
Abstract
Objective
Platelet-rich plasma (PRP) is a novel treatment option for vitiligo. PRP has been reported to be effective in combination with 308-nm excimer laser therapy, but there is no consensus on their combination use. Therefore, this meta-analysis assessed the efficacy and safety of the combination regimen in patients with vitiligo compared with laser therapy alone.
Methods
The meta-analysis was performed by searching PubMed, EMBASE, Web of Science, Cochrane Library, Chinese National Knowledge Infrastructure, and WanFang to identify relevant publications published through 1 February 2022.
Results
Six studies involving 302 patients were included. Compared with phototherapy alone, combination treatment with PRP and 308-nm excimer laser therapy significantly improved the total response rate and reduced the no response rate. Additionally, the proportions of patients with repigmentation rates of ≥75%, ≥50%, and ≥25% were significantly higher in the combination group than in the monotherapy group. In addition, the rates of adverse events for combination therapy were comparable to those for laser therapy alone, and the recurrence rates were low.
Conclusions
This meta-analysis provided evidence supporting the combined use of PRP and 308-nm excimer laser therapy as a valuable treatment modality for patients with vitiligo based on its superiority to monotherapy.
Keywords
Introduction
Vitiligo is an acquired depigmentation disorder characterized by circumscribed white maculae attributable to the absence of functional melanocytes, and its global prevalence ranges from 0.5% to 1%. 1 Half of all cases of vitiligo develop before the age of 20, and the condition can persist through patients’ lives. 2 Thus, vitiligo has devastating impacts on patients’ cosmetic beauty and social and psychosocial health. Currently, the pathophysiological cause of vitiligo is unclear,1,3 and thus, treatment remains challenging. Several treatment options are recommended, including topical and systemic drugs, phototherapy, laser therapy, and surgery, as well as the use of make-up.4–6
Meanwhile, the 308-nm excimer laser has proven to be an effective phototherapy for the treatment of vitiligo. 7 The mechanisms of action of the 308-nm excimer laser in the treatment of vitiligo might include the induction of T cell apoptosis and stimulation, proliferation, and migration of melanocytes. 8 However, 308-nm excimer laser therapy alone requires a long treatment course (several months or even years), and long-term irradiation poses a potential risk of carcinogenesis. 9 Platelet-rich plasma (PRP) consists of a high number of platelets and high concentrations of growth factors. 10 PRP was recently demonstrated to stimulate the differentiation, proliferation, and maturation of melanocytes and keratinocytes, 11 which participate in the pathogenesis of vitiligo.
Multiple clinical trials investigated the effectiveness of PRP in combination with NB-UVB, 12 excimer laser, 13 fractional CO2 laser, 14 and vitamin D 15 therapy in treating vitiligo, finding that combined treatment can enhance outcomes and reduce the occurrence of adverse events. The efficacy of PRP plus 308-nm excimer laser therapy compared with 308-nm excimer laser therapy alone remains uncertain, and no quantitatively synthesized analyses have been performed. In this study, we performed a meta-analysis to evaluate the efficacy and safety of 308-nm excimer laser monotherapy compared with PRP combined with 308-nm excimer laser therapy for the treatment of vitiligo.
Materials and methods
Search strategy
We performed a comprehensive search according to the PRISMA guidelines using English and Chinese databases (PubMed, EMBASE, Web of Science, Cochrane Library databases, Chinese National Knowledge Infrastructure, and WanFang) from inception to 1 February 2022. The subject search terms were as follows: “vitiligo,” “platelet-rich plasma,” “platelet concentrates,” “PRP,” “excimer,” “excimer laser,” and “308-nm excimer laser.” All relevant studies were independently screened by two reviewers (Jiaoquan Chen and Nanji Yu). In error, we did not prospectively register this trial, but we registered it retrospectively at PROSPERO Registry (registration number 344780). As a secondary research project, the requirements for informed consent and ethics approval were waived.
Study selection
The title and abstract of all relevant articles were screened and selected using the following inclusion criteria: (1) randomized controlled trials; (2) patients with a diagnosis of vitiligo; (3) the experimental group was treated with PRP and 308-nm excimer laser therapy, whereas the control group was only treated with 308-nm excimer laser therapy; and (4) the outcomes included the rate of repigmentation (≥25%, ≥50%, ≥75%, and no response), recovered area, side effects, and recurrence. The exclusion criteria were as follows: (1) duplicate publication; (2) non-randomized clinical trials, retrospective or observational studies, comments, letters, and guidelines; (3) appropriate outcomes were not reported; and (4) full text was not available. Any disagreements between reviewers were resolved by discussion to reach a consensus.
Data extraction and quality assessment
The final eligible articles in this analysis were screened by two reviewers independently. Basic information extracted from all eligible studies included the first author, publication year, number of patients (experimental and control groups), patients’ characteristics (age, sex), details of interventions and comparisons, follow-up duration, and outcomes. The risk of bias was independently evaluated by two authors using the Cochrane collaboration risk-of-bias instrument. Disagreements regarding the final included articles were resolved through discussion with a third author.
Statistical analysis
The meta-analysis was performed using RevMan 5.3 software (The Cochrane Collaboration, Copenhagen, Denmark). In this study, the risk ratio (RR) and 95% confidence interval (CI) were used as the summary statistics for analyzing dichotomous outcomes (the rates of repigmentation, adverse events, and recurrence). The recovered area was analyzed using the mean difference (MD) and 95% CI. Heterogeneity was assessed using the I2 statistic. A fixed-effects model was used when I2 < 50%. A random-effects model was adopted when I2 > 50%. P < 0.05 indicated statistical significance for all analyses. Subgroup analysis was conducted according to the different proportions of repigmentation and different side effects.
Results
Description of the studies
In total, 85 publications were identified from six databases. Among them, 61 articles were excluded for duplication, and 11 were removed after reviewing the titles and abstracts. Then, the full text of 13 studies was reviewed for inclusion. After reviewing the full text, seven studies were excluded for the following reasons: lack of controlled studies (n = 2), inappropriate control group (n = 1), and review article (n = 4). Eventually, six articles13,16–20 were eligible for the meta-analysis (Figure 1). The included studies were published between 2019 and 2021, and they included a total of 302 patients, including 188 women and 114 men. These studies were conducted in China (four trials) and Egypt (two trials). Detailed information on the included studies is presented in Table 1.
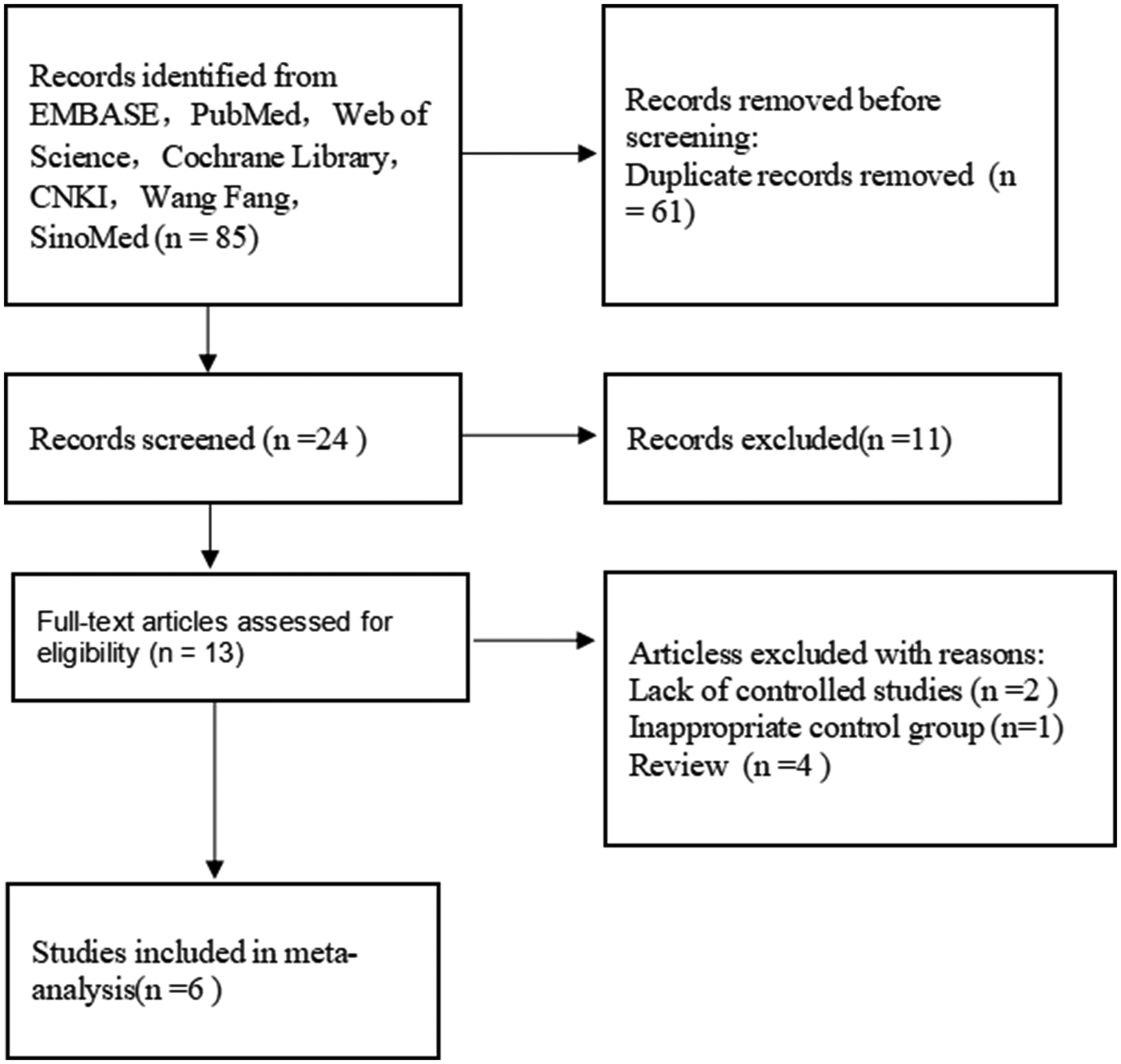
Flow chart of the study selection process.
Characteristics of the included studies.

PRP, platelet-rich plasma.
Bias risk of the included trials
Regarding study quality, Figure 2 presents the results of the assessment for each item presented as percentages across all included studies. For random sequence generation, five studies were considered to have a low risk of bias,13,16,18–20 and one study had an unclear risk. 17 Three articles provided adequate information on allocation concealment including the picked cards, 16 light-proof envelope, 13 and unique numbers. 18 Only one study 18 had a low risk of performance bias (blinding of participants and personnel). Regarding the blinding of the outcome assessment (detection bias), five studies13,17–20 had an unclear risk of bias, and one study 16 had a low risk of bias. Concerning incomplete outcome data and other types of bias, we considered that all studies had a low risk of bias.

Risk of bias graph.
Effects of PRP plus 308-nm excimer laser therapy compared with 308-nm excimer laser therapy alone
Six studies reported the rates of repigmentation (≥25%, ≥50%, ≥75%, and no response) as the primary outcome. As presented in Figure 3a, PRP plus 308-nm excimer laser therapy was considered superior to 308-nm excimer laser monotherapy (RR =1.32, 95% CI = 1.22–1.44, P < 0.00001, I2 = 64%), including better rates of ≥75% repigmentation (RR = 1.67, 95% CI = 1.16–2.41, P = 0.006, I2 = 62% in four studies),13,16,18,20 ≥50% repigmentation (RR =1.37, 95% CI = 1.19–1.59, P < 0.0001, I2 = 61% in six studies),13,16–20 and ≥25% repigmentation (RR = 1.22, 95% CI = 1.12–1.33, P < 0.00001, I2 = 62% in six studies).13,16–20 In addition, the overall pooled RR for patches or patients receiving combination therapy was 0.36 (95% CI =0.22–0.61, P = 0.0001, I2 = 0% in five studies)16–20 for no response (Figure 3b), revealing a significant benefit of combination therapy.

Rates of repigmentation in the 308-nm excimer laser monotherapy and PRP and 308-nm excimer laser combination therapy groups. (a) Rates of ≥25%, ≥50%, and ≥75% repigmentation and (b) Rate of no response.
Furthermore, two studies17,19 also documented the recovered area in the two groups and found that the recovered area was significantly larger in the combination therapy group than in the monotherapy group (MD = 5.94; 95% CI = 5.47–6.41; P < 0.00001, I2 = 99%; Figure 4).

Recovered area in the 308-nm excimer laser monotherapy and PRP and 308-nm excimer laser combination therapy groups.
Adverse events
The adverse events reported in four articles include burning sensation, hyperpigmentation, and erythema, all of which were minor, transient, and tolerable in both groups. Pooled data analysis illustrated that the incidence of adverse events did not differ between the combination and monotherapy groups (RR = 0.85, 95% CI = 0.62–1.17, P = 0.32, I2 = 0%). In subgroup analysis, no difference in the incidence of burning sensation (RR = 1.22, 95% CI = 0.55–2.73, P = 0.62, I2 = 0% in two studies),16,17 hyperpigmentation (RR = 0.85, 95% CI = 0.56–1.29, P = 0.44, I2 = 0% in three studies),16,17,19 and erythema (RR = 0.69, 95% CI = 0.39–1.22, P = 0.20, I2 = 53% in two studies)16,18 was detected between the combination therapy and monotherapy groups in the treatment of vitiligo (Figure 5).
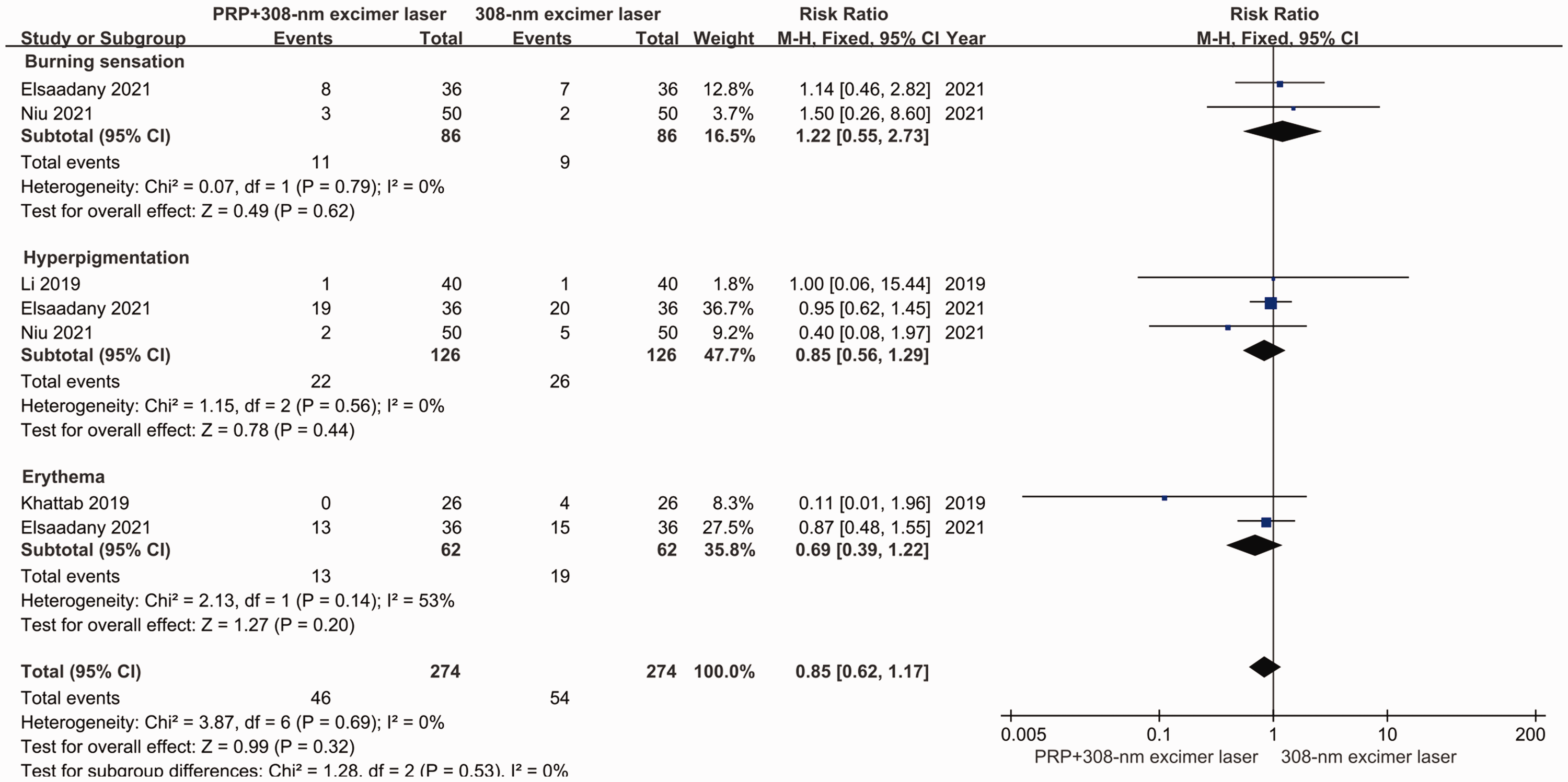
Rates of adverse events.
Recurrence
Three studies16,17,19 used the recurrence rate as one of the criteria for determining efficacy. The pooled analysis demonstrated that patients treated with combination therapy had lower recurrence rates than did those who received monotherapy (RR = 0.36, 95% CI = 0.17–0.78, P = 0.009 [fixed model], I2 = 0%; Figure 6).

Recurrence rates.
Discussion
Vitiligo is an acquired depigmentation disease resulting from the loss of epidermal melanocytes, and this cosmetically disfiguring problem causes great psychological and social effects in patients.21,22 However, the management of vitiligo remains challenging, and a safe and effective treatment remains to be identified. 23 As recommended by current guidelines,24–26 the treatment options for vitiligo include topical steroids, calcineurin inhibitors, vitamin D, Janus kinase inhibitors, laser therapy, and surgery. Unfortunately, none of these monotherapies achieved satisfactory efficacy because of the unclear pathology of vitiligo and individual differences. Therefore, many guidelines25,26 and researchers27,28 have proposed the use of combination therapy, such as laser therapy (NB-UVB, excimer laser, photodynamic) combined with topical steroids, calcium inhibitors, or immunosuppressive agents to treat vitiligo.
The possible mechanism of PRP in vitiligo could involve the enhanced proliferation of keratinocytes and fibroblasts induced by growth factors. 29 PRP also increases the interaction between melanocytes and keratinocytes and inhibits the apoptosis of melanocytes. 29 PRP was used as an investigational treatment for vitiligo, but it has not been approved by the US Food and Drug Administration. It was reported that PRP monotherapy could initiate repigmentation in patients with vitiligo.18,30 However, reports16,31 indicated that the efficacy of PRP alone for locally stable vitiligo is unsatisfactory (only 20% of patients achieved >75% repigmentation). Previous studies32,33 reported that TGF-b1 in PRP can inhibit melanin synthesis by delaying the activation of extracellular signal-regulated kinases. Meanwhile, PDGF in PRP can also stimulate skin angiogenesis, collagen synthesis, and extracellular matrix formation, resulting in reduced pigmentation. 34 Thus, the efficacy of PRP in the treatment of depigmentation-related diseases remains controversial. Some research indicated that PRP, when applied adjunctively in combination with NB-UVB or CO2 laser therapy, can produce satisfactory efficacy in treating stable vitiligo.14,31 One of the six included articles found that the addition of intradermal PRP to 308-nm excimer laser therapy did not provide an additional benefit concerning the degree of repigmentation, patient satisfaction, and the frequency of adverse events in patients with vitiligo. 16 By contrast, the other five articles13,17–20 all found that PRP combined with 308-nm excimer laser therapy provided significantly better efficacy than 308-nm excimer laser therapy alone. The disagreement among the studies might be related to sample size differences and trial methods (randomized controlled methods). According to the current meta-analysis, the combination of PRP and 308-nm excimer laser therapy yielded remarkably better outcomes in patients with vitiligo than 308-nm excimer laser monotherapy. In particular, the rate of re-pigmentation (≥25%, ≥50%, ≥75%) and recovered area indicated the superiority of the combination therapy. In addition, PRP might exert a beneficial effect by decreasing the non-response rate of patients with vitiligo when added to 308-nm excimer laser therapy. Regarding the safety of the combination regimen, our systematic review demonstrated that combination therapy was well tolerated, with only a small proportion of patients experiencing mild adverse events. Encouragingly, our meta-analysis also suggested that the rates of adverse events were comparable between the combination therapy and monotherapy groups, and lower recurrence rates were recorded for combination therapy.
This meta-analysis had multiple limitations. First, the number of included studies was relatively small, especially in terms of the subgroup analysis. Second, some eligible studies did not clearly describe the blinding of patients and allocation concealment process, which may indicate a possible risk of bias. Third, the included patients were all from China or Egypt, which could make the conclusion of our meta-analysis less robust. Fourth, the duration of intervention was short (within 4 months), and there was a lack of data on long-term efficacy.
The current meta-analysis found that the combination of PRP and 308-nm excimer laser therapy was more effective in the treatment of vitiligo than 308-nm excimer laser monotherapy. According to the results of this meta-analysis and the present theoretical basis, the combination of PRP and 308-nm excimer laser therapy could be a promising treatment for vitiligo. As the use of PRP in the treatment of vitiligo is a novel concept, additional large-scale, well-designed RCTs must be performed in the future.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221119646 - Supplemental material for Meta-analysis of the efficacy of adding platelet-rich plasma to 308-nm excimer laser for patients with vitiligo
Supplemental material, sj-pdf-1-imr-10.1177_03000605221119646 for Meta-analysis of the efficacy of adding platelet-rich plasma to 308-nm excimer laser for patients with vitiligo by Jiaoquan Chen, Nanji Yu, Huaping Li, Yi Tang and Huilan Zhu in Journal of International Medical Research
Footnotes
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Natural Science Foundation of Guangdong Province (2019A1515011593).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.