute pancreatitis and its complications and various types of spinal surgeries were searched in the title and abstract fields. The detailed search strategy is presented in the supplementary file (Annexure 1). Furthermore, the list of references of eligible articles was manually searched, and relevant articles were added to the review.
The initial eligibility screening was performed by two investigators using the titles, abstracts, and keywords of the citations. Thereafter, the full text of all relevant records was assessed according to the inclusion criteria. In cases of disagreement, a consensus was reached after input from the senior authors. All data pertaining to the clinical presentation, risk factors, investigations, treatment and outcomes were extracted, categorized, and tabulated. Finally, qualitative analysis was performed using the available data. A meta-analysis could not be performed because of the heterogeneity in the study methodology, treatment options, and description of outcomes. The risk of bias assessment of eligible studies was performed using the Downs and Black checklist, which is a valid and a reliable tool for assessing both randomized and non-randomized control studies (external validity, KR20 = 0.54; internal consistency, KR20 = 0.89), 13 and the findings are presented in Table S1.8,10,13–30
Results
Overall summary and patient characteristics
The search of PubMed/Medline, Scopus, EMBASE, CENTRAL, and LILACS resulted in 687 citations. After excluding duplicates, 620 were evaluated for eligibility. Of these, 598 papers were excluded after reviewing the titles and abstracts. The full texts of the 22 remaining papers were assessed for eligibility. Of these papers, 11 were excluded because the full text did not meet the inclusion criteria. Finally, 11 manuscripts, including six case reports and five cohort studies, were included in this systematic review. No relevant unpublished studies were obtained. The included studies described a total of 1326 patients, of whom 306 patients (23%; mean age, 22.2 years; 68.3% female [n = 209]). Three studies included children with cerebral palsy, and eight studies included patients undergoing surgery for scoliosis (Supplementary File S1).
Clinical symptoms and signs
Of the studies that specified symptoms (n = 55), abdominal pain (43.6%, n = 24), nausea and vomiting (32.7%, n = 18), and abdominal distention (7.3%, n = 4) were most prevalent. The other described features included reduced bowel sounds (5.4%, n = 3), food intolerance (3.6%, n = 2), and prolonged ileus (3.6%, n = 2). These clinical features appeared after a mean of 6.1 days after surgery (Table 1).
Clinical characteristics of acute pancreatitis following spinal surgeries.

AP, acute pancreatitis; NA, not available.
Biochemical findings
Only studies reporting serum amylase elevation of more than three times the upper limit of normal were included; therefore, all studies and case reports reported an elevation of serum amylase levels. Serum lipase elevation was observed in 65% of patients (n = 199; Table 2).
Investigation findings of acute pancreatitis following spinal surgeries.
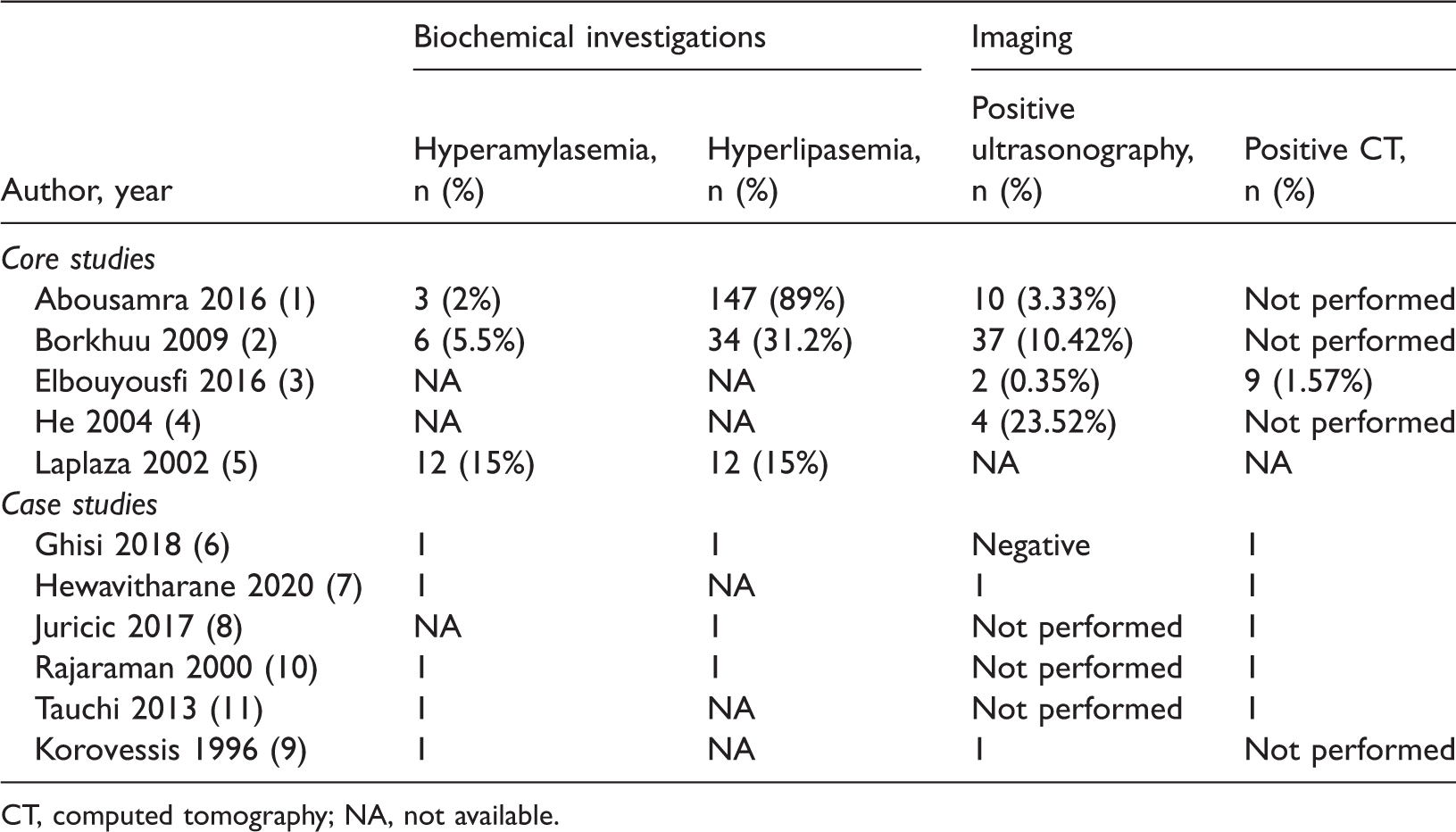
CT, computed tomography; NA, not available.
Imaging findings
Only studies that included definitive imaging evidence of acute pancreatitis were included. Although, all studies and case reports included imaging findings, only 24.5% (n = 75) of patients had detailed imaging data. Of these patients, 81.3% (n = 61) underwent abdominal ultrasound, and the remaining 18.6% (n = 14) underwent CT (Table 2).
Treatments used
All but one patient was treated non-operatively nil by mouth with nasogastric suction, intravenous fluids, somatostatin, and intravenous antibiotic prophylaxis until clinical improvement was observed. Four patients received total parenteral nutrition, and one patient needed total parenteral nutrition. One patient underwent surgery for corporeal fracture of the pancreas postoperatively after correction of the spinal deformity (Table 3).
Management, complications, and outcomes of acute pancreatitis following spinal surgeries.

ICU, intensive care unit; UTI, urinary tract infection; NA, not available; CP, chronic pancreatitis
Risk factors
Three studies identified a prolonged fasting time (13.6%), intraoperative blood loss (9.1%), gastroesophageal reflux disease (9.1%), age >14 years (9.1%), low BMI (9.1%), and an anterior or combined approach (9.1%) as the most common risk factors of acute pancreatitis. Risk factors such as the duration of surgery, total parenteral nutrition, feeding difficulty, reactive airway disease, increased TNF-alpha levels, urine trypsin-associated peptide levels, male sex, gastrointestinal tube placement, reactive airway disease, anemia, and the duration of surgery were also associated with acute pancreatitis, albeit at lower frequencies (4.5%, n = 1).
Complications
The common complications of acute pancreatitis were glucose intolerance (25%, n = 4), peritonitis (12.5%, n = 2), pseudocyst formation (12.5%, n = 2), and fluid collection (12.5%, n = 2). Other complications including pancreatic pseudocyst formation, pancreatic ascites, and fluid collection were found in 7.1% of patients (n = 2). A minority (6.2%, n = 1) of patients had complications including septicemia, severe pancreatitis, multiorgan failure, phrenic abscess, ascites, and pancreatic duct rupture. The mean hospital stay and intensive care unit stay were 22.1 and 5.4 days, respectively. Two deaths (0.6%) were reported. Of these deaths, one patient died of severe pancreatitis 48 hours after surgery, and the other died 1 month after surgery from multiorgan failure attributable to complications of pancreatitis, including pancreatic duct rupture and leakage with pseudocyst formation and acute digestive peritonitis (Table 3).
Discussion
Acute pancreatitis occurring following spinal surgery can severely disrupt the postoperative course, leading to unexpected morbidity and mortality. 15 It is associated with a relatively high mortality rate of 10% to 45% because of its potential to evolve into life-threatening systemic disease.31,32 Postoperative pancreatitis occurs following several surgeries, including both abdominal and extra-abdominal surgeries, although it occurs mostly following gastric and hepatobiliary surgery. 2 However, few studies have described its occurrence following spinal surgery. To our knowledge, this is the first systematic review of the clinical characteristics and outcomes of acute pancreatitis following spinal surgery.
Overall, the evidence suggests that acute pancreatitis is an uncommon yet important postoperative complication following spinal surgery. The studies included in our review described 306 patients who developed AP postoperatively. The incidence of acute pancreatitis ranged from 0.2% to 7.4% in the published studies. 8
The exact cause for postoperative pancreatitis has not been identified, although several mechanisms have been postulated. A study by Curtin et al. found that suboptimal positioning during surgery causing trauma to the pancreas might be a contributing factor. 33 Korovessis et al. identified a prolonged surgical time and the receipt of hypotensive anesthesia, which can cause ischemic injury in the pancreas, as potential causes of acute pancreatitis. 30 A study by Leichtner et al. found that intraoperative blood was significantly higher in patients who developed postoperative pancreatitis than in their counterparts. However, this study failed to demonstrate a relationship with hypotension. 23 Although medications are well-known causes of acute pancreatitis, its true incidence is low, ranging from 0.1% to 2%.34.35 Direct trauma in the abdominal region has been found to play a role in the development of acute pancreatitis following gastric and hepatobiliary surgery. 2 However, causes such as perioperative hypotension and reduced cardiac output were identified as major risk factors for postoperative acute pancreatitis in surgeries performed in non-abdominal regions. 31 A study by Rajaraman et al. on acute pancreatitis following anterior lumbar interbody fusion concluded that significant blood loss, the use of hypotensive anesthesia, and an anterior spinal approach should make surgeons take extra caution and stay vigilant concerning a possibility of acute pancreatitis, especially when patients develop prolonged postoperative ileus. Several common risk factors for developing acute pancreatitis were identified in the current review. A prolonged fasting time (13.6%), intraoperative blood loss (9.1%), gastroesophageal reflux disease (9.1%), age >14 years (9.1%), low BMI (9.1%), and an anterior or combined approach (9.1%) were the most common risk factors, whereas the duration of surgery, total parenteral nutrition, feeding difficulty, reactive airway disease, increased TNF alpha levels, urine trypsin-associated peptide levels, male sex, gastrointestinal tube placement, reactive airway disease, anemia, and the duration of surgery were also associated with acute pancreatitis, albeit in fewer patients.
A study by El Bouyousfi et al. on acute pancreatitis following scoliosis surgery revealed that pancreatitis occurred in the first 10 days after surgery, in line with the present study, in which symptoms appeared a mean of 6.2 days after surgery. Furthermore, they concluded that abdominal pain in postoperative acute pancreatitis was less typical and less frequent in comparison to that caused attributable to other common etiologies including alcohol or gallstones. However, symptoms such as nausea, prolonged ileus, and vomiting were more common in acute pancreatitis following surgery, possibly caused by the combined effect of acute pancreatitis and surgery itself. 16 Among patients receiving systemic opioids after surgery, prolonged ileus beyond 48 to 72 hours after surgery suggests the possibility of pancreatitis because these symptoms typically should regress within 48 to 72 hours.36,37 Although the most common symptoms identified in the current review were abdominal pain, nausea and vomiting, and abdominal distention, other symptoms including food intolerance, prolonged ileus, and reduced bowel sounds were described in a minority of patients. It is often difficult to link postoperative fever to acute pancreatitis because postoperative inflammation and infection must be excluded before seeking an alternative diagnosis, including acute pancreatitis. 16
Biochemical testing for serum lipase and amylase is performed to establish a diagnosis of acute pancreatitis, with serum lipase being superior to serum amylase, even in the postoperative setting. 38 In the present review, only 65% of patients displayed elevated serum lipase levels. Early imaging is unlikely to be useful in patients with typical clinical features of acute pancreatitis, even with supportive abnormal biochemistry to establish a positive diagnosis, in the postoperative setting. 39 Abdominal ultrasonography has proven to be of little benefit in the diagnosis of acute pancreatitis in adults; thus, CT is the most commonly used imaging modality in adults. 40 The drawbacks of abdominal ultrasound include its operator-dependent nature and poor visualization attributable to interposition of the hollow viscera, leading to a higher rate of false negatives that is more pronounced in patients who underwent abdominal surgery.23,38 In the present review, 81.3% (61/75) of patients underwent abdominal ultrasound, and the remaining patients (18.6%, n = 14) underwent CT.
Postoperative acute pancreatitis is associated with a high mortality rate, reaching 12% to 13%, and approximately 27% and 53% of patients develop severe pancreatitis and other major complications associated with pancreatitis, respectively. 6 The mortality rate of patients in the present study was 0.7%, which was considerably lower than the rates reported in the literature. However, complications such as sepsis were relatively more common (28.5%). Only 6.2% of patients in the present review developed severe pancreatitis, which was a much lower rate than those described in the literature for postoperative acute pancreatitis. Other complications of pancreatitis including pancreatic pseudocyst formation, pancreatic ascites, and fluid collection were found in a minority (6.2%) of patients.
There were several limitations in the present review. The main limitation was that the patient populations, clinical characteristics, types of spinal surgery, and outcomes varied widely across the included studies. Furthermore, there was considerable variability in the quality of studies because most studies were cohort studies and there were no published randomized control trials providing high-quality evidence. However, the risk of bias of the selected studies was minimal.
Conclusions
Although uncommon, acute pancreatitis remains an important postoperative complication of spinal surgery because of its associated morbidity and mortality. Avoiding major risk factors including prolonged fasting and minimizing intraoperative blood loss can help to reduce the incidence of acute pancreatitis in patients undergoing spinal surgery. Delays in diagnosis because of masked symptoms in patients after spinal surgery remain a challenge. A high index of suspicion and a low threshold for both biochemical and radiological investigations could facilitate an earlier diagnosis and thereby minimize both short- and long-term complications.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221121950 - Supplemental material for Clinical characteristics and outcomes of acute pancreatitis following spinal surgery: a systematic review
Supplemental material, sj-pdf-1-imr-10.1177_03000605221121950 for Clinical characteristics and outcomes of acute pancreatitis following spinal surgery: a systematic review by Ravindri Jayasinghe, Sonali Ranasinghe, Chandrani Kuruppu, Umesh Jayarajah and Sanjeewa Seneviratne in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605221121950 - Supplemental material for Clinical characteristics and outcomes of acute pancreatitis following spinal surgery: a systematic review
Supplemental material, sj-pdf-2-imr-10.1177_03000605221121950 for Clinical characteristics and outcomes of acute pancreatitis following spinal surgery: a systematic review by Ravindri Jayasinghe, Sonali Ranasinghe, Chandrani Kuruppu, Umesh Jayarajah and Sanjeewa Seneviratne in Journal of International Medical Research
Supplemental Material
sj-pdf-3-imr-10.1177_03000605221121950 - Supplemental material for Clinical characteristics and outcomes of acute pancreatitis following spinal surgery: a systematic review
Supplemental material, sj-pdf-3-imr-10.1177_03000605221121950 for Clinical characteristics and outcomes of acute pancreatitis following spinal surgery: a systematic review by Ravindri Jayasinghe, Sonali Ranasinghe, Chandrani Kuruppu, Umesh Jayarajah and Sanjeewa Seneviratne in Journal of International Medical Research
Footnotes
Author contributions
UJ and SS conceived the research idea. RJ, SR, CK, and UJ were involved in data curation, analysis, investigation, methodology, and initial draft writing. CK was involved in the formal academic literature search and methodology. SS was the senior author and supervisor, and he revised the final manuscript. All authors have read and agreed to the published version of the manuscript.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
INPLASY Registration number: INPLASY202270017, DOI number: 10.37766/inplasy2022.7.0017
Declaration of conflicting interest
All authors declare that there is no conflict of interest.
Funding
None.
Supplemental files
S1: PRISMA flowchart
Table S1: Risk of bias analysis of the included studies
S2: PRISMA checklist
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.