
Abstract
In this scoping review, we aimed to evaluate the effectiveness of integrated multidisciplinary team discharge planning and identify common outcomes among older adults with complex needs, focusing on a safe transition from the hospital to the community. We performed a literature search for relevant articles using seven electronic databases and agreed search terms. Only articles published in English were included. In total, 23,772 articles were identified, with 27 articles meeting the inclusion criteria. A preponderance of patients aged ≥65 years and women was inferred based on population demographics. Initiatives on complex discharge planning were noted across most Western countries. Common outcomes of complex discharge planning were functionality (n = 11) including frailty (n = 4), quality of life (n = 11), and patient-centered factors including psychosocial needs (n = 9). Various outcomes from complex discharge planning initiatives and pathways were explored in this scoping review. None of the selected studies covered all nine domains of outcome assessment. Further research is needed involving follow-up studies after complex discharge planning interventions to assess their true effectiveness or value.
Keywords
Introduction
According to the World Health Organization (WHO), the global population comprises 14% older adults, and this group is expected to increase to 1.4 billion by 2030 and 2.1 billion by 2050. 1 With growth in this population, older adult patients account for a main proportion of the admissions to acute care hospitals worldwide. 2 Factors influencing admissions include frailty (4%–59%), with varying prevalence of multimorbidity (55%–98%).3,4 To achieve a successful discharge outcome, the WHO Guidelines on Integrated Care for Older People recommend an integrated multidisciplinary team (MDT) care approach wherein complex discharge planning (CDP) measures are adopted to ensure the fulfillment of all care needs. 5
Discharge planning forms an integral part of an effective inpatient care plan, especially in frail older adults with complex needs. Its efficiency is reflected in the quality of care that the patient receives and a reduced rate of readmission. 6 In Ireland, statistical data from an independent expert review on delayed discharge (2016–2018) reported that nearly 90% of older adult patients have delayed discharge. 7 To address common medical and social complexities in older adult patients, integrated care guidance from the Health Service Executive, alongside the Integrated Care Programme for Older People, emphasizes early MDT involvement through streamlining transition and discharge processes.8,9 This is to deliver high-quality and safe care, improving patients’ quality of life (QOL) and their outcomes. 10
The term CDP loosely refers to the process whereby hospital teams develop an integrated care plan addressing both health and social care needs. 11 Several initiatives have been implemented to address CDP worldwide that have been demonstrated to reduce emergency department (ED) readmissions in older adults. These most notably include United Kingdom (UK) policies in the Community Care [Delayed discharge] Act (CCDA), Canada’s categorization pathway of individuals with complex needs as an Alternative Level of Care, the Better Outcomes for Older people through Safe Transitions (BOOST) initiative in the United States (US), Australia's policy derivative on a delayed discharge patient placement pathway with an escalation protocol, and Sweden’s complex iterative strategy using a six-step intervention mapping protocol.12–16
Whereas the existing literature discusses initiatives and interventions around discharge processes aimed at resolving complex needs, few have reported outcome measures assessing the efficacy of the proposed interventions. With advancement in age, there is an anticipated increase in associated multi-morbidity levels. 17 This gives rise to poor outcomes if complex needs are unaddressed. Outcome measures remain underexplored, such as those focusing on mortality, functionality, discharge location, reduction in length of stay (LOS), readmission, and other patient-related outcomes. 18 Some studies, particularly in the ED, only review hospital service outcomes, such as reducing LOS and readmission. 19 One systematic review showed discordant results in studying the effects of QOL among frail older adults owing to the heterogeneity of interventions and study designs. 20
In the present scoping review, we sought to summarize outcomes of CDP in the older adult population and identify gaps for future research considerations.
Methods
This protocol was retrospectively registered on the International Platform of Registered Systematic Review and Meta-analysis Protocols (INPLASY) on 20 May 2022 (Registration number INPLASY202250127. https://inplasy.com).
Objectives
We conducted a scoping review using the five-stage framework proposed by Arksey and O’Malley, 21 and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis extension for Scoping Reviews (PRISMA-ScR) 22 was used to guide the reporting.
In this scoping review, we aimed to summarize the current literature on (a) Discharge pathways or initiatives in place for CDP; and (b) patient outcomes associated with CDP across nine domains.
The research questions in our scoping review were as follows.
What discharge initiatives or pathways are in place for older adults with complex discharge needs that encompass all nine domains of outcome assessment? Are there follow-up studies assessing the impact or providing outcome evaluation of CDP initiatives or pathways?
Search strategy
We carried out a literature search for relevant articles published between November 2021 and January 2022 across key electronic databases including MEDLINE (EBSCO interface), MEDLINE (Ovid interface), CINAHL (Complete interface) CINAHL (EBSCOHost interface), EMBASE (Ovid interface), Web of Science, and Scopus. To avoid the potential inclusion of older and less relevant articles relative to the current health care system, articles were included if they focused on acute hospital settings, older adult populations, complex discharge planning, and were published within the selected 20-year window. Furthermore, only articles published in English were included. Study designs including quantitative and qualitative methods were considered. Posters, conference abstracts, editorial opinions, grey literature, integrated reviews, systematic reviews, and scoping reviews were excluded. The full-text article was assessed if no abstract was available; likewise, the abstract was reviewed if the full-text article was not available. Key search terms used included elders and complex discharge OR elders and complex discharge unit OR elders and frail and complex discharge OR elders and complex discharge planning OR elders and failed discharge OR elders and complex discharge and outcomes OR complex discharge planning and elder outcomes.
Article selection
Articles meeting all the inclusion criteria were deemed eligible for review. The inclusion criteria were as follows: 1) patients aged 65 years and older in the acute hospital setting; 2) delayed discharge from the acute hospital setting to home or intermediate care; 3) peer-reviewed articles focusing on CDP, complex discharge units, LOS, or the impact of delayed discharge; 4) published between January 2001 and December 2021; and 5) discharge strategies to improve patient outcomes.
The exclusion criteria were: 1) patients aged below 65 years; 2) articles not published in the English language; 3) patients admitted for elective cardiology interventions or surgical or vascular or orthopedic procedures or patients who were post-stroke and receiving rehabilitation; 4) patients admitted under psychiatry or oncology services; and 5) patients escalated to the intensive care unit (ICU) with a protracted ICU course and who later died.
We conducted the database search using an agreed search strategy. To determine eligibility, both reviewers examined the titles and abstracts of all articles identified in the search. The full text or abstract of articles deemed suitable for further review was independently examined by the reviewers. In the event of any disagreement in article selection, a consensus was reached between the reviewers using a nominal group technique in weekly face-to-face meetings.
Data extraction and charting
Standardized data extraction forms developed by the team were created using Microsoft Word (Supplemental Table 1). Relevant information in the form included: 1) article title, author information, publication year, and country of publication; 2) study aims, design, methods, and reported impact; and 3) outcome measures. Both reviewers independently collected the data using an iterative approach and compared them. Consensus meetings were held, and decisions were finalized through discussion.
Data sorting, summarizing, and reporting
A quality appraisal was not conducted owing to the nature of a scoping review. Outcomes of CDP were categorized to identify gaps in the existing research. A summary of relevant findings was tabulated by first author and year, country, study design, population characteristics, sample size, identified complex needs prolonging hospital stay, initiatives or pathways in CDP, and their outcomes (Table 1). Data were analyzed using a content analysis approach by applying appropriate responses to the stated research questions.
Characteristics of eligible studies.

ADL; activities of daily living; RCT, randomized controlled trial; QOL, quality of life; SPeED, Supported Patient-centered Early Discharge; US, United States; UK, United Kingdom; NR, not reported, ED, emergency department; LOS, length of stay; CFS, Clinical Frailty Scale; IMDP, Integrated Model for Discharge Planning; CCC, continuity of care center; BRASS, Blaylock risk assessment screening score; ML, machine learning; EDPP, Enhanced Discharge Planning Program; MDT, multidisciplinary team; ACTION, Aged Care Transition; CGA, comprehensive geriatric assessment; LiSat-11, Life Satisfaction Questionnaire -11; REFS, Reported Edmonton Frail Scale; GEDI, geriatric emergency department intervention.
Results
Characteristics of the included studies
The initial literature search generated 23,772 potential articles, of which 82 were duplicates and 23,570 were excluded after screening the titles and abstracts and according to the inclusion and exclusion criteria. Upon full-text assessment of 120 articles, 27 studies were included in the final scoping review for data extraction regarding study aims, design, methods, origin of the study, participant characteristics, sample size, and outcome data. The selection process is represented in the PRISMA-ScR flow chart (Figure 1).
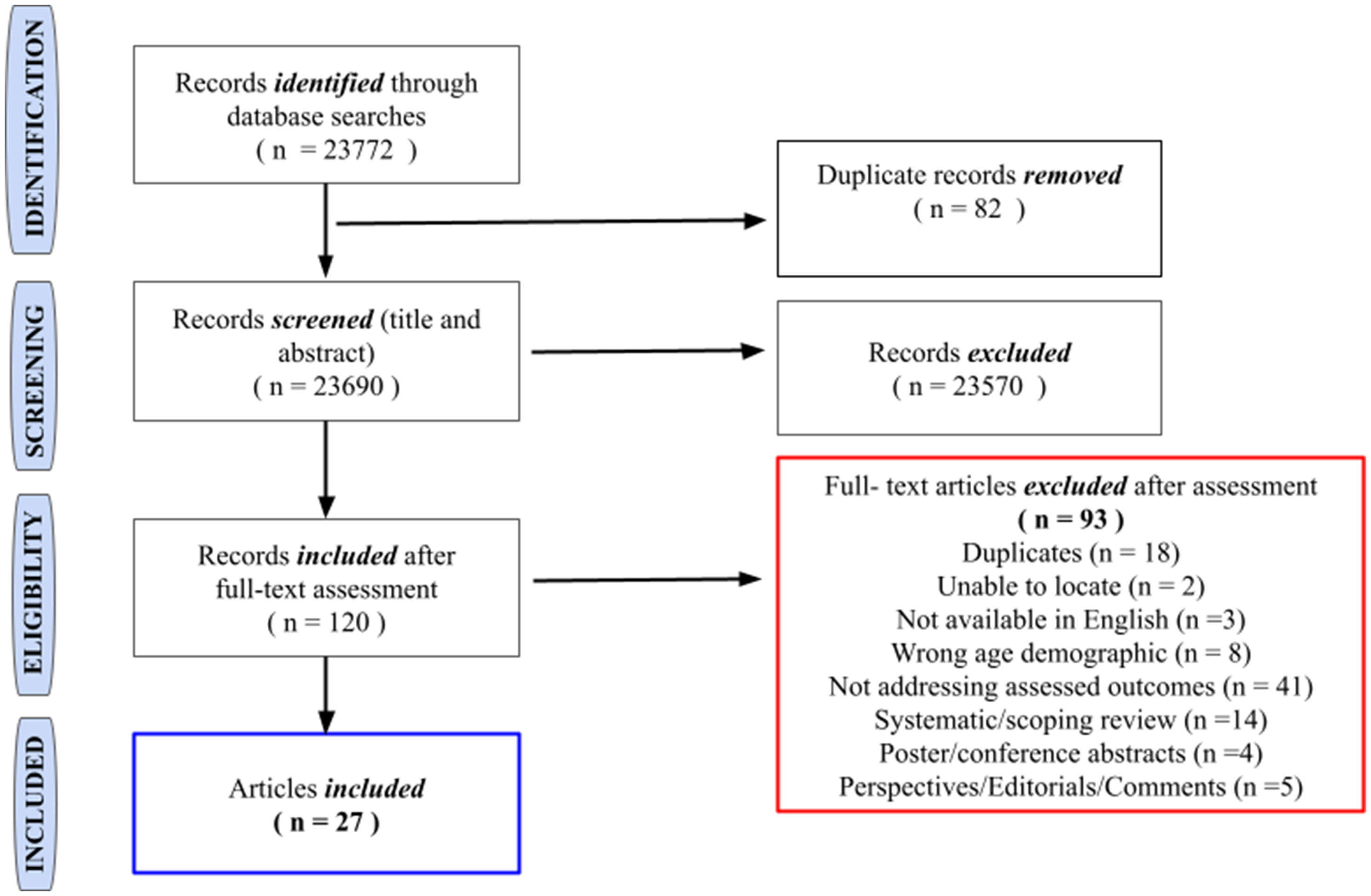
Preferred Reporting Items for Systematic Reviews and Meta-Analysis extension for Scoping Reviews (PRISMA-ScR) flow chart.
Eligible articles included in the scoping review were studies published between 2001 and 2021, with most published in 2015. Most studies were conducted in Norway (n = 5),23–27 followed by Australia (n = 4),28–31 Sweden (n = 4),32–35 Canada (n = 4),36–39 the US (n = 3),40–42 Singapore (n = 2),43,44 and one study each was conducted in Denmark, Ireland, Italy, Netherlands, and the UK.45–49 (Table 1).
Most studies (n = 23)23–25,27,29–40,42–47,49 were conducted in urban acute care hospital settings including university teaching hospitals (n = 9),23,27,29,32,36,37,46,47,49 academic medical centers (n = 1), 40 skilled nursing facilities (n = 1), 41 and geriatric rehabilitation facilities (n = 2).39,48 Some studies involved collaboration between community acute care hospitals in rural regions (n = 6).23,26,27,33,36,37 The sample size varied among studies, from 10 to 163,983 participants, depending on the study design.
The selected articles mostly reported quantitative studies including cohort-based studies (n = 8),39,41–43,46–49 observational studies (n = 2),33,34 and cross sectional studies (n = 3).24,25,32 We identified more prospective studies (n = 6)39,41,42,46–48 than retrospective studies (n = 2).43,49 The remaining articles described case studies (n = 4),23,27,28,37 randomized controlled trials (RCTs) (n = 3),35,40,45 quasi-experimental trials (n = 2),29,44 and a population-based study, 36 prospective non-RCT with blinded outcome evaluation, 30 comparative process evaluation, 26 predictability and prognostication analysis, 38 and a study protocol. 31
A preponderance of participants aged ≥ 65 years and women was inferred based on population demographics. Only nine articles discussed diagnoses leading to patient hospitalization. The most common diagnosis involved cardiac (n = 5),27,32,37,42,48 respiratory (n = 3),27,32,42 or gastrointestinal conditions (n = 2),24,32 acute confusion or delirium, 46 infection, 42 falls or general decline, 46 and cerebrovascular, 37 genitourinary, 27 or chronic illness. 23 One article, divided the admitting diagnosis according to an oncological versus a non-oncological diagnosis. 47 Another article categorized patients according to elective versus emergency admissions. 40 The remaining articles did not disclose details of the admitting diagnoses.26,28–31,33–36,38,39,41,43–45,49
Complex discharge planning initiatives and pathways
Seven studies26,28,31,37,40,41,43 discussed initiatives or pathways for CDP among frail older individuals. One study discussed an Integrated Model for Discharge Planning (IMDP) activated by a continuity of care-centered team led by a discharge manager. Integrating members into the MDT and patient involvement in discharge planning resulted in the efficient utilization of resources while showing consideration regarding the opinions of older adult patients. 37 Another study discussed the implementation of a dedicated allied health rapid discharge team, known as the Supported Patient-centered Early Discharge (SPeED) initiative, to extend rapid complex discharge programs for older patients across a broad cohort of conditions. To balance patient-centered care with optimal funding and organizational outcomes, this initiative provided an additional morale boost for staff in recognition of improved patient care. 28
One study was unique in that the researchers chose to implement intervention at the time of the patient’s presentation to the hospital. The geriatric emergency department intervention (GEDI) discussed in the study provided rapid targeted assessment and coordination of care with medical and allied health professionals, thereby reducing ED LOS while increasing the likelihood of safe discharge for residents of a residential aged care facility. 31
Two studies41,43 focused on transitional care needs. One study implemented an Aged Care Transition (ACTION) Program whereby dedicated care coordinators provided coaching to individuals and their families to enable better understanding of the medical diagnosis, the ability to effectively articulate their preferences, and self-management and care planning. This program helped to improve coordination and continuity of care and reduced rehospitalization and visits to the ED. 43 Another study involved an improving post-discharge transfer initiative, a multi-component intervention focused on transitional care and integration with a quality improvement tool to reduce potentially avoidable readmission. 41
One study chose to implement an enhanced discharge planning program (EDPP) post-discharge. The intervention included biopsychosocial assessment and an individualized plan following the program protocol. A telephone call at 30 days post-discharge from an experienced social worker had a positive impact on several important transitional care outcomes including home health services, medication management, and caregiver burden. 40 Only one study discussed the implementation of generic care pathways. The Patient Trajectory for Home-dwelling elders (PaTH) improved discharge arrangements and follow-up in primary care using checklists at defined stages in the patient trajectory. 26
Outcomes of complex discharge planning
Addressing complex needs through an individualized integrated care pathway is vital to achieving better discharge outcomes in older adults. Common outcomes across studies were functional outcomes (n = 11)28–30,39,42–46,48,49 including frailty (n = 4),9,42,46,49 QOL (n = 11),26,29,30,36,39,42–46,48 patient-centered factors including psychosocial needs (n = 9),23,24,27,33–35,37,40,49 economic factors (n = 6),28,31,32,43,44,47 medication management (n = 4),25,40,43,44 carer outcomes (n = 3),40,43,48 community services link-in (n = 6),26,29,31,40,43,44 follow-up (n = 6),26,29,40,43–45 and readmission (n = 8).24,25,28,29,38,40,41,45(Table 2). Although CDP processes were evaluated in most studies, none conducted a direct comparison of the outcomes of these processes in an acute hospital setting versus a subacute designated complex discharge unit. Only four studies mentioned the value of patient participation in CDP leading to an overall improvement in discharge outcomes. None of the included studies addressed all nine domains of outcome assessment.
Summary of outcomes from selected studies.
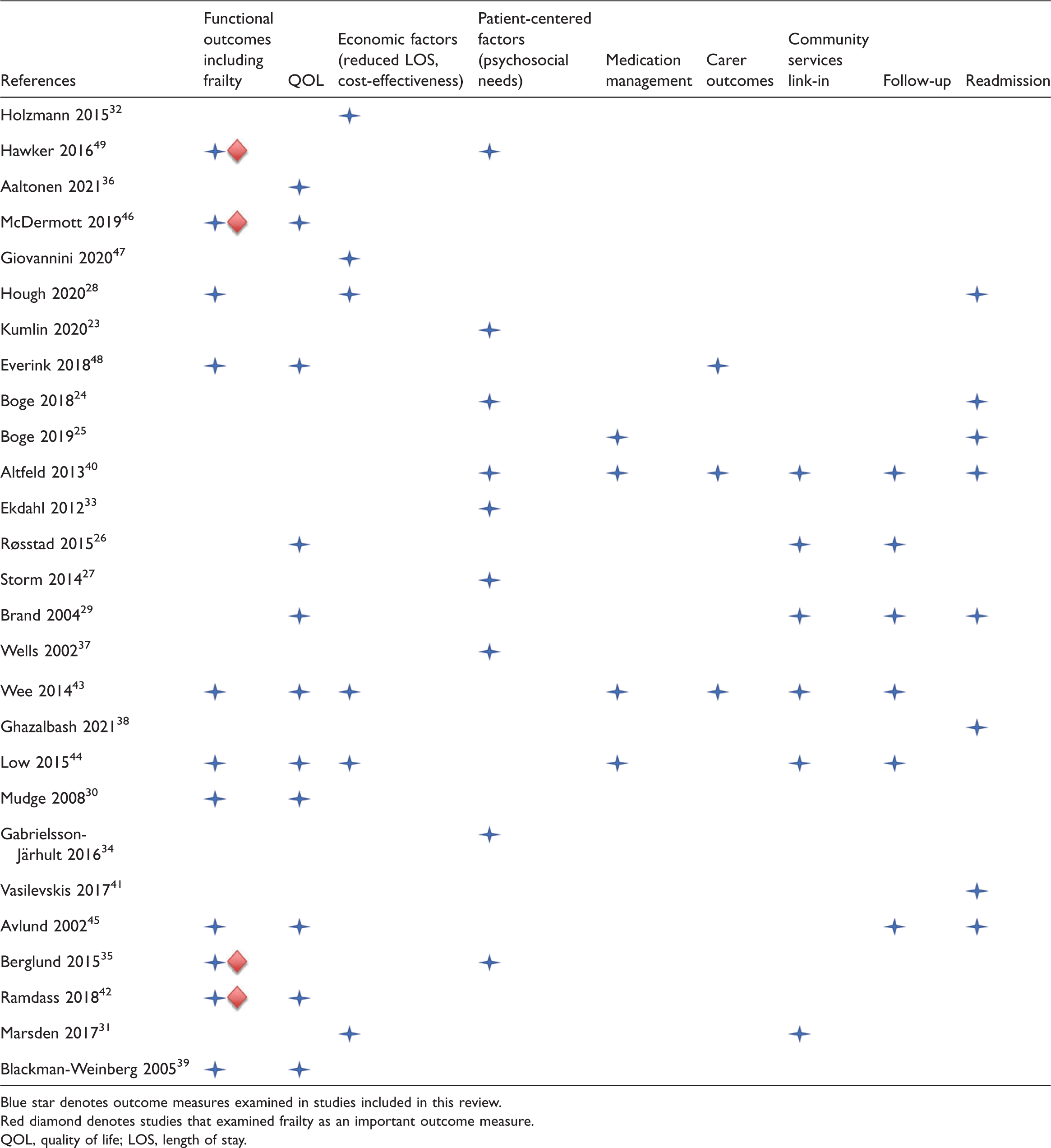
Blue star denotes outcome measures examined in studies included in this review.
Red diamond denotes studies that examined frailty as an important outcome measure.
QOL, quality of life; LOS, length of stay.
Functional outcomes
Multiple studies (n = 11)28–30,39,42–46,48,49 described functional outcomes as a determinant in the discharge process. Only seven articles exclusively discussed functional status among their outcome measures,28,30,39,43–45,48 and four studies discussed frailty.29,42,46,49
Frailty
Four articles29,42,46,49 were very similar in their definition of frailty: a multisystem, significant decline in physiological reserve in an older adult resulting in increased vulnerability to stressors.50–52 Frailty is a main cause of delayed discharge.29,42,46,49 Commonly used assessment tools to measure the efficacy of outcomes associated with frailty include the Reported Edmonton Frail Scale (REFS) and Clinical Frailty Score (CFS).42,46,49(Table 3). Whereas the REFS was reported to be practical, easy to administer, and useful in assessing multiple important geriatric domains, the CFS was considered helpful in predicting LOS and negative discharge outcomes.
Frailty and delayed discharge.

REFS, Reported Edmonton Frail Scale; TUAG, Timed Up and Go; CFS, Clinical Frailty Score; LOS; length of stay; RR, relative risk; CI, confidence interval.
Quality of life (QOL)
Other notable causes for delayed discharge included multimorbidity (n = 3),29,32,38 dementia (n = 1), 36 and QOL (n = 11).26,29,30,36,39,42–46,48 The manner in which the efficacy of outcomes from CDP was measured varied among studies. Assessment tools ranged from primary measures of independence in activities of daily living (ADL) using the Katz index (Katz-15 scale), with secondary measures to study pathway effects including the Frenchay Activity Index, 48 Barthel Index,30,39,42,44,45 functional independence measures, 28 and QOL assessed with the modified Cantril Self-Anchoring ladder (CSAL) scale, EuroQol EQ-5D scale,43,48 and Assessment of Quality of Life instrument. 26 One study used a minimum data set, which consisted of ADL elements in addition to cognition, psychosocial elements, and activity assistance level assessment scoring (University of Iowa Level of Assistance Scale) to evaluate patients’ discharge location goal. 39 Five studies 28,30,35,43,45 showed encouraging patient outcomes with involvement of an allied health Early Supported Discharge team, 28 with positive QOL and self-rated scoring post-discharge, 43 MDT- and Barthel score-associated functional improvement,30,45 and MDT-associated perceptual outcome. 35
In two studies, positive outcomes in ADL/QOL were not achieved after adjustment for baseline differences.29,48 Another study described positive outcomes in terms of integrated needs but suggested the need for an RCT to measure QOL outcomes of the transitional care program. 44 Two studies discussed longer LOS (days) in patients with severe frailty or dementia,36,46 and another study described using a multimorbidity predictor tool to facilitate discharge planning through prediction of mortality and readmission. 38 One study included functionality as part of their initiative (the PaTH checklist), choosing to focus primarily on pathway implementation, 26 and another article discussed multimorbidity in older adults as a factor affecting discharge from the ED. 32
Economic factors (reduced LOS, cost-effectiveness)
Delays in patient discharge were associated with negative outcomes and increased health care costs.31,32 Through care transition interventions, one study in Singapore reported SGD 3.4 million in savings from reduced readmissions over 6 months. 43 Similarly, another study in that country confirmed SGD 4.7 million in savings owing to reduced readmissions (5787 fewer bed-day costs saved SGD 4.87 million and 301 fewer ED admissions saved SGD 65,016). 44 One study did not explore cost-related savings but instead confirmed a lower median number of days considered “no advantage financially”, shorter LOS, and fewer readmissions within 30 days with their intervention (SPeED cohort). 28 Only one study reported a reduction in LOS from 33.3 ± 47.5 days during the first 3 months to 28.8 ± 39.5 days in the final 3 months of activity in a continuity of care center (CCC). 47
Patient-centered factors (psychosocial needs)
Patient participation in discharge planning and attitudes about self, disease, and discharge
Ten articles discussed the role of patient participation in CDP.23–25,27,33–35,37,40,49 One study noted patient and carer satisfaction when patients were allowed to assume a central role in discharge planning. 37 Conversely, another study described the passive position assumed by some patients surrounding decisions concerning changes in their health care or housing situation, in comparison with other patients who took charge of their situation and circumvented plans of hospital personnel and discharge process. 23 Patient care trajectories were largely determined by their level of trust in health personnel overseeing their care. One study acknowledged difficulties faced by patients with multimorbidity when participating in medical decision-making. 33 The vital role played by next of kin or carers was highlighted in another study, where a lack of information and preparedness for hospital discharge resulted in a risk of readmission and poorer discharge outcomes. 27 An additional study described how unanticipated problems occurred despite enhanced discharge care planning. 40 Problems with coordinating or accessing care from outpatient settings or community service providers, as well as the patient’s ability to cope with changes in health status and or mental health problems, were the most notable issues. Discharge quality monitored using the Discharge Care Experiences Survey (DICARES) in one study resulted in higher readmission scores for the factors “Coping after discharge” and “Adherence to treatment”; the lowest scores were reported for “Participation in discharge planning.”24,25
An observational study revealed three categories of concerns when managing life post-discharge: obtaining a secure living situation, need for continuous care and support, and influencing and regaining independence. Most patients expressed a desire to go back to familiar surroundings but were ambivalent in their ability to manage at home, feared becoming a burden to family members, and were dependent on support or facilities that they believed they could not financially afford. 34 In face-to-face interviews in an RCT using the validated Life Satisfaction Questionnaire-11 (LiSat-11), patients’ life satisfaction was more likely to be improved or maintained at 3, 6, and 12 months following comprehensive care intervention. 35
Vulnerable, frail older people living alone and loneliness
One study highlighted loneliness, living alone, and clinical frailty as factors associated with adverse discharge outcomes. There was a significant multivariate association between LOS and both self-reported loneliness (2.1%) and the CFS (1%), after adjusting for dementia and living alone. In a multivariate analysis, patients who lived alone were more likely to be readmitted to the hospital within 30 days (3.6%). 49
Medication management
Of the eligible articles, four studies emphasized medication safety as an important outcome measure.25,40,43,44 Three of these reported medication errors as contributing factors to complexities in discharge planning.25,40,44 Significant polypharmacy was reported in 68% of the older adult cohort in one study. 43 Another study included medication management using the DICARES-M, modified from their previous DICARES study.24,25 Initiatives such as ACTION, EDPP, and multidisciplinary transitional care plans incorporated medication management as integral factors.40,43,44 One study reported medication management issues in 16.4% of cases, with 10.6% warranting medication reconciliation. Compliance was achieved in 21.1% of patients post-intervention for medication compliance. 40
Carer outcomes
Carer stress was discussed in only three studies. Two studies reported that 20.9% 48 and 40% 43 of patients lacked informal carers at home. A prospective study assessed the efficacy of an integrated care pathway in a rehabilitation unit using a visual analog scale to determine the carer's self-rated burden. Secondary outcomes were measured using a modified CSAL and Erasmus School of Health Policy & Management instrument at baseline, 3 months, and after 9 months. An encouraging primary outcome was observed at 3 months, which faded with time. No difference was noted in the assessment of secondary outcomes. 48 Another study discussed carer stress as one of the vital components for enrollment in discharge planning initiatives; 34.4% reported a carer burden in an EDPP, but no significant difference was found in the control trial. 40 One study demonstrated a positive outcome of the ACTION program initiative. 43
Community services link-in
Six studies explored the importance of community service coordination.26,29,31,40,43,44 Three studies discussed initiatives such as an EDPP 40 and multidisciplinary transitional home care program, 44 with 34.2% and 23% of patients respectively assigned to appropriate care services and PaTH, 26 which improved collaboration with general practitioners (GPs). Interventions focusing on transition coordination services had 70% reduced 30-day readmission rates compared with 90% among controls. 43 An integrated GEDI model provided comprehensive geriatric assessment and discharge planning in the community or long-term care with relevant service referrals. 31 Another study discussed benefits of the integration of service coordination in the community through Chronic Disease Clinic/Chronic Disease Nurse Consultant assessment. 29
Follow-up
Follow-up outcomes were reported in six studies26,29,40,43–45 comprising RCTs (n = 2),40,45 quasi-experimental studies (n = 2),29,44 a retrospective study (n = 1), 43 and comparative evaluation with a normalized process theory framework (n = 1). 26 An additional four studies reported positive outcomes post-intervention.40,43–45 Post-discharge follow-up was reported at 30 and 60 days in one study 40 and at 3 and 6 months in a different study. 29 One quasi-experimental study discussed following up with patients a minimum of five times within the first 6 weeks. 45 Follow-up was mostly conducted via telephone (n = 3)26,40,43 and home visits (n = 3).26,43,45 Two studies reported that interventions such as ACTION and EDPP had a positive influence on hospital follow-up appointments.40,44 ACTION implementation, in particular, facilitated a 26.5% referral rate to specialist clinics. 44 One study reported that follow-up data gathered at 3 and 6 months reduced the risk for readmission post-intervention. 29 Furthermore, a comparative evaluation process was conducted using the PaTH initiative involving the hospital, and the corresponding GPs improved their primary care follow-up. 26
Readmission
Eight articles set readmission as their main outcome measure in discharge planning.24,25,28,29,38,40,41,45 Four studies assessed readmission at 30 days24,25,28,38 and another study at 3- and 6-month follow-up. 29 One prospective study reported that 35% of readmissions were avoidable according to root cause analysis. 41 Two trials showed no significant difference in readmission despite intervention implementation,40,45 with one case study reporting 14% fewer readmissions. 28 A predictability research study postulated the marker Charlson–Deyo Comorbidity Index as a strong determinant for readmission, 38 and a cross-sectional survey found no significant relationship between the patient’s experience and readmission, with 24.5% of patients readmitted within 30 days. 25 One quasi-experimental study reported no difference in readmission or the ED visit rate owing to issues arising from the application and appraisal of intervention. 29
Discussion
In this scoping review, we explored various outcomes of existing CDP initiatives and pathways worldwide. Overall, 27 articles met our inclusion criteria, after an exhaustive search of the literature. Although CDP processes were evaluated in most studies, there were no specific follow-up studies on outcomes after intervention or pathway implementation to assess their true effectiveness. Our scoping review is unique in that we discuss the importance of the nine domains of outcome assessment as being essential for successful patient discharge and transition to the community. These domains comprise functional outcomes including frailty, QOL, economic factors, patient-centered factors, medication management, carer outcomes, community services link-in, follow-up, and readmission.
It was evident in our scoping review that all nine domains of outcome assessment are closely interlinked and depend on each other to provide an ultimately positive outcome. Such robust outcomes can be achieved if the CDP pathway has a structure that allows for identification, assessment, initiation, appraisal, and review throughout all stages of CDP.
Common barriers to CDP observed in the articles examined in this scoping review were not solely confined to patient-centered factors. Barriers included a combination of administrative factors, community resources, and most importantly, effective communication between hospital teams and primary care teams to enable continuity of care post-discharge.37,40 Frailty and multimorbidity were the most commonly mentioned causes of delayed discharge leading to poor functional outcomes.29,32,35,36,39,42,43,46,49 All studies in our scoping review acknowledged longer LOS in moderately frail older adults as a result of fluctuation in their complex medical conditions and functional impairment. Greater emphasis must be placed on frailty scoring to serve as a guide in treatment intensity decisions and planning for the discharge destination. CDP is a process that must be initiated from the time of admission in at-risk older adults to permit physicians to anticipate and overcome potential barriers to discharge according to the nine domains of outcome assessment. Furthermore, early integrated involvement of MDTs can have a positive influence on functional independence and subsequent improvement in frailty among older adults, thereby reducing LOS. Functional independence through rehabilitation can be carried forward into the community with improved communication between allied health care resources and a wider availability of these resources.39,45
Although personalized integrated CDP and rehabilitation are proven to have positive outcomes, patients with moderate or severe frailty remain at risk of readmission and may require prolonged use of health care services in the community and follow-up. Psychosocial needs (anxiety, loneliness, depression), which form a vital part of CDP, are also recognized as factors that contribute to physical health. 53 Having an integrated liaison psychiatry team and medical social worker to streamline resources in the community would be invaluable to the continuity of care, not only from a psychiatric and psychosocial perspective but also to provide much-needed support to carers whose concerns are often overlooked.
With advancing age, multimorbidity, poor self-management, and unanticipated challenges post-discharge, patient adherence to medications can prove challenging. Initiatives such as ACTION, EDPP, and multidisciplinary transitional care plans are exemplary in the way they emphasize medication reconciliation as well as educate and raise patient awareness about medication safety, thus minimizing the risk of potential adverse events post-discharge.40,43,44 There should be more physician-directed care plans targeted toward reviewing the at-home or in-clinic setting post-discharge as well as community coordination of services to help minimize readmission.26,40,41 Communication has a critical role in ensuring that medications are effectively managed in the community; many older adults who re-present to the hospital often have missed medications or admit to polypharmacy as a result of lacking a clear understanding of their discharge prescriptions.40,43
With increasing numbers of older adults in long-term residential care settings, there is a need for improved collaboration between hospital physicians and their colleagues in skilled nursing and community-based physicians in an effort to reduce the number of preventable future readmissions. Better access to diagnostics in the community or educating staff to be more adept in managing acute conditions before escalating care to a secondary- or tertiary-level hospital should be further evaluated in future studies.
Additional research is needed with regard to measurement of QOL outcomes in transitional care programs. In our scoping review, we had difficulty delineating hospital-associated geriatric syndrome outcome measures. An important gap identified among the included studies is the lack of outcome measures in limiting cognitive and functional decline in hospitalized, frail older adults with dementia.
Strengths and limitations
The nine outcomes of CDP mapped in this scoping review will provide useful measurement tools for future researchers. We acknowledge the possibility that not all articles relevant to CDP outcomes were included in the final selection. Many studies were omitted because they included a younger cohort or because the data for adults aged ≥65 years were difficult to isolate in the results. It was challenging to examine outcomes worldwide owing to language bias. Furthermore, the differences in terminology regarding CDP and older adults varied between developed and developing nations, raising the question of what initiatives are implemented in developing nations.
There is a need for future research into experimental designs centered around strategies or interventions that encompass all nine outcome measures. Most included studies focused on certain outcomes in older adult patient cohorts, within a timeframe applicable to their respective studies. It would be interesting to see how outcomes differed if older populations were categorized into different age groups to identify at-risk populations, further refine current community resources, and evaluate how provision of better staff education and training affect functionality and QOL and influence hospital admissions among older adults.
Conclusion
In our scoping review, we clarified that with heterogeneity among the general population, a combination of the best intervention, effective communication, and integrated care pathways in CDP can provide optimal outcomes in older adult populations. However, it is important to note that a seamless transition of care upon discharge may be limited by available resources in the community in certain countries.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221110511 - Supplemental material for Outcomes of complex discharge planning in older adults with complex needs: a scoping review
Supplemental material, sj-pdf-1-imr-10.1177_03000605221110511 for Outcomes of complex discharge planning in older adults with complex needs: a scoping review by Puteri Maisarah Rameli and Nithya Rajendran in Journal of International Medical Research
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.