
Abstract
Objective
To compare the efficacy of percutaneous ethanol injection (PEI) and radiofrequency ablation (RFA) for patients with hepatocellular carcinoma (HCC) of no larger than 5 cm.
Methods
The data used in this study were retrieved from the SEER database. In total, 3510 patients diagnosed with HCC of no larger than 5 cm who received PEI or RFA were included.
Results
The median overall survival (mOS) and median cancer-specific survival (mCSS) of RFA-treated patients were not significantly longer than those of PEI-treated patients either before or after propensity score matching (PSM). The subgroup analysis showed that patients with HCC of no larger than 2 cm, HCC of larger than 2 cm, American Joint Committee on Cancer (AJCC) stage I and II, and AJCC stage III and IV who received RFA had mOS and mCSS similar to those of patients who received PEI after PSM. Multivariable regression analysis showed that PEI did not increase the all-cause mortality risk or cancer-specific mortality risk after PSM.
Conclusion
RFA is still the better choice for patients with a single HCC of no more than 5 cm. However, PEI might be a good choice for these patients who cannot be treated with RFA.
Keywords
Introduction
Hepatocellular carcinoma (HCC) is one of the most common causes of cancer-related death worldwide.1,2 Approximately 780,000 new cases of HCC are diagnosed each year globally, and the incidence of HCC in the United States has increased during the last decade. 3 For patients with early HCC, radical treatments such as transplantation, hepatectomy, and radiofrequency ablation (RFA) are recommended. 4 The 5-year survival rate after hepatectomy is high because the tumor can be completely removed. However, some patients with HCC do not tolerate hepatectomy because of poor liver function or poor health conditions. Thus, RFA, a minimally invasive technology, has become more frequently applied to the treatment of early HCC. Several randomized controlled studies and meta-analyses have shown that RFA provides the same benefit as hepatectomy to patients with HCC with a tumor size not exceeding 2 cm while reducing the incidence of complications.5–7
Although the efficacy of RFA in the treatment of small HCC is very good, RFA is challenging to perform when the tumor is located near major vessels or other vital organs because the blood flow can dissipate the generated heat, leading to incomplete ablation. The technology of artificial ascites might represent a good treatment strategy for HCC localized near important organs. However, it might increase the risk of abdominal infection, limiting its use if the tumor is present in certain locations. Several other new technologies, such as cryoablation and microwave ablation, have also been used to treat early HCC and have provided encouraging results.8–11 Percutaneous ethanol injection (PEI) continues to be widely employed in HCC therapy because it is cost-effective and can reduce treatment-related damage.
PEI has been used to treat solid tumors for many years and is considered safe, efficacious, and cost-effective. PEI was also used in past decades in the treatment of patients with small HCC. 12 Several studies have shown that in patients with small HCC (one to three tumors, each 3 cm or less in diameter), RFA provides a better survival benefit than PEI.13–17 However, the difference in efficacy between RFA and PEI in patients with a single HCC no larger than 5 cm remains unclear.
Previous studies compared the efficacy of RFA and PEI in patients with two to three tumors no larger than 3 cm.18,19 However, they included few patients with a single tumor no larger than 5 cm, and these patients were not used as a subgroup in the analysis of the outcomes of RFA or PEI. Thus, the present study used the Surveillance, Epidemiology, and End Results Program (SEER) database to compare the efficacy of RFA and PEI in patients with a single HCC no larger than 5 cm.
Materials and methods
The data were extracted from the SEER database, which covers approximately 34.6% of the United States population. The SEER database routinely collects data on patient demographics, primary tumor site, tumor morphology, stage at diagnosis, first course of treatment, and follow-up status. Data extraction was accomplished using the SEER*stat software.
The reporting of this study confirms to the STROBE guidelines. 20 The study was approved by the ethics committee of the hospital. The requirement for patient consent was waived because the study used the SEER database. However, the data used in the study were approved by the SEER program (reference ID: 12577-Nov2019).
The inclusion criteria were a diagnosis of primary HCC from 2004 to 2015 (ICD-O-3, code 8170/3-8175/3, site code C220), age of 30 to 84 years at the time of diagnosis, the presence of a single tumor of no larger than 5 cm, treatment with RFA or PEI, and complete data on the survival time (patients with a survival code of 0 or unknown survival were excluded) (Figure 1).

Flowchart of patient selection. PEI, percutaneous ethanol injection; RFA, radiofrequency ablation.
Endpoint definitions
The endpoints of the study were overall survival (OS) and cancer-specific survival (CSS). OS was defined as the time from HCC diagnosis to death. CSS was defined as the time from HCC diagnosis to death caused by cancer.
Statistical analysis
All statistical analyses were conducted using IBM SPSS Statistics for Windows, Version 24.0 (IBM Corp., Armonk, NY, USA) and GraphPad Prism 8.0 software (GraphPad, San Diego, CA, USA). The categorical baseline variables were compared between the two groups using the chi-square test and Fisher’s test. Survival curves were plotted using the Kaplan–Meier method, and differences in survival were determined by the log-rank test. A Cox regression risk model was used to predict the factors affecting OS and CSS of patients in both groups. To reduce collinearity, all characteristics were included in the multivariable regression analysis.
Propensity score matching (PSM) was performed to reduce selection bias and potential confounders. PSM included age at diagnosis, sex, year of diagnosis, summary status, grade, American Joint Committee on Cancer (AJCC) stage, tumor size, marital status, chemotherapy, and radiotherapy; 1:5 ratio matching was used, and 872 patients were matched. The optimal caliper was set at 0.1. After PSM, all characteristics were balanced between the two groups.
Results
Patients
After application of the inclusion criteria, this study involved 3510 patients treated with PEI (n = 190) or RFA (n = 3320). After PSM, 872 patients were included in the survival analysis (190 were treated with PEI and 682 with RFA) (Table 1).
Baseline characteristics of patients before and after PSM.

Data are presented as number of patients.
PSM, propensity score matching; PEI, percutaneous ethanol injection; RFA, radiofrequency ablation; AJCC, American Joint Committee on Cancer.
Survival outcomes
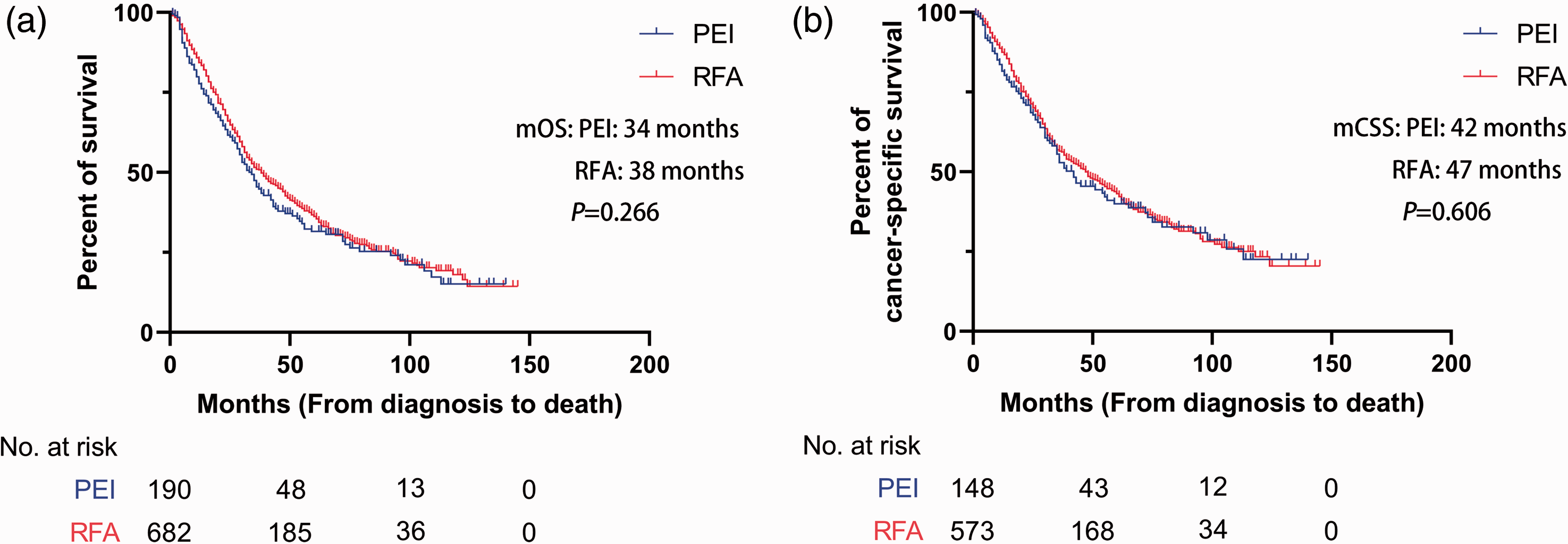
Before PSM, the median OS (mOS) of patients in the RFA group (41 months; 95% confidence interval (CI), 38.6–43.4) was slightly longer than that of patients in the PEI group (34 months; 95% CI, 28.5–39.5), but the difference did not reach statistical significance (Figure 2). Similar results were obtained after PSM; the mOS of patients in the RFA group (49 months; 95% CI, 45.8–52.2) was slightly longer than that of patients in the PEI group (42 months; 95% CI, 29.5–54.5), but the difference was not statistically significant (Figure 3).

Kaplan–Meier curves for overall survival and cancer-specific survival before propensity score matching. (a) Kaplan–Meier curve for overall survival and (b) Kaplan–Meier curve for cancer-specific survival.
Kaplan–Meier curves for overall survival and cancer-specific survival after propensity score matching. (a) Kaplan–Meier curve for overall survival and (b) Kaplan–Meier curve for cancer-specific survival.
Outcomes of multivariable regression analysis
The multivariable regression analysis before PSM showed that PEI did not increase the all-cause mortality risk (hazard ratio (HR), 1.138; 95% CI, 0.949–1.364) or cancer-specific mortality risk (HR, 1.068; 95% CI, 0.856–1.331) compared with RFA. Similar results were obtained after PSM. PEI did not change the all-cause mortality risk (HR, 1.150; 95% CI, 0.940–1.407) or cancer-specific mortality risk (HR, 1.106; 95% CI, 0.867–1.473) compared with RFA (Table 2).
Multivariable regression analysis of overall survival and cancer-specific survival before propensity score matching.

OS, overall survival; CSS, cancer-specific survival; HR, hazard ratio; CI, confidence interval; AJCC, American Joint Committee on Cancer; RFA, radiofrequency ablation; PEI, percutaneous ethanol injection.
Outcomes of subgroup analysis
Before PSM, for patients with a tumor no larger than 2 cm, survival after RFA (mOS, 56 months; 95% CI, 49.3–62.7 and mCSS, 74 months; 95% CI, 59.2–88.8) was significantly longer than that after PEI (mOS, 33 months; 95% CI, 26.1–39.9 and mCSS, 36 months; 95% CI, 24.6–47.4) (P = 0.002 and P = 0.007, respectively). For patients with a tumor of 2 to 5 cm, survival after RFA (mOS, 36 months; 95% CI, 33.7–38.3 and mCSS, 42 months; 95% CI, 38.6–45.4) was not significantly longer than that after PEI (mOS, 34 months; 95% CI, 27.3–40.7 and mCSS, 42 months; 95% CI, 25.3–58.7). For patients with AJCC stage I and II cancer, survival after RFA (mOS, 42 months; 95% CI, 39.5–44.5 and mCSS, 51 months; 95% CI, 47.2–54.8) was not significantly longer than that after PEI (mOS, 35 months; 95% CI, 28.8–41.2 and mCSS, 42 months; 95% CI, 30–54). For patients with AJCC stage III and VI cancer, survival after RFA (mOS, 22 months; 95% CI, 14.5–29.5 and mCSS, 26 months; 95% CI, 17.4–34.6) was not significantly longer than that after PEI (mOS, 9 months; 95% CI, 6.2–11.8 and mCSS, 9 months; 95% CI, 6.4–11.6) (Figure 4).
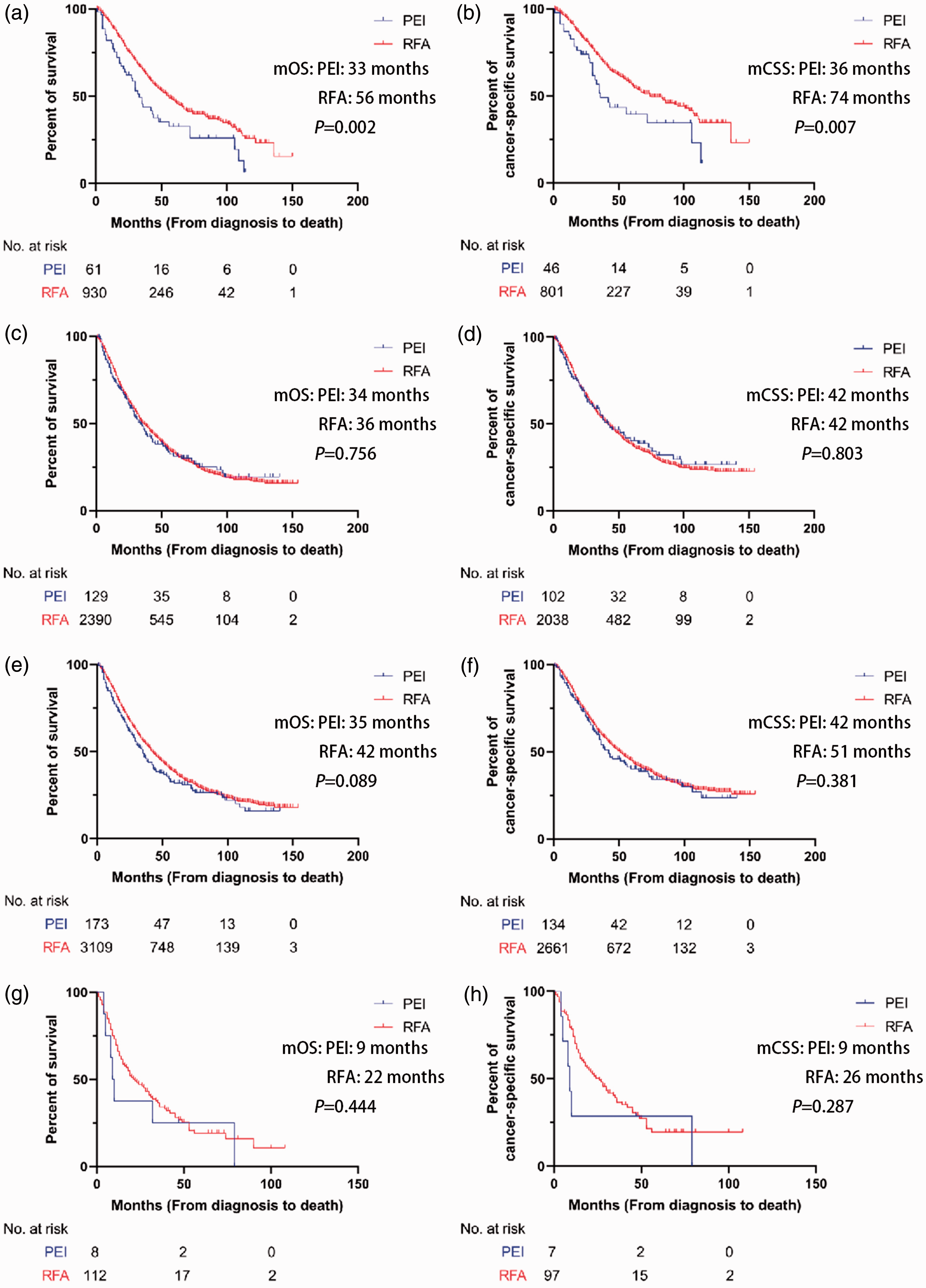
Kaplan–Meier curves for overall survival and cancer-specific survival in subgroup analysis before propensity score matching. (a, b) Kaplan–Meier curves for overall survival and cancer-specific survival of patients with tumors of no more than 2 cm. (c, d) Kaplan–Meier curves for overall survival and cancer-specific survival of patients with tumors larger than 2 cm. (e, f) Kaplan–Meier curves for overall survival and cancer-specific survival of patients with AJCC stage I and II cancer and (g, h) Kaplan–Meier curves for overall survival and cancer-specific survival for patients with AJCC stage III and IV cancer.
After PSM, for patients with a tumor no larger 2 cm, survival after RFA (mOS, 45 months; 95% CI, 32.6–57.4 and mCSS, 61 months; 95% CI, 46.3–75.7) was not significantly longer than that after PEI (mOS, 33 months; 95% CI, 26.1–39.9 and mCSS, 36 months; 95% CI, 24.6–47.4). For patients with a tumor of 2 to 5 cm, survival after RFA was not significantly longer than that after PEI (mOS, 34 months; 95% CI, 28.9–39.1 and mCSS, 44 months; 95% CI, 36.6–51.4). For patients with AJCC stage I and II cancer, survival after RFA (mOS, 39 months; 95% CI, 33.3–44.7 and mCSS, 48 months; 95% CI, 39.4–56.6) was not significantly longer than that after PEI (mOS, 35 months; 95% CI, 28.8–41.2 and mCSS, 42 months; 95% CI, 30–54). For patients with AJCC stage III and VI cancer, survival after RFA (mOS, 30 months; 95% CI, 13.3–46.7 and mCSS, 28 months; 95% CI, 16.2–39.8) was not significantly longer than that after PEI (mOS, 28 months; 95% CI, 16.2–39.8 and mCSS, 14 months; 95% CI, 0.0–47.8) (Figure 5).

Kaplan–Meier curves for overall survival and cancer-specific survival in subgroup analysis after propensity score matching. (a, b) Kaplan–Meier curves for overall survival and cancer-specific survival of patients with tumors of no more than 2 cm. (c, d) Kaplan–Meier curves for overall survival and cancer-specific survival of patients with tumors larger than 2 cm. (e, f) Kaplan–Meier curves for overall survival and cancer-specific survival of patients with AJCC stage I and II cancer. (g, h) Kaplan–Meier curves for overall survival and cancer-specific survival for patients with AJCC stage III and IV cancer.
Discussion
Radical treatment is recommended for HCC of no larger than 5 cm that does not invade lymph nodes or metastasize to distant organs. 4 RFA is considered the first-line treatment for patients with tumors no larger than 2 cm. 4 However, some studies have shown that patients with HCC of 3 to 5 cm who are not suitable for surgery can obtain survival benefits from RFA as well as from PEI. However, few studies have compared the efficacy of RFA and PEI in patients with HCC of no larger than 5 cm. Therefore, the present study was conducted to compare the outcomes of patients treated with RFA and PEI using population-based data.
The European Association for the Study of the Liver guidelines state that PEI can be an alternative to RFA in the treatment of HCC no larger than 2 cm because it can trigger complete necrosis in 90% of tumors smaller than 2 cm.4,14,21 However, the current analysis showed that patients with a single tumor no larger than 5 cm do not gain an additional survival benefit from RFA compared with PEI. A previous study showed that patients with small HCC (three or fewer tumors, each with a diameter not exceeding 3 cm) who received RFA had a lower mortality risk than patients treated with PEI. 22 Another investigation compared the outcomes in patients treated with PEI, high-dose PEI, and RFA and showed that RFA provided the most significant survival benefit. 23 In the present study, PEI-treated patients with tumors no larger than 2 cm had survival benefits similar to those of patients treated with RFA. The results of the current work are similar to the findings of Yu et al., 13 who analyzed 535 patients with early HCC and compared the efficacy of PEI and RFA. Using multivariate Cox regression analysis, they found that PEI did not increase the mortality risk compared with RFA (HR, 1.690; 95% CI, 0.828–3.449) in patients with HCC of no larger than 2 cm.
A study of patients with HCC of 1.5 to 3.0 cm showed that RFA increased the 1-year complete response rate but did not provide a survival advantage compared with PEI. 19 The current study compared the efficacy of RFA and PEI in patients with HCC of 2 to 5 cm in size and showed that patients receiving RFA had mOS and mCSS similar to those of patients receiving PEI. This result was obtained before and after PSM. However, the emergence of multipolar ablation needles has improved the efficacy of RFA in patients with larger tumors. Similarly, multiple injections of ethanol into the tumor can also ensure good efficacy in patients with larger tumors, which might be one reason for the survival of PEI-treated patients with tumors of 2 to 5 cm being similar to that of RFA-treated patients. Another reason might be that RFA can completely destroy the tumor (no more than 2 cm), but PEI can diffuse to all the tumor, which might lead to better efficacy for tumors of no more than 2 cm treated by RFA than PEI. However, incomplete ablation may occur in some patients with tumors larger than 2 cm. Incomplete ablation can lead to tumor recurrence and a poor prognosis, which might explain why patients with liver tumors of 2 to 5 cm achieved similar survival from PEI as from RFA. The current study also compared the efficacy of PEI and RFA in patients with early HCC (AJCC stages I and II) and advanced HCC (AJCC stages III, IV, and unknown) and showed that survival was similar after both types of treatment. However, the number of patients with advanced HCC was small, necessitating confirmation of this conclusion in a study with a larger sample size.
A multivariable regression analysis was conducted to eliminate the contribution of variables not related to the type of treatment. All variables were included in the multivariable regression analysis to reduce collinearity. The results showed that patients in whom HCC was diagnosed at an earlier time had a higher all-cause mortality risk and cancer-specific mortality risk. Moreover, patients with a larger tumor size had a higher all-cause mortality risk before and after PSM, a finding also reported in prior studies. A potential reason for these findings is the emergence of new drugs, such as sorafenib and lenvatinib, and the development of surgical technology and modification of surgical methods.24,25 After eliminating other potential variables that might affect OS and CSS, the all-cause mortality risk and cancer-specific mortality risk were similar in RFA- and PEI-treated patients both before and after PSM. The results of the multivariable regression analysis showed that among patients with a single HCC tumor no larger than 5 cm, OS and CSS were similar between patients who received PEI and those who received RFA.
This study has several limitations. First, the retrospective nature of the study might have resulted in selection bias; however, the use of PSM reduced this effect. Second, the patients’ liver function and physical condition were not included in the analysis because this information is not available in the SEER database. Finally, the number of patients with intermediate and advanced HCC was small, which affected the reliability of the results of the subgroup analysis. We hope that future studies will include these factors and recruit more patients with intermediate and advanced HCC to confirm the validity of the conclusions of the present work.
Conclusion
RFA is still the better choice for patients with a single HCC of no more than 5 cm. PEI-treated patients with an HCC tumor of no larger than 5 cm have OS and CSS similar to those of RFA-treated patients. Thus, PEI might be a good choice for patients who are unsuitable for or unwilling to receive RFA.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221111281 - Supplemental material for Efficacy of percutaneous ethanol injection versus radiofrequency ablation for single hepatocellular carcinoma no larger than 5 cm
Supplemental material, sj-pdf-1-imr-10.1177_03000605221111281 for Efficacy of percutaneous ethanol injection versus radiofrequency ablation for single hepatocellular carcinoma no larger than 5 cm by Ping Yang, Ningjie Li in Journal of International Medical Research
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.